Ankle-Foot Orthoses in Spinal Cord Injury: Systematic Review of Literature
Background: Spinal cord injury patient present gait abnormality, and this can compromise physical and mental health. Ankle- Foot Orthosis are the most used orthoses in the walking rehabilitation of these patients. Aim: The aim of this review was to overview types, characteristics, function and efficacy of ankle-foot orthosis in the rehabilitation of SCI patients, based on the literary EBM. Methods: A systematic review was conducted throught a clinical query based on PICO method. Studies were identified in Pubmed, MEDLINE, ISI Web of Knowledge, EDS Base Index, PEDro, NARCIS database. PRISMA Statement was used to report results, and Newcastle-Ottawa Castle was used to assess quality of the articles. Results: The review included five cohort studies. Four studies used hinged AFOs and compared them with other orthoses for the walking rehabilitation of SCI patients. Two studies concerned powered AFOs, and two other ones combined them with other rehabilitation devices. According to the Newcastle-Ottawa Scale, all studies scored 6/7 and 7/7. Discussion: Hinged AFOs provided the best performance and effective devices, especially in the rehabilitation context. Powered AFOs are innovative orthoses with a great evaluative, therapeutic and prognostic value. They can promote recover of walking ability in SCI patients. A comprehensive rehabilitation programme, using hands-on techniques, aids and orthoses together with AFOs is effective and better than the single use of a device.
Introducation
Spinal cord injury (SCI) refers to an interruption of the continuity of ascending and descending nerve pathways, which form the spinal cord [1, 2, 3, 4, 5]. According to international quality studies, the overall estimate SCI incidence is about 40-80 new cases every year for millions of inhabitants. So, every year, around the world, between 250 000 and 500 000 people suffer a spinal cord injury [6, 7, 8].
Currently, the prevalence of SCI patients in the United States is approximately of 290.000 with a range that varies from 249.000 to 363.000 [9, 10, 11, 12, 13, 14].
The most recurrent type of SCI is the traumatic one, meaning accidents, violent acts, falls or sport injuries. According to data, it occurs mostly in the young population, because they are more active so more at risk [12, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29]. Normally, these people have a higher and longer life expectancy also after the trauma, and they are more motivated to recover autonomy and motricity than elderly patients [30, 31, 32, 33]. As a consequence, the walking training plays major mental and physic role for young people with a consistent clinic situation [34, 35, 36, 37, 38, 39, 40, 41, 42, 43]. Ankle-foot orthoses (AFO) are used to cope with the weaknesses and spasticity of the ankle joint [44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54].
That’s why AFOs are the most used orthoses in the rehabilitation and daily routine SCI patients, due to the large number of those people having distal deficiency of the lower limb.
The aim of this review is to highlight the knowledge, data and information found in the literature about the use of AFOs (ankle-foot orthoses) for SCI subjects, in order to support and encourage further research.
The goal is to provide an overview of use, types and efficiency of AFOs with evaluative, predictive and rehabilitative purposes in the rehabilitative process of SCI patients.
Methods
A systematic review of literature has been conducted; Clinical Query has been developed through the PICO method (Population Intervention Comparison Outcome) [55, 56], based on the choice of key words and their composition (Table 1).
| Population | Intervention | Comparison | Outcome |
|---|---|---|---|
| Spinal Cord Injury | AFO | Not applicable | Six Minutes Walking Test |
| Incomplete Spinal Cord Injury | Ankle Foot Orthoses | Gait Analysis | |
| Paraplegia | Codivilla Spring | Kinetic | |
| Paraplegic | Kinematic | ||
| Cadence | |||
| Walking Speed | |||
| Step Lenght | |||
| Range of motion | |||
| Temporospatial parameter | |||
| Proprioceptive threshold | |||
| Foot Clearance | |||
| Electromyography | |||
| Endurance |
Table 1: Keywords selected using PICO method.
Studies have been identified on the web in the database of Pubmed, MEDLINE, ISI Web of Knowledge, EDS Base Index, Physiotherapy Evidence Database (PEDro) and National Academic Research and Collaborations Information System (NARCIS). A primary screening of literature revealed a lack of RCTS, so we chose to conduct the research on cohort studies.
PRISMA Statement (Preferred Reporting Items for Systematic Reviews and Meta-Analyzes) has been used to report the research results. Articles quality assessment has been made following the Newcastle-Ottawa Scale (NOS), which evaluates the quality of non-randomized studies.
The Table 2 shows the inclusion and exclusion criteria used for this study, meaning cohort studies on adults with acute or chronic, complete and incomplete spinal cord injury (cervical, thoracic or lumbar). Publication date had not earlier than 2004. Studies about the impact of solid and mechanic, articulated, electro-hydraulic, robotic jointed ankle-foot orthoses (AFO) have been selected for the review.
Selected documents had to refer these outocme measures: Six Minute Walking Test (6MWT), Gait Analysis, human kinetic, walking kinematics, foot cadence, walking speed, step length, range of motion (ROM), space-time walking parameters, ankle proprioceptive threshold, foot clearance, EMG and endurance.
Other studies, published more than 16 years ago and conducted on minors, animals, that included alternative outcome measures used on patients with different disability, second level literary studies research (reviews, meta-analysis etc.), have been excluded.
The abstract and the full text, complete with all the studies found in the databases, have been compared to the inclusion criteria and checked by a single reviewer.
| Inclusion criteria | Exclusion criteria |
|---|---|
| Cohort studies | Second level literary studies research |
| Studies published in the past 16 years | Studies published more than 16 years ago |
| Population’s age > 18 years | Population’s age < 18 years |
| Population with acute or chronic, complete or incomplete,cervical, dorsal or lumbar SCI | Adults with other neurological diseases other than SCI |
| Studies with the following outcome measures: 6MWT, Gait Analysis, kinetics, kinematics, cadence, walking speed, stride, step, ROM, spatio-temporal walking parameters, proprioceptive threshold and foot clearance, EMG, endurance. | Studies with different outcome measures |
| Animals |
Table 2: Inclusion and exclusion criteria used in articles’ selection.
Results
A total of 98 results have emerged from the research on the databases. After reading the title and abstract, only few articles have been selected, according to the inherence to the topic and inclusion criteria. In case of uncertainty, the article has been read entirely.
Last, after reading the article fully, 5 cohort studies have been selected (Figure 1).
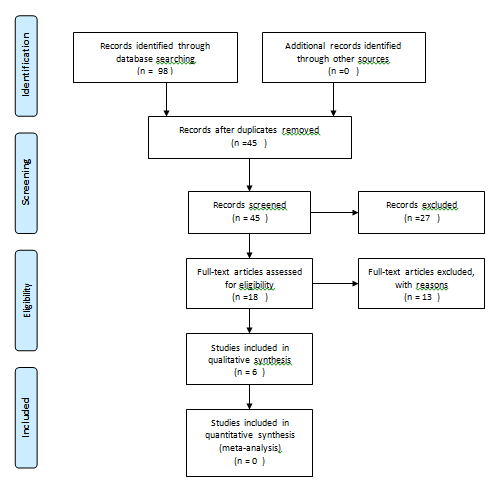
Five cohort studies were selected for final review. The characteristics of the selected articles are summarized in Table 3. According to the Newcastle-Ottawa Scale, all studies scored 6/7 and 7/7 (Table 4).
Date and Journal Author and Title Population (n) and Protocol Outcome measures Results Dambreville C, Pairot de Fontenay B, Blanchette AK, Roy J-S, Mercier C, Bouyer Ankle proprioception during gait in individuals with incomplete spinal cord injury
15 with iSCI 65 healthy Test the ankle proprioception in SCI patients during the walking through a rAFO
07.10.19 Physiological Reports
19 with iSCI Comparison the effect of a hinged AFO to the one of a FES in 4 conditions:
- with hinged AFO
- with FES
- with hinged AFO and FES
- without orthosis
01.10.04 Archives of physical medicine and rehabilitation Kim CM, Eng JJ, Whittaker MW Effects of a simple functional electric system and/or a hinged ankle-foot orthosis on walking in persons with incomplete spinal cord injury
5 with iSCI Comparison between a solid AFO and a hinged AFO with regard to the space-time parameters of the gait. The individuals had to walk on the treadmill in 3 conditions:
- barefoot
- wearing bilaterally two solid AFOs
- wearing bilaterally two hinged AFOs Arazpour M, Tajik HR, Aminian G, Bani MA, Ghomshe FT, Hutchins SW Comparison of the effects of solid versus hinged ankle foot orthoses on select temporal gait parameters in patients with incomplete spinal cord injury during treadmill walking.
02.07.12 Prosthetics and Orthotics International
- Gender, age and pain did not affect the disturbance perception applied by the r-AFO
- Speed affected the proprioception (with minor speed, the proprioceptive threshold was inferior so that the ankle proprioception increased)
- Proprioception was compromised in SCI patients with respect to healthy individuals
- Proprioception varied in SCI patients depending on the injury, from values similar to the ones of the control groups (healthy subjects) to nulls
- Proprioceptive assessment was possible with a rAFO
- Proprioceptive threshold
- Walking speed
- Walking speed increased with the use of AFOs and FES
- Walking speed increased with the use of AFOs and FES combined together
- The distance travelled in the 6MWT increased with the use of AFOs
- Foot clearance reached the highest values with the use of FES
- The more significant positive variations were always obtained by combining AFOs to FES.
- 6MWT (walking speed and endurance)
- Foot clearance
- Step length and cadence increased when patients walked wearing orthoses (compared to walking barefoot)
- Those measurements reached the higher numbers when the subjects wore the solid AFO with regard to the hinged AFO
- The ankle ROM improved with the use of AFOs compared to barefoot without significant differences between the two orthotic conditions.
- Ankle ROM
- Step length
- Cadence
- Sawicki GS, Domingo A, Ferris DP
- The effects of powered ankle-foot orthoses on joint kinematics and muscle activation during walking in individuals with incomplete spinal cord injury.
- 28.02.06
- Journal of Neuro
- Engineering and
- Rehabilitation
- Bani MA, Arazpour M, Ghomshe
- FT, Mousavi ME, Hutchins SW
- Gait evaluation of the advanced reciprocating gait orthosis with solid versus dorsi flexion assist ankle foot orthoses in paraplegic patients.
- 17.09.12
- Prosthetics and Orthotics
- International
Table 3: Description of the selected articles.
5 with iSCI It was tested the mobility assistance from a robotic powered AFO. During the test, each participant walked on the treadmill with body weight partial support (regulated in accordance with individual necessities) at four different speeds in three conditions under the control of the therapist:
- without orthoses
- wearing bilaterally solid AFOs
- with a pAFO.
Some subjects tested the fourth condition which referred to the automatic control of powered orthoses, without the help of the therapist.
- Ankle ROM increased in the final phase when the individuals used the pAFO compared to the solid AFO.
- The EMG resulting values were the same both with the pAFO and the solid AFO (except the soleus that activated for the 13% in less with powered AFO).
- Two out of five subjects were able to control the orthosis automatically, at the expense of the ankle ROM.
- Ankle ROM
- EMG
- Assistance from orthosis
3 with iSCI 1 with complete SCI Comparison the influence of a solid AFO and a hinged AFO in paraplegic patients that use ARGO. The test consisted of a walking evaluation through a walkway of 6m for at least five times with selected speed in two conditions: 1. the individuals started to walk with ARGO and bila teral solid AFO 2. with ARGO and hinged AFO, which were wore bilaterally.
- Foot cadence did not vary so much between the two orthoses
- Step length and the speed reached higher values with the use of AFO, which supported the dorsiflexion.
- The degrees of gait of hips and knees did not vary between the two orthoses
- Ankle ROM increased significantly with the use of hinged AFO
- Ankle ROM
- Knee ROM
- Hip ROM
- Stride length
- Cadence
- Walking speed
| n° | Date | Author | Newcastle-Ottawa Scale |
|---|---|---|---|
| 1 | 07.10.19 | Dambreville C, Pairot de Fontenay B, Blanchette AK, Roy J-S, Mercier C, Bouyer | 7 |
| 2 | 01.10.04 | Kim CM, Eng JJ, Whittaker MW | 7 |
| 3 | 02.07.12 | Arazpour M, Tajik HR, Aminian G, Bani MA, Ghomshe FT, Hutchins SW. | 6 |
| 4 | 28.02.06 | Sawicki GS, Domingo A, Ferris DP | 7 |
| 5 | 17.09.12 | Bani MA, Arazpour M, Ghomshe FT, Mousavi ME, Hutchins SW. | 6 |
Population
Dambreville, et al. [57] recruited 15 individuals with incomplete spinal cord injury (ASIA C/D), stable medical conditions and capacity of walking on the treadmill have been included; non exposed cohort was composed by 65 healthy individuals, in order to evaluate factors that could influence the test, and to verify the reliability of the test-retest.
Similarly, Kim, et al. [58] recruited 19 adults (age 42,7±13,6 years) with incomplete spinal cord injury (ASIA C/D), stable medical conditions, ability of therapeutic or functional walking with or without orthoses. Indeed, patients used a cane during the test (8 of them used a single cane, one 2 canes, one a single crutch, five 2 crutches, three an axillary walker and three wore ankle-foot orthoses daily).
In Arazapour cohort study [59], 5 adults (age 28±8,68 years) with incomplete thoracic spinal cord injury (ASIA C/D), stable medical conditions, no orthopaedic complications and capacity of limited deambulation were studied.
Sawicki, et al. [60] included in his study 5 subjects of age 44.6 ± 15.5 years with incomplete spinal cord injury (ASIA C/D) at the cervical and thoracic level, stable medical conditions, without a history of orthopedic complications and with limited walking abilities.
Lastly, 4 adults (age 26,5±2,5 years) with thoracic spinal cord injury (ASIA A/B), stable medical conditions, no orthopaedic, cardiovascular, pulmonary complications, no obesity and spasticity had been included by Bani, et al. [61].
1.1. Aims and Measures Applied Dambreville, et al. [57] tested ankle proprioception in SCI patients during the walking with r-AFO, ( ankle-foot electro- hydraulic robotic orthosis); in addition, 65 healthy patients tested the reliability of the robotic device and analysed factors that may affect proprioception. For SCI individuals, the procedure consisted of the use of robotic electro-hydraulic AFO, walking on a treadmill (speed between 0.6-3 km/h); the orthosis applied a perturbation (of entity between 0.5Nm and 8Nm) that provoked a rapid deviation to the angular position of the ankle. The motion happened always during the initial phase of the swing, on average every five steps. The patient had to push a button when and if he perceived a disturbance. The visual foot feedback was not allowed. Healthy patients underwent the same test.
In their study, instead, Kim, et al. [58] compared the effect of a hinged AFO to FES (functional electric stimulation) about foot clearance, walking speed and endurance. They also assessed the benefits of combining the two methods. The gait was analysed throughout four conditions: without wearing any orthosis and without stimulation, with hinged AFO blocked in plantarflexion and set free in dorsiflexion, with electrical stimulation of the muscle (FES), at one time with hinged AFO and FES.
Arazpour, et al. [59] compared the use of a solid AFO to a hinged AFO for space-time parameters of gait (average step length and average cadence). The individuals had to walk barefoot on the treadmill, wearing bilaterally two solid AFOs and then two hinged ones.
In their study of 2006, Sawicki GS, et al. [60] tested the mobility assistance for robotic powered AFO in joint kinematics and muscle activation of the lower limb during the deambulation. A powered AFO is an orthosis with artificial pneumatic muscles which support the plantarflexion.
During the test, each participant walked on the treadmill with body weight partial support at four different speeds (0.36, 0.54, 0.72 and 0.89 m/s) in three conditions: no orthoses, meaning wearing bilaterally solid AFOs, with a p-AFO, under the control of the therapist.
Some subjects tested the fourth condition which referred to the automatic control of powered orthoses, without the help of the therapist.
Last, Bani’s study [61] compared solid AFO and hinged AFO that supported the dorsiflexion, with on space-time parameters of gait and with ROM joints of lower limbs in paraplegic patients that use ARGO. (Advanced Reciprocating Gait Orthosis). Participants made a training of 6-10 weeks with an ARGO combined to a solid AFO or AFO dorsiflexion assisted orthosis. During that period, they also strengthened the upper body muscles, reached the autonomy of the management and the use of orthoses, and together with these orthoses, they found a secure orthostatic position, and the ability to walk again on a regular surface. The test consisted of a walking evaluation through a walkway of 6m for at least five times with selected speed in two conditions: first, the individuals started to walk with ARGO and bilateral solid AFO and then with ARGO and AFO that supported the dorsiflexion.
Outcome used and Results
In Dambraville, et al. [57] study outcome measures were the ankle and walking speed proprioceptive threshold. As a result of the tests factors which were independent by SCI (gender, age and pain), did not affect the disturbance perception applied by the r-AFO. On the contrary, the speed affected proprioception: with minor speed, the proprioceptive threshold was inferior, so ankle proprioception increased. As expected, the proprioception was more compromised in SCI than healthy individuals, and it varied in SCI patients depending on the injury, from values similar to control cohort to absent. Lastly, proprioceptive assessment was ascertained to be feasible and reliable during walking rehabilitation with r-AFO. Instead, Kim, et al. [58] identified 6MWT (Six Minutes Test), walking speed and foot clearance values as outcome. After testing, walking speed increased not only with the use of AFOs and FES, but also when these two devices were combined together (18% more than the deambulation without orthoses). The distance by 6MWT increased with the use of AFOs, because the endurance values rose, while the foot clearance reached the highest values with the use of FES. The best performance was always obtained by combining AFOs to FES.
Arazpour, et al. [59] outcome were step length, foot cadence and ankle ROM. The medium step length and the average foot cadence reached higher values when patients walked using the orthoses compared to barefoot deambulation. The ankle articulate ROM improved with the use of AFOs compared to barefoot use without significant differences between the two orthotic conditions.
Sawicki, et al. [60] analysed ROM variations, the EMG resulting values conducted on the participants and the benefit of orthoses to the deambulation. Particularly, ankle ROM increased in the final phase when the individuals used the pAFO compared to the solid AFO. EMG values, instead, were the same both with the pAFO and the solid AFO (except the soleus that activated for the 13% in less with powered AFO). Lastly, two of five subjects were able to control the orthosis automatically, at the expense of the ankle ROM.
In conclusion, Bani, et al. [61] chose foot cadence, step length, gait speed and ROM of the three joints of the lower limbs as outcome measures; author’s experience demonstrated that foot cadence did not vary between the two orthoses, while the step length and the speed reached higher values with the use of AFO. The degrees of gait of hips and knees did not vary between the two orthoses, differently from ankle ROM, which increased significantly with the use of AFO for dorsiflexion.
Discussion
This study resulted compliant to all 27 items proposed by the PRISMA Statement checklist for the reporting of the systematic reviews of literature. The strongest point of this review is the research of a specific theme, which has been highly neglected by researchers. The aim was to highlight the knowledge, data and information already existing in literature for the future research. The information and instrumentation used in the studies were simple, concrete, affordable for every rehabilitation centre, and easily applicable to the clinical uniqueness of a single patient. The outcome indicators and the measurement methods were uniform on the entire review.
The major critical point of this study was the lack of experiences with a high methodological value (RCTs); scientific knowledge about rehabilitation using AFOs in SCI patients is extremely low. On the contrary, this theme, applied to patients with brain damage (ischemic strokes, haemorrhagic strokes, cerebral palsy and head trauma) is widely addressed in the literature, even with qualitative valid studies [62, 63, 64]. For this reason, this topic needs more scientific researches.
The risk of bias among all studies is low since this review does not present a final statistical analysis of data and the reviewer (third party and external to any study included) has no interest in publishing but only in reporting information.
Hinged AFO
Four of the five studies included in this review investigated effects of hinged AFO during walking rehabilitation in SCI patients, especially with incomplete injuries. In three out of four studies, the deambulation quality was tested by alternating hinged AFOs with solid ones. In one of the studies walking rehabilitation with hinged AFO was compared to the one without any orthosis. The parameters evaluated by the studies were ankle range (ROM), speed, cadence, foot clearance, step length and endurance.
Kim, et al. [58] demonstrated that foot clearance values increased when subjects used hinged AFOs (27.88mm) compared to walking without orthosis (8.78mm). Moreover, in Arazpour’s study [59], the angle of the ankle in plantarflexion varied from 6.69° ± 7.56° in walking rehabilitation without orthosis, to 8.37° ± 8.01° wearing solid AFO, in order to arrive with hinged AFO at 11.43° ± 11.15°. This large opening of the ankle angle in the last condition was present in subjects in which the plantarflexion and dorsiflexor muscle was strong or scarcely affected by the neurological deficit. A powered hinged AFO was used in the Sawicki’s study [60], and it modified the ankle ROM in SCI patients. Using solid AFOs, ROM decreased compared with walking without orthosis. The main function of these AFOs was the stabilization of the joint, at the expense of the ROM. However, individuals reported a feeling of instability when wearing articulated AFOs, that disappeared when they wore solid type AFOs. Lastly, in the Bani’s article [61] an increase in ROM in walking rehabilitation with hinged AFO (11.63° ± 0.15°) was confirmed compared to the one with solid AFO (8.05° ± 0.51°) to the detriment of the feeling of stability. Talking about space-time parameters of walking rehabilitation, Kim, et al. [58] noted a slight increase in speed, from 0.40 m/s to 0.43 m/s, in the walking rehabilitation without orthosis compared to the one wearing articulated AFOs. In the latest case, the endurance values during the 6MWT also increased. In the Arazpour’s study [59], cadence increased with hinged orthoses but step length was greater with solid orthoses. Bani, et al. [61] detected higher speed and cadence when participants wore hinged AFO (0.35 ± 0.01 m / s and 42 ± 3.09 steps / min) than when they used solid AFOs (0.32 ± 0.02 m / s and 40 ± 2.38 steps / min). Stride length was greater with articulated orthoses than with solid ones. This diversity could be explained by analysing the peculiarities and structural discrepancies of the two orthoses. Indeed, even if they were both hinged AFOs, they could produce heterogeneous effects with highly subjective, personal and non-standardizable disabilities. In conclusion, hinged AFOs led to more effective results in ankle range of motion, gait clearance, speed, cadence and endurance. On the other hand, the solid AFOs produced lower performances but ensured a high stability and safety to the individual who used them. Solid type orthoses are the most suitable for daily use with the lowest risk of falls and the greatest comfort for the SCI subjects, while hinged AFOs are more appropriate in a physiotherapeutic and rehabilitative context.
Powered AFOs
For SCI patients the development of powered orthoses for the ankles could offer an innovative solution, to reduce energetic dispendious by mechanic orthoses. Two of the studies included in this review proposed and experimented the use of powered AFO on subjects with incomplete SCI. In the study by Dambreville, et al. [57] a foot ankle robotic electro-hydraulic orthosis (r-AFO) was used to evaluate the residual proprioception of the ankle during the walking in subjects with incomplete SCI. The r-AFO was put on the lower limb which presented more weakness in all patients.
Following proofs, it was ascertained that proprioception of the ankle in the individuals with SCI is compromised in respect to the sane subjects, confirming and extending the scope of the precedent studies. Proprioception detected, was strictly related to lesion, and went from values that where similar to the ones of healty subjects, to nothing. This variability reflected the heterogeneity of SCI population, represented in the study by recruitment of participants with different demographic and clinic profiles (time post-trauma, velocity of ambulation, level of injury).
The evaluation of the proprioception during the walking with r-AFO represents a more reliable and effective proof, compared to tests that require the passive or active segmentary mobility. The second article included in this review to propose a powered orthosis on patients with incomplete SCI is the one by Sawicki, et al. [60]. The goal of the study was to test the robotic assistance of a powered AFO (pAFO) on the joint kinematics, and the muscular activation during walking.
Normally, in the subjects affected by SCI, given the limited propulsion at the end of the stance, the angle of the ankle in the push-off phase is typically reduced [65]. But, when the patients used the pAFO under a therapist control, the ankle angle in such phase increased on the physiological level of -12 degrees. Robotic assistance has taken the kinematic of the push of the ankle to a condition similar to the one of the sane patients, even though the speed was reduced. An important result of the study was reported on the electromyography: the muscular activation was not reduced with the use of pAFO, except from the soleus that registered a diminution on the recruitment 13% during the support stage. authors demonstrated that the use of powered orthosis in a rehabilitative context, emphasize the muscular active recruitment, stimulating the neural plasticity, to maximize the motor recovery. In conclusion, the mechanic assistance given by powered orthosis foot-ankle has improved the push cinematic of the ankle, without reducing the muscular activation during the ambulation. These results are surely positive and put the pAFO as a valid instrument usable during the rehabilitation of the walk of a patient with spinal cord injury.
The AFO and Other Rehabilitative Instruments
Two studies included in this review analyse the possible advantages given by the combination of AFO to other orthoses. Kim, et al. [58], in their study, compared the effects of a hinged AFO and a FES in the walk of patients with an incomplete SCI. Following the tests, it was demonstrated that the distance at 6MWT increased with the use of AFO, since the endurance values increased. Foot clearance, on the other hand, reached higher values with the usage of FES. Although, the most significatively positive variations were given by the combination of AFO and FES for both endurance and foot clearance. Gait speed increased with both the use of AFO and FES, but the most significant improvement was given when these two elements were merged together (18% more that the deambulation without orthotics). So, there was no type of orthosis superior to the other, but that effects produced on walking were complementary: FES acted decreasing the foot-drop during the swing phase, while the AFO gave more stability during the support. These results confirm the informations by other studies [66, 67, 68, 69]. In Bani’s study [61] it was investigated the influence of a solid AFO and an AFO that assists the dorsiflexion, on the space-time parameters of the gait and on the articular ROM of the lower limbs in paraplegic patients, who use ARGO. Tests and measurements demonstrated that the range of motion of the steps didn’t vary significantly between the two orthotics, meanwhile the step length and the speed was significantly greater with the use of AFO that assist the dorsiflexion. The degrees of gait of hips and knees didn’t vary between the two orthoses, differently from the ankle’s ROM which, instead, increased with the usage of AFO in assistance to dorsiflexion. Bani, et al. [61] not only confirmed the positive effects of ARGO in deambulation of spiral cord injured patients [70, 71], but they also demonstrated the added value and the benefits that the conjunction of said orthosis and a hinged AFO give to the patient.
Conclusion
The use of ankle-foot orthosis is fundamental and extremely beneficial to the recovery and the training recovery in patients with spinal cord injuries.
- Hinged AFOs show higher performances, while solid AFOs lower ones, but high degrees of stability. For these reasons, solid orthoses are more adequate for a daily usage, while hinged AFOs are more appropriate in rehabilitative context.
- Powered AFOs have great evaluative, rehabilitative and prognostic value, useful to positively influence and incentivize the recovery of ambulation of SCI patients.
- The use of FES with foot-ankle orthoses and ARGO or matched to a hinged AFO, might represent an added value to the recovery of the walk.
References
-
Gosselin RA, Coppotelli C (2005) A follow up study of patients with spinal cord injury in Sierra Leone. Int Ort 29: 330-332.
-
Allotey P (2003) The DALY, context and the determinants of the severity of disease: an exploratory comparison of paraplegics in Australia and Cameroon. Soc Sci & Med 57(5): 949-958.
-
Liverman CT, Altevogt BM, Joy JE, Richard T (2005) Spinal cord injury: progress, promise, and priorities. Washington, DC, Nat Acad Pr.
-
Weerts E, Wyndaele JJ (2011) Accessibility to spinal cord injury care worldwide: the need for poverty reduction. Spinal Cord 49(7): 767.
-
Kirshblum SC, Burns SP, Biering Sorensen F, Donovan W, Graves DE, et al. (2011) International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 34: 535-546.
-
Noonan VK, Fingas M, Farry A, Baxter D, Singh A, et al. (2012) Incidence and prevalence of spinal cord injury in Canada: a national perspective. Neuroepidemiology 38(4): 219-226.
-
Knútsdóttir S, Thórisdóttir H, Sigvaldason K, Jónsson H Jr, Björnsson A (2012) Epidemiology of traumatic spinal cord injuries in Iceland from 1975 to 2009. Spinal Cord 50: 123-126.
-
Hagen EM, Eide GE, Rekand T, Gilhus TE, Gronning G (2010) A 50-year follow-up of the incidence of traumatic spinal cord injuries in western Norway. Spinal Cord 48: 313-318.
-
Rahimi Movaghar V, Saadat S, Rasouli MR, Ganji S, Ghahramani M, et al. (2009) Prevalence of spinal cord injury in Tehran, Iran. J Spinal Cord Med 32(4): 428-431.
-
Dahlberg A, Kotila M, Leppänen P, Kautiainen H, Alaranta H (2005) Prevalence of spinal cord injury in Helsinki. Spinal Cord 43: 47-50.
-
O’Connor PJ (2005) Prevalence of spinal cord injury in Australia. Spinal Cord 43: 42-46.
-
New PW (2013) Prevalence of non-traumatic spinal cord injury in Victoria, Australia. Spinal Cord 51(2): 99-102.
-
Jain NB, Ayers GD, Peterson EN, Harris MB, Morse L, et al. (2015) Traumatic spinal cord injury in the United States, 1993-2012. JAMA 313(22): 2236-2243.
-
Lasfargues JE, Custis D, Morrone F, Carswell J, Nguyen T (1995) A model for estimating spinal cord injury prevalence in the United States. Paraplegia 33(2): 62-68.
-
Surkin J, Gilbert BJC, Harkey HL, Sniezek J, Currier M (2000) Spinal cord injury in Mississippi: findings and evaluation, 1992–1994. Spine 25(6): 716-721.
-
Olasode BJ, Komolafe IE, Komolafe M, Olasode OA (2006) Traumatic spinal cord injuries in Ile-Ife, Nigeria, and its environs. Trop Doct 36(3): 181-182.
-
Lakhey S, Jha N, Shrestha BP, Niraula SR (2005) Aetioepidemiological profile of spinal injury patients in eastern Nepal. Trop Doct 35(4): 231-233.
-
Deconinck H (2003) The health condition of spinal cord injuries in two Afghan towns. Spinal Cord 41(5): 303- 309.
-
Costacurta MLG (2010) Epidemiological profile of a pediatric population with acquired spinal cord injury from AACD: Sao Paulo/ Brazil. Spinal Cord 48(2): 118- 121.
-
Ones K, Yilmaz E, Beydogan A, Gultekin O, Caglar (2007) Comparison of functional results in non-traumatic and traumatic spinal cord injury. Disabil Rehabil 29(15): 1185-1191.
-
DeVivo MJ, Vogel LC (2004) Epidemiology of spinal cord injury in children and adolescents. Journal Spinal Cord Med 27(S1): S4-S10.
-
Dahlberg A, Kotila M, Leppänen P, Kautiainen H, Alaranta H (2005) Prevalence of spinal cord injury in Helsinki. Spinal Cord 43(1): 47-50.
-
Ronen J, Goldin D, Bluvshtein V, Fishel B, Gelernter I, et al. (2004) Survival after nontraumatic spinal cord lesions in Israel. Arch Phys Med Rehabil 85(9): 1499-1502.
-
Lee JH, Sung IY, Kang JY, Park SR (2009) Characteristics of pediatric-onset spinal cord injury. Pediatr Int 51: 254- 257.
-
Obalum DC, Giwa SO, Adekoya Cole TO, Enweluzo GO (2009) Profile of spinal injuries in Lagos, Nigeria. Spinal Cord 47(2): 134-137.
-
Knútsdóttir S, Thórisdóttir H, Sigvaldason K, Jónsson Jr H, Björnsson A, et al. (2009) Epidemiology of traumatic spinal cord injuries in Iceland from 1975 to 2009. Spinal Cord 50(2): 123-126.
-
O’Connor P (2002) Incidence and patterns of spinal cord injury in Australia. Accid; Anal Prev 34(4): 405-415.
-
Catz A, Thaleisnik M, Fishel B, Ronen J, Spasser R, et al. (2002) Survival following spinal cord injury in Israel. Spinal Cord 40: 595-598.
-
Celani MG, Spizzichino L, Ricci S, Zampolini M, Franceschini M (2001) Spinal cord injury in Italy: a multicentre retrospective study. Arch Phys Med Rehabil 82(2): 589-596.
-
Anderson KD (2004) Targeting recovery: priorities of the spinal cord injured population. Journal Neurotrauma 21(10): 1371-1383.
-
Anderson KD, Anderson KD, Borisoff JF, Johnson RD, Stiens SA, et al. (2007) The impact of spinal cord injury on sexual function: concerns of the general population. Spinal Cord 45(5): 328-337.
-
Ditunno PL, Patrick M, Stineman M, Ditunno JF (2008) Who wants to walk? Preferences for recovery after SCI: a longitudinal and cross-sectional study. Spinal Cord 46: 500-506.
-
Snoek GJ, IJzerman MJ, Hermens HJ, Maxwell D, Biering- Sorensen F (2004) Survey of the needs of patients with spinal cord injury: impact and priority for improvement in hand function in tetraplegics. Spinal Cord 42(9): 526- 532.
-
Kreutz D (2000) Standing frames and standing wheelchairs: implications for standing. Top Spinal Cord Inj Rehabil 5: 24-28.
-
Shields RK, Dudley Javoroski S (2006) Musculoskeletal plasticity after acute spinal cord injury: effects of long- term neuromuscular electrical stimulation training. J Neurophysiol 95(4): 2380-2390.
-
Wolfe DL (2012) Physical activity and SCI. In: Eng JJ, et al. (Eds.), Spinal cord injury rehabilitation evidence. Version 4. Vancouver, Spinal Cord Injury Rehabilitation Evidence (SCIRE).
-
Borg J, Lindström A, Larsson S (2011) Assistive technology in developing countries: a review from the perspective of the Convention on the Rights of Persons with Disabilities. Prost Orthot Int 35(1): 20-29.
-
Connolly SJ, McIntyre A, Mehta S, MA Brianne L Foulon, Teasell RW (2012) Upper limb rehabilitation following spinal cord injury. In: Eng JJ, et al. (Eds.), Spinal cord injury rehabilitation evidence, Version 4. Vancouver, Spinal Cord Inj Rehabil Evid (SCIRE).
-
Wuolle KS, Bryden AM, Peckham PH, Murray PK, Keith M (2003) Satisfaction with upper-extremity in individuals with tetraplegia. Arch Phys Med Rehabil 84: 1145-1149.
-
Snoek GJ, Van Til JA, Krabbe PF, Ijzerman MJ (2008) Decision for reconstructive interventions of the upper limb in individuals with tetraplegia: the effect of treatment characteristics. Spinal Cord 46(3): 228-233.
-
Yeo JD, Walsh J, Rutkowski S, Soden R, Craven M, et al. (1998) Mortality following spinal cord injury. Spinal Cord 36(5): 329-336.
-
DeVivo MJ, Krause JS, Lammertse DP (1999) Recent trends in mortality and causes of death among persons with spinal cord injury. Arch Phys Med Rehabil 80(11): 1411-1419.
-
Krause JS, DeVivo MJ, Jackson AB (2004) Health status, community integration, and economic risk factors for mortality after spinal cord injury. Arch of Phys Med and Reh 85: 1764-1773.
-
Janisse DJ, Janisse E (2008) Shoe modification and the use of orthoses in the treatment of foot and ankle pathology. J Am Acad Orthop Surg 16(3): 152-158.
-
Nawoczenski DA, Janisse DJ (2004) Foot orthoses in rehabilitation--what’s new. Clin Sports Med 23(1): 157-
-
Chevalier TL, Chockalingam N (2011) Foot orthoses: a review focusing on kinematics. J Am Podiatr Med Assoc 101(4): 341-348.
-
Rowan Robinson K (2019) Knee Orthoses for Treating Patellofemoral Pain Syndrome. Orthop Nurs 38(1): 55- 56.
-
Tyson SF, Kent RM (2013) Effects of an ankle-foot orthosis on balance and walking after stroke: a systematic review and pooled meta-analysis. Arch Phys Med Rehabil 94 (7): 1377-1385.
-
AlamM, Choudhury IA, Mamat AB (2014) Mechanism and design analysis of articulated ankle foot orthoses for drop-foot. Sci World J 2014: 867869.
-
Tyson S, Sadeghi Demneh E, Nester S (2013) A systematic review and meta-analysis of the effect of an ankle-foot orthosis on gait biomechanics after stroke. Clin Rehabil 27(10): 879-891.
-
Ferreira LAB, Neto HP, Christovao TCL, Duarte NA, Lazzari ND, et al. (2013) Effect of ankle-foot orthosis on gait velocity and cadence of stroke patients: a systematic review, J Phys Ther Sci 25(11): 1503-1508.
-
Degelaen M (2019) Effect of ankle-foot orthoses on motor performance in cerebral palsy. Dev Med Child Neurol 61(2): 119-120.
-
Prenton S, Hollands KL, Kenney LPJ, Onmanee P (2018) Functional electrical stimulation and ankle foot orthoses provide equivalent therapeutic effects on foot drop: A meta-analysis providing direction for future research. J Rehabil Med 50(2): 129-139.
-
Zollo L, Zaccheddu N, Ciancio AL, Morrone M, Bravi M, et al. (2015) Comparative analysis and quantitative evaluation of ankle-foot orthoses for foot drop in chronic hemiparetic patients. Eur J Phys Rehabil Med 51(2): 185-196.
-
Miller SA, Forrest JL (2001) Enhancing your practice through evidence-based decision making: PICO, learning how to ask good questions. J Evidence-Based Dental Pract 1(2): 136-141.
-
Huang X, Lin J, Demner Fushman D (2006) Evaluation of PICO as a knowledge representation for clinical questions. AMIA Annu Symp Proc 2006: 359-363.
-
Dambreville C, Pairot de Fontenay B, Blanchette AK, Roy JS, Mercier C, et al. (2019) Ankle proprioception during gait in individuals with incomplete spinal cord injury. Physiol Rep 7(24): e14328.
-
Kim CM, Eng JJ, Whittaker MW (2004) Effects of a simple functional electric system and/or a hinged ankle-foot orthosis on walking in persons with incomplete spinal cord injury. Arch Phys Med Rehabil 85(10): 1718-1723.
-
Arazpour M, Tajik HR, Aminian G, Bani MA, Ghomshe FT, et al. (2013) Comparison of the effects of solid versus hinged ankle foot orthoses on select temporal gait parameters in patients with incomplete spinal cord injury during treadmill walking. Prosthet Orthot Int 37(1): 70-75.
-
Sawicki GS, Domingo A, Ferris DP (2006) The effects of powered ankle-foot orthoses on joint kinematics and muscle activation during walking in individuals with incomplete spinal cord injury. J Neuroeng Rehabil 3: 3.
-
Bani MA, Arazpour M, Ghomshe FT, Mousavi ME, Hutchins SW (2013) Gait evaluation of the advanced reciprocating gait orthosis with solid versus dorsi flexion assist ankle foot orthoses in paraplegic patients. Prosthet Orthot Int 37(2): 161-167.
-
Pohl M, Mehrholz J (2006) Immediate effects of an individually designed functional ankle-foot orthosis on stance and gait in hemiparetic patients. Clin Rehabil 20(4): 324-330.
-
Aboutorabi A, Arazpour M, Ahmadi Bani M, Saeedi H, Head JS (2017) Efficacy of ankle foot orthoses types on walking in children with cerebral palsy: A systematic review. Ann Phys Rehabil Med 60(6): 393-402.
-
Hesse S, Luecke D, Jahnke MT, Mauritz KH (1996) Gait function in spastic hemiparetic patients walking barefoot, with firm shoes, and with ankle-foot orthosis. Int J Rehabil Res 19(2): 133-141.
-
Pépin A, Norman KE, Barbeau H (2003) Treadmill walking in incomplete spinal-cord-injured subjects: 1. Adaptation to changes in speed. Spinal Cord 41(5): 257- 270.
-
Ladouceur M, Barbeau H (2000) Functional electrical stimulation-assisted walking for persons with incomplete spinal injuries: longitudinal changes in maximal overground walking speed. Scand J Rehab Med 32(1): 28-36.
-
Lehmann JF, Condon SM, de Lateur BJ, Price R (1986) Gait abnormalities in peroneal nerve paralysis and their corrections by orthosesL biomechanical study. Arch Phys Med Rehabil 67(6): 380-386.
-
Abel MF, Juhl GA, Vaughan CL, Damiano DL (1998) Gait assessment of fixed ankle-foot orthoses in children with spastic diplegia. Arch Phys Med Rehabil 79(2): 126-133.
-
Lehmann JF, Esselman PC, Ko MJ, Smith JC, deLateur BJ, et al. (1983) Plastic ankle-foot orthoses: evaluation of function. Arch Phys Med Rehabil 64: 402-407.
-
Franceschini M, Baratta S, Zampolini M (1997) Reciprocating gait orthoses: a multicenter study of their use by spinal cord injured patients. Arch Physical Med Rehabil 78(6): 582-586.
-
Massucci M, Brunetti G, Piperno R (1998) Walking with the advanced reciprocating gait orthosis (ARGO) in thoracic paraplegic patients: energy expenditure and cardiorespiratory performance. Spinal Cord 36(4): 223- 227.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial