Effect of Transcranial Direct Current Stimulation on Balance and Stroke Specific Quality of Life in Stroke Patients
Stroke is the leading cause of disability which requires rehabilitation. It is defined as obstruction or restriction of blood supply to the brain, usually because a blood vessel supplying brain is burst or blocked by a clot; causing damage to the cells of brain. This in turn may result in physical and/or mental disabilities. Upper limb functions are most commonly impaired following stroke; which also deteriorates activities of daily living. tDCS is a novice approach which can improve upper limb function by modulating cortical neuronal excitability. Objective: To investigate the effect of cathodal, anodal and sham tDCS on balance and stroke specific quality of life in stroke patients. Method: 30 stroke patients meeting inclusion criteria were randomly allocated into three groups. Group A, B and C received cathodal tDCS, anodal tDCS and sham tDCS respectively. The intensity of the current was 2mA given for 20 minutes along with all the upper limb active and fine motor exercises. It was given for 12 sessions in 3 weeks. Berg balance scale and stroke specific quality of life questionnaire was taken to assess lower limb function respectively. It was taken before and after the 3 weeks. Result: paired t test showed that the balance improved before and after treatment with cathodal (0.003) and anodal (0.000) tDCS and sham stimulation (0.917) and also for SSQOL cathodal and anodal showed improvement in quality of life but sham stimulation showed no improvement. (0.173). Kruskal Wallis Test showed significant difference in between the groups (p<0.05) which showed balance improved more in anodal tDCS than cathodal and sham. Also cathodal tDCS balance compared to sham tDCS. but in SSQOL there was no significant improvement seen in all three groups. Conclusion: Both cathodal and anodal tDCS improve balance over sham tDCS. Improvement of balance with anodal tDCS was better than cathodal tDCS. There was no change in SSOL.
Introduction
Stroke is defined as the unexpected death of brain cells because of need of oxygen which is caused by obstruction of blood flow or break of an artery to the brain. There is gradually loss of speech, weakness or paralysis of one side of the body are the symptoms [1]. And therefore due to blockage there are mental and physical disabilities. There are around 15 million people according to WHO, who suffer from stroke each year in the world. According to world consensus, the second and fourth most causing stroke in patient is death and impairment. After 3 months there are approximately 56% stroke patients who recover their limb function (upper extremity and lower extremity).
Transcranial direct current stimulation (tDCS) device is a type of neurostimulation whose purpose is to use consistent low-level frequency current which is transferred by electrodes on the scalp. This device was used for helping patients who had injuries of brain or any psychiatric problems. It is a contemporary, portable, non-invasive, neuromodulatory technique that produces a low-level electric current to the head. The typically applied, fixed currents are 1 and 2 mA. In the device the constant current is produced by two electrodes and a battery powered device. Current has to enter and leave a given neuron to exert any physiological effects due to physical reasons. Thus, every neuron under the electrode will have depolarizing and hyperpolarizing effect. The anodal tDCS augments cortical activity and excitability. On contrary, the cathodal tDCS hyperpolarises the cortical resting potential membrane [2]. The effect of tDCS is analogous to that of the long term potentiation (LTP); which hastens the process of neuroplasticity. Hence it can augment the upper limb function along with rehabilitation.
Methods
30 Stroke patients were selected with inclusion criteria of one time stroke, above 18 years of age, MMSE score ≥ 24 and BBS score between 21-40 that is medium risk of fall. Patients with Traumatic brain injury or any injury to the brain, impaired skin over the placement of electrode which includes eczema, rashes, blisters, open wounds, burns and cuts, functional limitations due to musculoskeletal injuries, cognitive impairment, pacemaker, epileptic fit less than 1 year, intervertebral metal clip were excluded [3]. There were divided into three Groups with 10 patients in each Group. Treatment procedure was explained and a written informed consent was taken from each of them. Group A received cathodal tDCS, Group B received anodal tDCS and Group C received sham stimulation all along with conventional physiotherapy exercises. tDCS dosage was given at intensity of 2mA for 20 minutes with electrodes of area 25 cm². Lower limb exercises along with stimulation were hip, knee, ankle physiological movements. Conventional physiotherapy exercises included for reducing the spasticity of the muscles spastic muscles icing and stretching, mat exercises such as rolling, quadruped, kneeling, half kneeling along with reach outs and perturbations, balance and gait training. Treatment was given for 20 minutes, 4 days per week for 3 weeks [4, 5, 6, 7, 8].
Data Analysis and Interpretation
Statistical analysis was done using Wilcoxon Signed Rank test for Pre and Post test within the group and Kruskal Wallis test for comparing the groups (Figure 1).
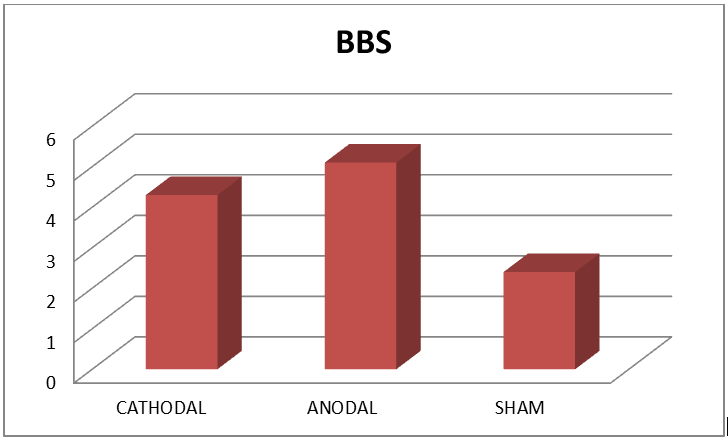
Interpretation: This represents there is significant difference in balance post treatment in groups A,B,C with p value 0.028 < 0.005. The mean difference is higher in Group B (5.1), then Group A (4.3) followed by Group C (2.4) [9, 10, 11, 12, 13]. Thus suggesting, anodal being more effective than cathodal and sham tDCS given with conventional exercises (Figure 2).
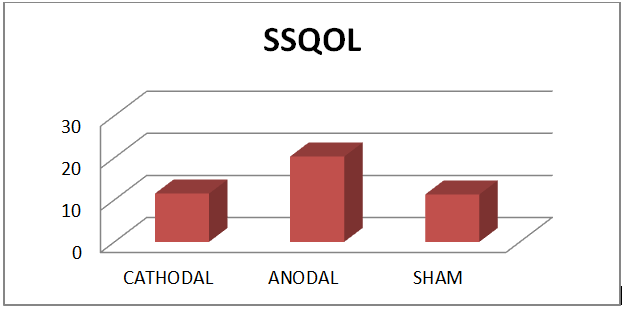
Interpretation: This represents there is no significant difference in quality of life in groups A,B,C with p value 0.539
> 0.005. The difference is higher in Group B (20.3), then Group A (11.5) followed by Group C (11.3). Thus suggesting anodal being more effective than cathodal and sham tDCS given with conventional exercise.
Results
In this study, 30 stroke patients were taken. The Group A, B and C has 10 each patients respectively. The Group A, B and C were given Cathodal, anodal and Sham tDCS respectively with conventional physiotherapy exercises [14, 15, 16, 17].
The normality of data was checked using Shapiro-Wilk Test. The data was not homogenous the P value being higher than 0.05.
By applying Wilcoxin Signed Rank Test and mean, shows statistical significance in balance in Group A, B and C. The mean difference was 4.3 ± 3.33, 5.1 ± 1.37 and 2.4 ± 1.07 for Groups A, B, C respectively. There is statistically significant improvement in Group B than compared to Group A and C. Also it is significant difference in Group A compared to Group C. The Chi square value is 18.83 and p value = 0.028. This states that there is significant improvement in balance in anodal tDCS followed by cathodal tDCS and then sham stimulation. There is a significant difference in the mean values in the Groups A, B, C, the p value < 0.05 .Thus anodal tDCS and cathodalt DCS and sham stimulation are effective in improving balance activities in stroke patients. Freidman test was used for the comparison between berg balance score in Group A, B and C.
By applying Wilcoxin Signed Rank Test and mean, shows statistical significance in stroke specific quality of life for Groups A, B, C. The mean difference was 11.5 ± 7.28, 20.3 ± 24.85 and 11.3 ± 24.15 for Group A, B and C respectively. There is a significant improvement in Group B than compared to Groups A and C. Also it is significant difference in Group A than compared to Group C. the p value = 0.539. Thus it states that there is no significant improvement in quality of life. The mean value difference is higher in Group B that is anodal tDCS. Thus, anodal tDCS, cathodal tDCS and sham stimulation are not effective in improving quality of life. Freidman test was used for the comparison between SSQOL in Groups A, B and C.
Discussion
This present research is done to compare the effect of transcranial direct current stimulation which is given with conventional physiotherapy in stroke patients. There was a significant improvement for balance with cathodal, anodal, sham stimulation along with physiotherapy exercises in stroke patients. But not much improvement was seen in stroke specific quality of life in cathodal, anodal and sham stimulation. The treatment was given for 12 sessions in 3 weeks. There was significant improvement in balance with anodal tDCS followed by cathodal tDCS and then followed by sham tDCS. For stroke specific quality of life there was no significant improvement seen. The lower limb function that is balance was checked by berg balance scale and quality of life which was checked by SSQOL before and after 3 weeks. Also there was no significant difference between dominant and non- dominant affected lower limb. Hyu-Kyu Cha, et al. said that it is hard for patients to recover after stroke. Stimulation by tDCS which is a non-invasive technique controls the purpose of neural structures which are not specific that makes the cortical excitability and its motor function better. He also stated that tDCS could enhance the function of balance and ADL which has been damaged. In this research the motor function of both the limbs and Activity Daily Living assessment had seen improvement in the experimental group. Together these study results suggested that tDCS along with conventional physiotherapy exercises provide an input to motor cortex. This study shows that there has been a significant increase of lower extremity function by giving tDCS stimulation and conventional physiotherapy in stroke patients which supports the above study. As by giving tDCS there is increase in the neuronal activity of the brain which promotes functional recovery of lower limb.
Wanalee Klomjai, et al. investigated if a single session of dual tDCS before physiotherapy would immediately benefit lower limb function. They compared tDCS and sham tDCS on the MVC of knee extensors and TUG and FISST scores in the similar patients. While comparing before and after no significant difference was found for sham group while for the actual tDCS group showed noticeably greater performance in TUG and FISST. Therefore, the study shows that there has been a significant improvement in balance when given anodal tDCS and cathodal tDCS than sham stimulation in stroke patients similar results were found in other researches. Eman Khedr, et al. in his study of effects of anodal and cathodal tDCS suggested that there has been no significant difference between anodal and cathodal tDCS effect, both effects had better improvement than compared to sham stimulation in the study. These effects were due to increase in cortical excitability and marginally increase in muscle strength in all 3 groups, and so improvement was also seen in lower limb function of the affected side. Jeffery in his study had found that anodal stimulation which was given at intensity of 1 mA had no effect on MEPs of lower limb. That was because the leg motor area is situated more inside than the arm area in the Primary Motor Cortex area. Therefore any anodal tDCS which is given at the intensity of 2mA shows improvement in leg EPs that is same as that of 40% increase in the improvement that is achieved by the hand MEPs at the intensity of 1mA. This study had also given anodal tDCS at the level of 2mA to increase the stimulation of the leg area of the Primary Motor Cortex.
The primary mechanism of tDCS on the cerebral cortex is a sub threshold modulation of neuronal resting membrane potential. Current has to enter and leave a given neuron to exert any physiological effects due to physical reasons. Thus, every neuron under the electrode will have depolarizing and hyperpolarizing effect. It modulates spontaneous neuronal network activity.
However in this study only stroke patients were included. Moreover the effect of dominance cannot be conclusive because of relatively small sample size within the group. Dominance plays important role in recovery of stroke and so should be studied separately.
The primary mechanism of tDCS on the cerebral cortex is a sub threshold modulation of neuronal resting membrane potential. Current has to enter and leave a given neuron to exert any physiological effects due to physical reasons. Thus, every neuron under the electrode will have depolarizing and hyperpolarizing effect. It modulates spontaneous neuronal network activity.
Conclusion
This research study concludes that improvement in lower extremity function had significant improvement on balance and stroke specific quality of life was improved with anodal stimulation than cathodal transcranial direct current stimulation. There was no as such improvement in sham tDCS for balance and stroke specific quality of life.
Acknowledgement
I would like to thank authorities of Dr. D Y Patil Vidyapeeth for allowing me to conduct this study by providing infrastructure and equipment. I would also like to thank all the participants of the study.
Conflict of Interest
There was no conflict of interest in this study.
References
-
Shiel CW (2017) Medical definition of stroke.
-
Cortical Homunculus: Nervous System.
-
Zimerman M, Heise KF, Hoppe J, Cohen LG, Gerloff C, et al. (2012) Modulation of Training by Single-Session Transcranial Direct Current Stimulation to the Intact Motor Cortex Enhances Motor Skill Acquisition of the Paretic Hand. Stroke 43(8): 2185-2191.
-
Ahmad SH, Mazhari S, Najafi K, Ahmadi M, Aghaei I (2018) Anodal transcranial direct current stimul;ation enhamces positive changes in movement function, visual attention and depression of patient with chronic stroke- A clinical trial. Biomedical Research and Therapy 5(11): 2841-2849.
-
O’Sullivan S, Schmitz T, Fulk G (2007) Physical rehabilitation. 6th (Edn.), Philadelphia: F.A.Davis.
-
(2017) The Anatomy of Movement Brain Connection.
-
Murphy T, Corbett D (2009) Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 10(12): 861-872.
-
Schjetnan AGP, Faraji J, Metz G, Tatsuno M, Luczak A (2013) Transcranial Direct Current Stimulation in Stroke Rehabilitation: A Review of Recent Advancements. Stroke Res Treat 2013: 170256.
-
Brunoni A, Nitsche M, Bolognini N, Bikson M, Wagner T, et al. (2012) Clinical research with transcranial direct current stimulation (tDCS): Challenges and future directions. Brain Stimul 5(3): 175-195.
-
Naros G, Geyer M, Koch S, Mayr L, Ellinger T, et al. (2016) Enhanced motor learning with bilateral transcranial direct current stimulation: Impact of polarity or current flow direction?. Clinical Neurophysiology 127(4): 2119- 2126.
-
Lindenberg R, Renga V, Zhu L, Nair D, Schlaug G (2010) Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology 75(24): 2176-2184.
-
Monfils M, Plautz E, Kleim JA (2015) In search of the Motor Engram: Motor Map Plasticity as a mechanism for encoding motor experience. Neuroscientist 11(5): 471- 483.
-
Techhio F, Zappasodi F, Assenza G, Tombini M, Vollaro S, et al. (2010) Anodal Transcranial Direct current stimulation enhances procedural consolidation. J Neurophysiol 104(2): 1134-1140.
-
Boggio P, Castro L, Savagim EA, Braite R, Cruz VC, et al. (2006) Enhancement of non-dominant hand motor function by anodal transcranial direct current stimulation. Neurosci Lett 404: 232-236.
-
Nasseri P, Nitsche M, Ekhtiari H (2015) A framework for categorizing electrode montages in transcranial direct current stimulation. Front Hum Neurosci 9(12): 12-23.
-
Boggio PS, Nunes A, Rigonatti SP, Nitsche MA, Pascual- Leone A, et al. (2007) Repeated sessions of noninvasive brain DC stimulation are associated with motor function improvement in stroke patients. Restor Neurol Neurosci 25(2): 123-129.
-
Au-Yeung Y, Wang J, Chen Y, Chua E (2014) Transcranial Direct Current Stimulation to Primary Motor Area Improves Hand Dexterity and Selective Attention in Chronic Stroke. Am J Phys Med Rehabil 93(12): 1057- 1064.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial