Evaluation of Seated Trunk Postural Control in Patients with Spinal Cord Injury: Systematic Review of Literature
Background: SCI patients have impairments of postural trunk control in sitting position. Aim: To compare the different evaluation scales of trunk postural balance in sitting position in patients with SCI, to elect the best EBM one. Methods: A systematic review of literature in accordance with PRISMA statement was conducted, using the PICO model for the clinical query. Articles were searched in: PubMed, Medline, Cochrane database, PEDro, EBS base index. RCTs/cohort studies concerning scale for the assessment of seated postural trunk control in patients with SCI were included. Methodological quality was evaluated using New Castle-Ottawa Scale. Results: Ten studies were selected for the final phase of the review. A total of 13 tools to evaluate postural trunk control in the sitting position emerged: 4 for chronic SCI, 8 for acute SCI and 1 for paediatric patients. No scale has been fully investigated in terms of reliability, validity, responsiveness or reproducibility. Discussion: None of the 13 rating scales can be defined as gold standard. TCT-SCI is valid and reliable for acute SCI. Furthermore, it is useful to predict independence and walking. The FIST-SCI is the most reliable scale for patients with chronic SCI, although it may present practical limits in home setting.
Introduction
Spinal cord injury (SCI) is the interruption of the ascending and descending pathways of the spinal cord, with temporary or permanent change of the normal motor, sensory or autonomic functions below the level of injury [1].
The severity and classification of the SCI are defined by the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) created by the America Spinal Cord Injury Association (ASIA) in collaboration with the International Spinal Cord Society (ISCOS) [1].
The trunk stability in sitting position has a main influence on clinical and functional status of SCI patients: a worse trunk control is associated with a lower level of functional independence, a worse quality of life and a greater risk of falls [2, 3]. Consequently, one of the fundamental objectives of rehabilitation in the patient with SCI is the recovery of postural control in the sitting position [4]. It is necessary to perform a correct balance assessment to plan effective programs aimed at recovering the seated postural stability, to monitor changes in functional status and to identify people with greater risk of falls.
Several examples of measures, instruments or scales used to evaluate seated postural control in patients with are reported in the literature, but it has not yet been defined which is the gold standard that allows to evaluate the ability of individuals to (1) maintain a posture (static stability), (2) to maintain balance control during voluntary movements (proactive control), and (3) to regain control after an unexpected loss of balance (reactive stability), in sitting position without the support of the upper limb [5, 6].
Instruments, such as the force platform for the detection of the centre of pressure (COP) [7] or electromyography (EMG) [8], allow an objective and precise assessment of the trunk control in patients with SCI.
However, the equipment used for these examinations is expensive and unsuitable in clinical settings, where are required tests or rating scales quick and easy to administer. Therefore, starting from the need for rapid and valid tests for the evaluation of postural trunk stability in the clinical setting, the objective of this review is to compare the different scales that measure the seated trunk control in patients with SCI to select the best one in light of the latest EBM data.
Methods
A systematic review of the scientific literature in accordance with the Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines was conducted [9].
RCTs or cohort studies concerning scale for the assessment of seated postural trunk control in patients with SCI were included. These studies required a minimum sample of ten participants to be included in this review. According to the exclusion criteria, publications other than RCTs or cohort studies with sample smaller than 10 patients were excluded.
The scientific evidence was researched in the following databases: PubMed, Medline, Cochrane database, PEDro, EBS base index. Combinations of the following key words were used: spinal cord injury, trunk control, balance, postural stability. The last access to database dates to 30 August 2020. The results emerged from the research in the scientific database were examined by title and abstract by a researcher to identify those to be included for the subsequent screening of the full text. In case of indecision of the first researcher, a second one examined the abstract to make a final decision. These two performed the analysis of the full texts selecting the scientific evidence matching with the inclusion and exclusion criteria.
Data Extraction
The studies selected for the final phase of this review were translated and carefully analysed to identify statistical significance (p-value), psychometric properties (validity and reliability), responsiveness and interpretability of the scales in the population of patients with SCI.
The three forms of validity of content, criterion and construct were analysed. Reliability was assessed in terms of test-retest, intra- or inter-rater reliability and internal consistency. Responsiveness is the ability of an instrument to detect the change in the construct measured and is a property that reflects the change measured by a tool. Finally, reproducibility was analysed by studying differences in scores between subgroups, floor and ceiling effects and the minimum detectable change (MIC).
Quality Assessment
The methodological quality of the studies was evaluated using the New Castle-Ottawa Scale (NOS) [10].
Results
Following the application of the search strategy within the different database, studies were identified according to the path described in the PRISMA Statement flowchart (Figure 1).
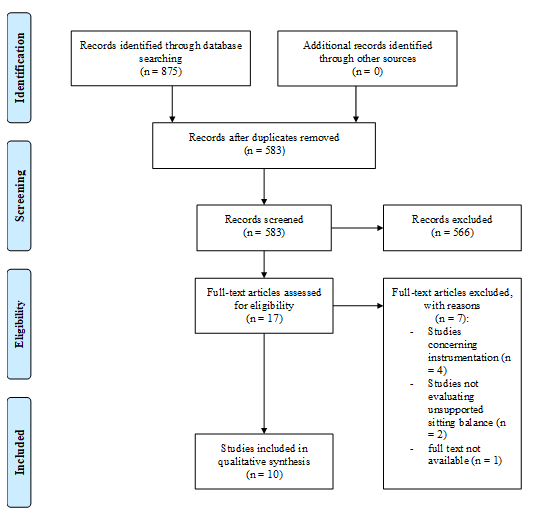
The overall searches revealed a total of 875. After the elimination of duplicates (292), the remaining 583 articles were analysed reading the title and abstract. After screening by title and abstract, most of the studies (566) were excluded,
- because they did not match the inclusion criteria, while the remaining 17 full-text were analysed. Of these 17 studies, in one case it was not possible to obtain a full text [11]. n°
- Date
- Author
- Title
- Journal
- 1
- 2014
- J Quinzaños, et al. [12]
- Proposal and validation of a clinical trunk control test in individuals with spinal cord injury
- Spinal Cord
- 2
- 2011
- CB Pastre, et al.
- [13]
- Validation of the Brazilian version in Portuguese of the
- Spinal Cord
- Thoracic-Lumbar Control Scale for spinal cord injury
- 3
- 2009
- CL Boswell-Ruys, et al. [14]
- Validity and Reliability of Assessment Tools for Measuring
- Unsupported Sitting in People with a Spinal Cord Injury
- 4
- 2019
- L Abou, et al.
- [15]
- Reliability and validity of the function in sitting test among non-ambulatory individuals with spinal cord injury
- The Journal of Spinal Cord
- Medicine
- 5
- 2011
- V Jørgensen, et al. [16]
- Assessment of unsupported sitting in patients with spinal cord injury
- Spinal Cord
- 6
- 2016
- G Wadhwa, et al.
- [17]
- Development, validity and reliability of the ‘Sitting Balance
- Measure’ (SBM) in spinal cord injury
- Spinal Cord
- 7
- 2020
- AE Palermo, et al. [18]
- Psychometric Testing and Clinical Utility of a Modified Version of the Function in Sitting Test for Individuals with Chronic SCI
- 8
- 2007
- S Sprigle, et al.
- [19]
- Development of Valid and Reliable Measures of Postural
- Stability
- The Journal of Spinal Cord
- Medicine:
- 9
- 1998
- SM Lynch, et al.
- [20]
- Reliability of Measurements Obtained with a Modified
- Functional Reach Test in Subjects with Spinal Cord Injury
- Physical Therapy
- Sensitivity to change and responsiveness of the Segmental
- Assessment of Trunk Control (SATCo) in children with spinal cord injury
- 10
- 2018
- LC Argetsinger, et al. [21]
Table 1: CT included in the review.
Methodological Quality
As shown in Table 2, most of the evidence included in this review showed high methodological quality (NOS score ≥ 7), with the exception of three studies16,17,20 for which methodological quality was rated as “ fair “(NOS score = 4-6).
| n° | Author | Item Selection | Item Comparability | Item Result |
|---|---|---|---|---|
| 1 | J Quinzaños, et al. [12] | ✭✭✭ | ✭✭ | ✭✭ |
| 2 | CB Pastre, et al. [13] | ✭✭✭ | ✭✭ | ✭✭✭ |
| 3 | CL Boswell-Ruys, et al. [14] | ✭✭✭✭ | ✭✭ | ✭✭✭ |
| 4 | L Abou, et al. [15] | ✭✭✭✭ | ✭✭ | ✭✭✭ |
| 5 | V Jørgensen, et al. [16] | ✭✭✭ | ✭✭ | ✭ |
| 6 | G Wadhwa, et al. [17] | ✭✭ | ✭ | ✭ |
| 7 | AE Palermo, et al. [18] | ✭✭✭ | ✭✭ | ✭✭ |
| 8 | S Sprigle, et al. [19] | ✭✭✭✭ | ✭✭ | ✭✭ |
| 9 | SM Lynch, et al. [20] | ✭✭ | ✭✭ | ✭✭ |
| 10 | LC Argetsinger, et al. [21] | ✭✭✭ | ✭✭ | ✭✭✭ |
Table 2: Methodological quality according to the New Castle-Ottava Scale (NOS).
Instruments
The following 13 assessment tools for seated trunk control in subjects with SCI emerged from the analysis of the full-texts included in this review: Trunk Control Test for Spinal Cord Injury (TCT-SCI)12, Thoracic-Lumbar Control Scale for Spinal Cord Injury (TLCS-SCI)13, Set of Assessment Tools for Measuring Unsupported Sitting14, Function in Sitting Test (FIST)15, modified Motor Assessment Scale (mMAS)16, modified Sitting Balance Score (mSBS)16, Sitting Balance Measure (SBM)17, modified Function in Sitting Test (FIST-SCI)18, Functional Reach (FR)19, Reach Area (RA)19, Bilateral Reach (BR)19, modified Functional Reach Test (mFRT)20, Segmental Assessment of Trunk Control (SATCo) [21].
These scales were divided into instruments tested on patients with acute SCI (time since injury <12 months) and individuals with chronic SCI (time since injury> 12 months) based on the time since injury.
In addition, the study by Argetsinger, et al. [21] was considered separately, as it is the only one to have analysed a specific rating scale for paediatric patients.
The SBM17, FIST15, FIST-SCI18, SATCo 21 scales are the only ones to evaluate all domains of postural trunk control, testing static, proactive and reactive dynamic postural stability. Furthermore, FIST and FIST-SCI are the only two scales that evaluate postural stability integrating the motor function with the sensory function: participants are asked to perform activities or to maintain the position with both eyes open and closed. The other scales evaluate only one or two of the three domains of equilibrium. The TLCS-SCI13 presents an item for the evaluation of standing postural stability while testing the static and proactive balance in the sitting position,
Scale for Acute Patients
The TCT-SCI12, SATMUS, mMAS16, mSBS16, SBM17, FR19, RA19 and BR19 tools have been tested acute SCI.
Only one study did not report specific characteristics of the subjects included in the sample. The number of participants ranged from 30 to 177 with a total of 294 individuals with SCI included in the studies. The neurological level ranged between C5 and S1 and the degree of injury varied from AIS A to AIS D according to the ASIA Impairment Scale (AIS) [22]. The age of the participants ranged between 15 and 81 years.
Two studies Quinzaños, et al. and Adhwa G, et al. [12, 17] analysed the reliability of the respective evaluation scales by defining the internal consistency through the calculation of the Cronbach alpha coefficient (Cα): both TCT-SCI12 (Cα = 0.979) and SBM17 (Cα = 0.967) have a high internal consistency. None of the authors reported intra-rater reliability. However, two studies12,16 evaluated the inter- rater reliability by calculating the weighted kappa (kw) of TCT-SCI12 (kw = 0.987) and mMAS16 (kw = 0.83-0.91) and mSBS16 (kw = 0.69-0.96), respectively.
In addition, a high test-retest reliability of the TCT-SCI12 was confirmed through the calculation of the weighted k (kw = 0.999; p = 0.001). On the other hand, both Sprigle et al.19 and Boswell-Ruys, et al. [14] analysed the test-retest reliability of the respective scales calculating the interclass correlation coefficients (ICC). Test-retest reliability was classified fair to good for the FR, RA and BR (ICC: FR = 0.858, RA = 0.705, BR = 0.725) and for the anterior and lateral sway of the upper-body sway (respectively, ICC = 0.51 and 0.72), while the maximal distance of the upper-body sway and the alternating reach, maximal balance range, coordinated stability, seated reach, and t-shirt test differed showed an excellent test-retest reliability (ICC range 0.79 –0.91) [14, 19].
Only Quinzaños et al.12 defined overall the criterion, content and construct validities of the TCT-SCI. This scale was rated by four rehabilitation specialists with experience in evaluating patients with impaired trunk control to define the content validity. Similarly, the SBM17 scale was reviewed by a group of three occupational therapists to establish its content validity.
Furthermore, the content validity ratio (CVR) was calculated for each item. Data obtained were compared with the values of the Lawshe 23 table and 12 items were eliminated having an insufficient CVR (<0.42),. The other evaluation methods were analysed solely in terms of criterion or construct validity, but not of content validity.
Regarding criterion validity, Quinzanos, et al. [12] demonstrated that TCT-SCI is sensitive to change. Specifically, the probability of having an adequate trunk control (TCT-SCI score ≥ 13) increases 1,864 times for each additional point in the test, in relation to a sensitivity of 92.2% and a specificity of 98%.
The construct validity of the TCT-SCI12 was evaluated by calculating the Pearson’s correlation coefficient (r), which demonstrated a strong positive correlation between the proposed scale and the la SCIM24 (r = 0.873; p = 0.001) and a weak positive correlation with the time since injury (r = 0.437; p = 0.001).
The construct validity of the SATMUS 14 was evaluated demonstrating the association of the tests with the scores of the ASIA1 scale through the Spearman’s coefficient (s).
Most of the tests were significantly correlated to the sensory scores and motor of the ASIA1 scale. However, the seated reach test has a significant correlation only with the motor score, while the upper-body sway is poorly correlated with both the motor and sensory levels of the ASIA1 scale.
In addition, the Pearson’s correlation coefficient (p) has shown the existence of significant correlations between all tests (p <0.05), except for some components of the upper-body sway test. The strongest correlations were found between the coordinated stability test A and the “put-on” component of the t-shirt test (r = 0.79; p> 0.01), the coordinated stability test B and the supported alternating reach test (r = 0.72 ; p> 0.01) and all directions of the seated reach test with the maximal balance range test (r = 0.60–0.80; p <0.01). There are also significant correlations between the components of each test (r = 0.59-0.98; p> 0.01). The strongest correlations are evident within the alternating reach test (r = 0.93; p <0.01) and the t-shirt test (r = 0.86-0.96; p <0.01). Similarly, Wadhwa, et al. [17] defined the inter-item relationships of the SBM by calculating the Pearson’s correlation coefficient (r), whose values ranged from 0.35 to 0.99.
Jorgensen, et al. [16] decided to calculate the Spearman’s correlation coefficient analysing the relationships between the mMAS and the mSBS and the neurological level, the AIS [22, 23, 24], the time since injury and two functional assessment scales, the Five Additional Mobility and Locomotor Scale (5AML) [25] and the items 9 to 13 of the Functional Independence Measure (FIM) Linacre JM, et al. [26] to evaluate the construct validity of these two scales. The correlation between mMAS and mSBS was high for all testers (s = 0.78, 0.85 and 0.77). Correlation with neurological level was low for mSBS (s = 0.19–0.37) and moderate for mMAS (s = 0.43–0.51). Correlations for mMAS or mSBS with the AIS ranged from moderate to high (s = 0.57– 0.68). However, correlations between time since injury and mMAS (s = 0.14– 0.21) or mSBS (s = 0.24–0.26) were low. Both mMAS and mSBS showed low to high correlation (s = 0.13–0.68) with 5AML and FIM items.
Sprigle, et al. [19] analysed the possible correlation between the achievement measures (FR, RA, BR) and the score obtained in the tests for ADL calculating the Pearson’s correlation coefficient to evaluate the construct validity: only the BR has a significant correlation with the patients’ ADL performance (r = 0.583).
Scale for Chronic Patients
The TLCS-SCI13, FIST15, FIST-SCI18 and mFRT20 scales have been tested on patients with acute SCI. The number of participants ranged from 22 to 38 with a total of 124 individuals with SCI recruited for studies. The neurological level ranged between C1 and L3 and the degree of injury varied from AIS A to AIS D according to the AIS. Participants’ age ranged between 18 and 61 years.
Except for mFRT20, the internal consistency of all other scales was reported calculating the Cronbach’s alpha coefficient (Cα). According to the results, the internal consistency is high for the TLCS-SCI13 (Cα = 0.934) and the FIST-SCI18 (Cα = 0.94) and satisfactory for the FIST15 (Cα = 0.81).
Only two studies13,18 have evaluated the inter- and intra-rater reliability of the respective instruments defining the interclass correlation coefficients (ICC). Statistical analysis showed that both TLCS-SCI13 (respectively ICC = 0.986; ICC = 0.961) and FIST-SCI18 (respectively, ICC = 0.985; ICC = 0.983) have excellent inter- and intra-rater reliability. Th FIST15 (ICC = 0.95, p <0.01) and the mFRT20 (ICC = 0.85- 0.93) have excellent test-retest reliability according to the calculation of the interclass correlation coefficients (ICC). Finally, the analysis of the ROC curve established that the FIST-SCI18has a sensitivity of 92% and a specificity of 92% with a cut off score of 45 points.
None of the authors analysed the content validity of the respective scales. Three studies13,15,18 have evaluated construct validity, but using different methods or demonstrating for different correlations.
Pastre, et al. [13] analysed the construct validity calculating the Spearman’s correlation coefficient (s), whose values show that TLCS-SCI13 was highly correlated with the ASIA1 sensory score (s = 0.83, p = 0.001) and moderately to the total score of the FIM26 (s = 0.64, p = 0.001).
Pearson’s correlation coefficient (r) showed that the FIST15 is moderately correlated with the lateral mFRT (r = 0.64, p <0.001), however no correlation with the anterior mFRT was found (r = 0.16, p = 0.42) and not even with the results of posturography (r = 0.23, p = 0.25). Palermo, et al. [18] defined the construct validity demonstrating the correlation between the FIST-SCI and the level of injury or the modified Motor Assessment Score (mMAS)16 by calculating the Spearman’s correlation coefficient (s): mean FIST-SCI18 scores are moderately correlated with lesion level (s = 0.507; p <0.05) and mMAS16 scores (s = 0.522; p <0.05).
Among the studies that analysed the evaluation scales of postural trunk control in patients with chronic SCI, only two15,18 determined the reproducibility. Analysis of the statistic of the FIST-SCI18 revealed a standard error (SEM) measure of 1.3 and a minimum detectable change (MDC) of 3.5. The reproducibility of the FIST15 was ensured by an SEM of 1.45 and an MDC of 4.
Scale for Paediatric Patients
The Argetsinger, et al. [21] study was the only one which analysed a rating scale for postural trunk control in paediatric patients. Authors introduced SATCo21 as outcome measure for neuromuscular recovery in children with SCI included in a rehabilitation program. A sample of 21 subjects was collected from an outpatient rehabilitation program. The mean age was 63.3 months (range 17-142 months). According to the AIS22 classification, 6 participants had an AIS A degree of injury, 5 AIS B, 3 AIS C and 7 were not classified because they were less than 6 years old. Nine subjects presented cervical lesions and twelve thoracic lesions.
Participants were evaluated from the moment of beginning and after every 20 rehabilitation sessions within 3 months of daily therapy, to assess the sensitivity to change in the SATCo and to compare its responsiveness with other outcome measures (Pediatric Balance Test, Modified Functional Reach, Timed Short Sit Test, Timed Long Sit Test, Timed Stand Test, 2-Minute Walk Test) [21].
From one evaluation to the next, there was an average two-point change in the SATCo. In both the chronic and acute patient groups, the average score varied by 6 points from the initial assessment to the last and 2 points from one measurement to the next. Compared with other outcome measures, the SATCo showed the best responsiveness to change from the first to the last evaluation. The calculation of the post hoc power of responsiveness has shown a power of 99.9% for evaluations between the first and fourth, 97% between the first and third and 82.3% between the first and the second.
Discussion
This systematic review was conducted following the PRISMA guidelines. In total, 13 tools to assess seated trunk control in individuals with SCI emerged.
Among the scales tested on patients with acute SCI, the TCT-SCI12 has been tested on a sample 3-5 times larger than all others. This suggests that the related information may be more reliable and representative of the SCI population.
Comparing the measurement properties of the psychometric characteristics in common, in accordance with the findings of Qizanos, et al. [27], the TCT-SCI12 is the most complete and reliable evaluation scale, as it has the best reliability in terms of internal consistency, test-retest and inter-rater reliability.
All the other assessment tools have lower values of both internal consistency and test retest or inter-rater reliability.
However, the assessment of intra-rater reliability is not reported in the study by Quinzaños, et al. [12]. This lack represents a relatively significant limitation considering that for all other scales no internal consistency and / or test- retest, intra- or inter-rater reliability have been determined.
Only two studies Quinzaños J, et al. and Adhwa G, et al. [12, 17] have demonstrated content validity illustrating the different development stages of TCT-SCI12 and SBM17, respectively. In addition, Quinzaños et al.12 were the only authors to have analysed the criterion validity demonstrating the ability of TCT-SCI to differentiate between patients with postural stability or instability. Specifically, the probability of having an adequate trunk control (TCT-SCI score ≥ 13) increases by each additional point in the test, in relation to an extremely high specificity (92.2%) and sensitivity (98%).
All studies demonstrated construct validity calculating Spearman (s) or Pearson (r) correlation coefficients. TCT- SCI12 has a strong positive correlation with the SCIM24. Given the high correlation, TCT-SCI could be administered in association with the SCIM to allow a more complete assessment of the patient’s functional status. All the other scales present Spearman and / or Pearson coefficients with fluctuating values, demonstrating a variable and generally poor construct validity.
Furthermore, a following study by Quinzaños, et al. [27] demonstrated that TCT-SCI is useful for providing a prognosis of independence and walking in individuals with SCI, independently of the neurologic level and the severity of the injury.
Finally, except for the other scales, some tests of the SATMUS14 have a low practicality in the clinical setting because they require procedures that are not ideal for clinical practice: a 40 cm rod was used fixed to the chest of the patients at the level of the armpit on the horizontal plane of the body, with a pen positioned at the end of the bar itself, which recorded the movement of the trunk on a graph sheet positioned on a small table to quantify the oscillations in the upper-body sway, the distance in the maximal balance range or follow a path in the coordinated stability test.
The FIST15 and the FIST-SCI18 represent the two most complete tools among the assessment scales of postural trunk control tested on patients with chronic SCI because they allow to measure all the domains of balance. Furthermore, they are the only two scales that assess postural stability integrating the motor function with the sensory function. The TLCS- SCI13-item for standing balance assessment represents a huge limitation for a valid and reliable evaluation of seated trunk postural control: patients unable to reach and maintain the standing position have lower score, even if they may show an excellent balance in the sitting position.
According to the available data, the FIST-SCI18 is the most reliable scale since it has the best internal consistency compared to the TLCS-SCI13 and the FIST15. Furthermore, both the FIST-SCI18 and the TLCS-SCI13 have excellent inter-and intra-rater reliability according to the values of the interclass correlation coefficients (ICC). However, neither scale was analysed in terms of test-retest reliability, unlike the FIST15 and the mFRT20, which have excellent test- retest reliability. Furthermore, the analysis of the ROC curve established that the FIST-SCI18has a sensitivity of 92% and a specificity of 92%.
None of the studies analyzed the content validity of the respective scales, but three studies Pastre, et al. [13], Pastre CB, et al. [15], Palermo AE, et al. [18] evaluated construct validity. Pastre, et al. [13] were the only ones to have considered a correlation with a scale that assessed autonomy in functional activities (FIM26). For the other tools, the lack of correlation with scales for the level of independence represents an important limitation, since one of the fundamental elements to be evaluated and to work on in physiotherapy for patients with chronic SCI is the level of functional independence in daily life activities.
According to the values of the Spearman’s correlation coefficient (s), the TLCS-SCI15 is highly correlated to the ASIA1 sensory score and moderately to the FIM26 total score; while the mean scores of the FIST-SCI20 are moderately correlated to the level of injury and to the scores of the mMAS16. According to the values of Pearson’s correlation coefficients (r), the FIST was moderately correlated with the lateral reach of the mFRT, however no correlation was found with the anterior mFRT nor with the results of posturography [17].
The reproducibility of FIST17 and FIST-SCI20 was guaranteed by the values of the standard error measure (SEM) and the minimal detectable change (MDC).
Assessment tolls for patients with chronic SCI should demonstrate good practicability in the home setting. All the proposed scales are adequate, as they require essential and easily available equipment in any home. However, except for the mFRT20, all other measure are performed on the bed and therefore may be slightly influenced by the type of mattress or by the inability to vary the height of patient’s bed.
SATCo21 was the only evaluation scale for postural trunk control tested on paediatric patients with SCI. In the study by Argetsinger, et al. [21] an analysis of validity and reliability is not reported, but only the responsiveness of the SATCo is presented. In comparison with other outcome measures, the SATCo showed the best responsiveness to change from the first to the last evaluation. The calculation of the post hoc power of responsiveness showed a power of 99.9% for the evaluations between the first and the fourth, 97% between the first and the third and 82.3% between the first and the second.
Limitations and Strength
Discussions and conclusions contained in this review are based on studies that are good in terms of methodological quality according to the New Castle Ottawa-Scale (NOS)10. This work was conducted with a complete adherence to international statements (PRISMA statement9) and no study or publication bias were committed, as no meta-analytic mathematical syntheses were performed and there are no conflicts of interest with the authors of the included studies. The populations of the included papers are homogeneous and represent a highly representative statistical sample of the SCI population.
Despite the different strengths, this review also presents weaknesses: there are no randomized controlled trials (RCTs) in the scientific literature, because the lack of a gold standard for the evaluation of seated trunk control of the patients with SCI did not allow of double-arm RCTs comparing different scales.
Conclusion
To date, none of the 13 scales14-23 for of seated trunk control can be defined as the gold standard for adult o paediatric patients with acute or chronic SCI, as further reliability and validity analyses are required. Starting from this assumption, the TCT-SCI14 is the most valid and reliable tool to determine postural trunk control in the sitting position in individuals with acute SCI. It is ideal for clinical practice because it is fast and easy to reproduce. Given the high correlation of the TCT-SCI with the SCIM24, these two scales could be performed simultaneously to define the patient’s clinical-functional status. Furthermore, it has prognostic validity for functional independence and gait. The FIST-SCI18 allows an evaluation of all domains of sitting balance. In addition, it is the most reliable scale in terms of internal consistency and intra- and inter-rater reliability among the scales for individuals with chronic SCI, despite the limits of practicability in the home.
Declaration of Interest Statement
The authors report no conflict of interest.
Funding Details
No found was obtained for the conduct of this article.
References
-
Kirshblum SC, Burns SP, Biering Sorensen F, Donovan W, Graves DE, et al. (2011) International standards for neurological classification of spinal cord injury (revised 2011). J Spinal Cord Med 34(6): 535-546.
-
Jorgensen V, Butler Forslund E, Opheim A, Franzén E, Wahman K, et al. (2017) Falls and fear of falling predict future falls and related injuries in ambulatory individuals with spinal cord injury: a longitudinal observational study. J Physiother 63(2): 108-113.
-
Whalley Hammell K (2007) Quality of life after spinal cord injury: a metasynthesis of qualitative findings. Spinal Cord 45(2): 124-139.
-
Harvey LA, Ristev D, Hossain MS, Hossain MA, Bowden JL, et al. (2011) Training unsupported sitting does not improve ability to sit in people with recently acquired paraplegia: a randomised trial. J Physiother 57(2): 83- 90.
-
Arora T, Oates A, Lynd K, Musselman KE (2020) Current state of balance assessment during transferring, sitting, standing and walking activities for the spinal cord injured population: A systematic review. J Spinal Cord Med 43(1): 10-23.
-
Abou L, de Freitas GR, Palandi J, Ilha J (2018) Clinical Instruments for Measuring Unsupported Sitting Balance in Subjects with Spinal Cord Injury: A Systematic Review. Top Spinal Cord Inj Rehabil Spring 24(2): 177-193.
-
Karataş GK, Tosun AK, Kanatli U (2020) Center-of- pressure displacement during postural changes in relation to pressure ulcers in spinal cordinjured patients. Am J Phys Med Rehabil. 87(3): 177-182.
-
Sherwood AM, McKay WB, Dimitrijević MR (1996) Motor control after spinal cord injury: assessment using surface EMG. Muscle Nerve 19(8): 966-979.
-
Moher D, Liberati A, Tetzlaff J, Altman DG (2015) Linee guida per il reporting di revisioni sistematiche e meta- analisi : il PRISMA Statement. Evidence 7(6): e1000114.
-
Wells G, Shea B, O’Connell D, Peterson J, Welch V, et al. (2019) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomisedstudies in meta-analyses.
-
Musselman KE, Lemay JF, Walden K, Harris A, Gagnon DH, et al. (2019) The standing and walking assessment tool for individuals with spinal cord injury: A qualitative study of validity and clinical use. J Spinal Cord Med 42(S1): 108-118.
-
Quinzanos J, Villa AR, Flores AA, Perez R (2014) Proposal and validation of a clinical trunk control test in individuals with spinal cord injury. Spinal Cord 52(6): 449-454.
-
Pastre CB, Lobo AM, Oberg TD, Pithon KR, Yoneyama SM, et al. (2011) Validation of the Brazilian version in Portuguese of the Thoracic-Lumbar Control Scale for spinal cord injury. Spinal Cord 49(12): 1198-1202.
-
Boswell Ruys CL, Sturnieks DL, Harvey LA, Sherrington C, Middleton JW, et al. (2009) Validity and reliability of assessment tools for measuring unsupported sitting in people with a spinal cord injury. Arch Phys Med Rehabil 90(9): 1571-1577.
-
Abou L, Sung J, Sosnoff JJ, Rice LA (2019) Reliability and validity of the function in sitting test among non- ambulatory individuals with spinal cord injury. J Spinal Cord Med 18: 1-8.
-
Jørgensen V, Elfving B, Opheim A (2011) Assessment of unsupported sitting in patients with spinal cord injury. Spinal Cord 49(7): 838-843.
-
Adhwa G, Aikat R (2016) Development, validity and reliability of the ‘Sitting Balance Measure’ (SBM) in spinal cord injury. Spinal Cord 54(4): 319-323.
-
Palermo AE, Cahalin LP, Garcia KL, Nash MS (2020) Psychometric Testing and Clinical Utility of a Modified Version of the Function in Sitting Test for Individuals With Chronic Spinal Cord Injury. Arch Phys Med Rehabil S0003-9993(20): 30428-30437.
-
Sprigle S, Maurer C, Holowka M (2007) Development of valid and reliable measures of postural stability. J Spinal Cord Med 30(1): 40-49.
-
Lynch SM, Leahy P, Barker SP (1998) Reliability of measurements obtained with a modified functional reach test in subjects with spinal cord injury. Phys Ther 78(2): 128-133.
-
Argetsinger LC, Trimble SA, Roberts MT, Thompson JE, Ugiliweneza B, et al. (2019) Sensitivity to change and responsiveness of the Segmental Assessment of Trunk Control (SATCo) in children with spinal cord injury. Dev Neurorehabil 22(4): 260-271.
-
Roberts TT, Leonard GR, Cepela DJ (2017) Classifications In Brief: American Spinal Injury Association (ASIA) Impairment Scale. Clin Orthop Relat Res 475(5): 1499- 1504.
-
Lawshe CH (1975) A Quantitative approach to content validity. Pers Psychol 28(4): 563-575.
-
Catz A, Itzkovich M, Agranov E, Ring H, Tamir A (1997) SCIM--spinal cord independence measure: a new disability scale for patients with spinal cord lesions. Spinal Cord 35(12): 850-856.
-
Middleton JW, Harvey LA, Batty J, Cameron I, Quirk R, et al. (2006) Five additional mobility and locomotor items to improve responsiveness of the FIM in wheelchair- dependent individuals with spinal cord injury. Spinal Cord 44(8): 495-504.
-
Linacre JM, Heinemann AW, Wright BD, Granger CV, Hamilton BB (1994) The structure and stability of the Functional Independence Measure. Arch Phys Med Rehabil 75(2): 127-132.
-
Quinzaños Fresnedo J, Fratini Escobar PC, Almaguer Benavides KM, Aguirre Güemez AV, Barrera Ortíz A, et al. (2020) Prognostic validity of a clinical trunk control test for independence and walking in individuals with spinal cord injury. J Spinal Cord Med 43(3): 331-338.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial