Characteristics of Sit-to-Stand from a Western-Style Toilet When Putting on Pants in Patients with Hemiplegia Who are Toilet Independent: A Preliminary Study
Introduction: Studies of independent toileting in hemiplegic stroke patients have examined patients’ ability to perform sit-tostand (STS) motion from a Western-style toilet; however, the characteristics of the STS motion performed in conjunction with pulling up of pants (toileting) remain unclear. This study elucidated the characteristics of toileting based on the differences in the center of pressure (COP), force on the foot sole (foot force), and trunk acceleration during toileting in hemiplegic patients under conditions similar to those of daily life. Methods: Ten male hemiplegic patients participated in this study. Measurements were taken using a foot pressure distribution analysis tool and portable three-dimensional motion analysis tool. Based on video recordings, STS and toileting tasks were divided into four phases (P1–P4), and each phase was analyzed. STS and toileting tasks were evaluated and compared. Results: Eight participants exhibited “Pattern A,” which involved increased displacement of the COP toward the paretic side during toileting compared to that during STS. Two participant exhibited "Pattern B", which involved decreased displacement of the COP toward the paretic side during toileting compared to that during STS. Comparisons between STS and toileting showed that the phase from maximum dorsiflexion to full hip extension (P3) was significantly different for maximum displacement of the COP in the paretic side direction (STS, -4.7 ± 9.17; toileting, 8.6 ± 14.12; p <.05) and the maximum foot force on the paretic side direction (STS, 42.6 ± 6.03; toileting, 53.4 ± 11.25; p <.05). Furthermore, the maximum trunk acceleration, which reflects the magnitude of the force applied to the body, was significantly different in the paretic side direction (STS, 0.04 ± 0.01; toileting, 0.09 ± 0.03; p <.01) and non-paretic side direction (STS, 0.04 ± 0.01; toileting, 0.09 ± 0.03; p <.01). Conclusion: Our findings suggest that the characteristics of toileting and STS differ in hemiplegic stroke patients. Occupational therapists and physiotherapists need to provide independent toileting. Activity instructions to hemiplegic stroke patients that cover the actual toileting motion in addition to the STS motion.
Introduction
Hemiplegic stroke patients highly require toileting independence. Families often describe it as a condition for patients to return home. The series of toilet activities related to excretion require a composite of tasks such as moving, changing clothes, transferring, and hygiene. Reports suggest that toilet activity tasks are ranked from most difficult to least difficult in the following order: putting on pants, opening and closing the door, taking off pants, and changing direction [1]. Moreover, early reports have suggested that toilet activity independence in hemiplegic stroke patients is affected by the following functions in this order: lower limb function, cognitive function, and trunk function [2]. As an index for evaluating activities of daily living (ADL), the Functional Independence Measure (FIM) is often used. The scored items for toilet activity in the FIM include putting on and taking off pants and cleaning the pubic area. They do not include opening and closing doors or transferring to the toilet seat [3]. However, research into toilet motion has emphasized the sit-to-stand (STS) motion from a Western-style toilet. Studies have examined topics such as differences in toilet seat height [4] and standing up from a Western-style toilet using a single cane [5]. Recently, studies have assessed the putting on of pants in a standing posture [6, 7, 8]. Nevertheless, these studies evaluate only a part of the overall composite of toilet activities, with results expected to differ from those of an examination of a series of toilet motions including standing up.
In studies conducted to date, force plates have been widely used to evaluate standing motion. In addition, a systematic review of the standing motion of hemiplegic stroke patients revealed characteristics such as a shift of the trunk toward the non-paretic side, asymmetric weight bearing and knee joint moment, and center of pressure (COP) displacement to the non-paretic side [9]. Recently, some reports have described the use of an accelerometer as an evaluation index for balance and trunk sway during standing motion [10], quiet standing [11], and walking [12].
It is often difficult for a hemiplegic patient to put on and remove pants during toilet motion, even if they can execute a standing motion from the toilet seat. STS with the putting on of pants (toileting) is a dual task. It may increase asymmetry in hemiplegic stroke patients more than STS. This study was designed to compare STS and toileting and elucidate the characteristics of toilet motion based on differences in the COP and force on the sole of the foot (foot force) and trunk acceleration during motion.
Materials and Methods
Participant Information
The participants were 10 male hemiplegic stroke patients recruited at a local hospital. The inclusion criteria were as follows: 1) hemiplegia related to stroke, 2) ability to stand from a Western style toilet, and 3) ability to pull up and pull down pants independently (6 or 7 FIM toileting items). The exclusion criteria were as follows: 1) cognitive dysfunction affecting comprehension of the task, 2) musculoskeletal disorders affecting standing motion, 3) Parkinson’s disease, and 4) higher brain dysfunction that may affect task performance, such as unilateral spatial neglect or attention deficit. The participant characteristics are shown in Table 1. This study was approved by the Ethics Committee of Yamagata Prefectural University of Health Sciences (No. 1809-15) and the Ethics Committee of Yamagata Saisei Hospital (No. 383). Consent was received from participants after written and oral explanations.
| ID | Affected side (Rt/ Lt) | Diagnosis | Age (y) | Sex | Height (cm) | Weight (kg) | Time since onset (months) | Br. stage U/E- Finger- L/E | FMA | BBS | MMSE | Hands used to put on pants | Gait aid | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| U/E | L/E | |||||||||||||
| 1 | Rt | Pontine infarction | 83 | M | 153 | 58.1 | 3 | V-V-V | 54 | 30 | 50 | 28 | Both hands | No |
| 2 | Lt | Putaminal hemorrhage | 54 | M | 171 | 66.3 | 5 | IV-V-IV | 48 | 29 | 52 | 30 | Non Paretic hand | Yes |
| 3 | Rt | Putaminal hemorrhage | 69 | M | 175 | 68.7 | 1 | V-V-V | 54 | 34 | 43 | 20 | Both nonos | No |
| 4 | Rt | Corona radiata and putanmen infaracts | 56 | M | 167 | 70.9 | 30 | IV-V-V | 62 | 20 | 45 | 30 | Non Paretic hand | No |
| 5 | Lt | Thalamic hemorrhage | 45 | M | 163 | 57.5 | 2 | V-V-V | 65 | 34 | 50 | 30 | Both hands | No |
| 6 | Rt | Putaminal hemorrhage | 61 | M | 170 | 82 | 3 | IV-V-V | 52 | 27 | 50 | 30 | Non Paretic hand | Yes |
| 7 | Lt | Thalamic hemorrhage | 58 | M | 169 | 63.1 | 3 | V-V-V | 44 | 31 | 54 | 30 | Both hands | Yes |
| 8 | Rt | Putaminal hemorrhage | 60 | M | 162 | 65.0. | 20 | V-V-V | 57 | 32 | 55 | 30 | Non Paretic hand | No |
| 9 | Lt | Corona radiata and putamen infacts | 48 | M | 170 | 87.2 | 4 | V-V-IV | 50 | 48 | 54 | 30 | Both hands | No |
| 10 | Rt | Basal ganglia and frontal temporal infarcts | 68 | M | 180 | 74.7 | 23 | IV-V-V | 49 | 27 | 53 | 30 | Non Paretic hand | Yes |
| Mean | Rt: 6 | Infarction: 4 | 60.2 | 168.1 | 69.4 | 9.4 | 54 | 29 | 51 | 29 | Both hands: 5 | Y: 4 | ||
| SD | Lt: 4 | Hemorrhage: 6 | 11.1 | 7.4 | 9.7 | 10.6 | 6 | 4 | 4 | 3 | Non Paretic hand: 5 | N: 6 | ||
| Range | 48-83 | 153-180 | 7.5-82 | 1-30 | 44-62 | 20-34 | 43-55 | 20-30 |
Table 1: Characteristics of participants. Brunnstrom recovery stage (Br.stage), Fugl-Meyer Assessment (FMA), Berg Balance Scale (
Experimental Equipment
Participants wore trousers (pants, TR-9A1238JP; Alpine, Inc., Nagoya, Japan) over their underwear (TR- 3R1084UP; Alpine, Inc., Nagoya, Japan). The actual clothes used differed according to waist sizes (S, M, L, 2L, and 3L). The height of the Western-style toilet (TS-FX805P-B; Takara Standard Co., Ltd., Osaka, Japan) (SCS-TS200D-1; Toshiba Corp., Tokyo, Japan) was 42 cm above the floor. Measurements were performed using a foot pressure distribution analysis tool (EM-MP2703; Sakai Medical Co. Ltd., Tokyo, Japan), a portable three-dimensional motion analysis tool (EM-M07; Sakai Medical Co. Ltd., Tokyo, Japan), and two video cameras (C920; Logitech Corp., New York, USA). The motion sensor of the portable three-dimensional motion analysis tool was fixed with a belt at the level of the spinous process of the fourth lumbar vertebra. The video camera was positioned so that the whole body could be photographed in the frontal and sagittal planes. The time resolutions of the foot pressure distribution analysis tool and the portable three-dimensional motion analysis tool were both 100 Hz. The spatial resolution was 16 bits for both. The time resolution of the video camera was 30 Hz. The spatial resolution was 998,400 pixels (1,280 × 780). All devices were synchronized and measured using software (MR3 ver. 3.12; Sakai Medical Co. Ltd., Tokyo, Japan).
Experimental Task
This experiment assessed two types of tasks: Task 1 was STS and Task 2 was toileting.
Task 1 involved standing up without using the upper limbs from a seated position on a Western- style toilet. The examiner instructed the participant to stand up from the sitting position in response to a signal and place his hands next to his body after completing the motion. The following instructions were given regarding the position of the feet: “Please keep your feet in a position that allows you to stand up safely without moving them” and “Do not shift the position of your left and right feet back and forth.” Task 2 involved standing up and pulling up pants from a seated position on a Western-style toilet. The examiner instructed the participant to stand up while pulling up his pants in response to a signal and place his hands next to his body after the motion was completed. The time taken to pull up the pants was defined as the time from when the waist part of pants was positioned on the knee joint to the time when it was positioned beyond the superior anterior iliac spine. The timing of pulling up the pants, motion procedure, and limbs to be used were determined arbitrarily by the participant. The participants were instructed to perform the task as they usually would. The following instructions were given regarding the position of the feet: “Please keep your feet in a position that allows you to stand up safely without moving them” and “Do not shift the position of your left and right feet back and forth.”
Procedure
The participants were allowed to stand on the plate with their feet in the same position they used for normal toilet activity. The examiner calibrated the foot pressure distribution analysis tool and the portable three-dimensional motion analysis tool. Task 1 was performed before Task 2. Each task was measured five times after several practice attempts. The participants rested for 2 min between Task 1 and Task 2.
Data Analysis
Data obtained from each sensor were processed using software (MATLAB 2019a; MathWorks Inc., Natick, Massachusetts, USA). The raw data included noise; hence, a low-pass filter was used. The cutoff frequency was 10 Hz [13].
Separation of STS and Toileting Tasks
Based on the video, both the STS and toileting tasks were classified into four phases (Figure 1). Phase 1 (P1) was the duration from the beginning of any movement of the body to liftoff. Phase 2 (P2) was the duration from liftoff to maximum ankle dorsiflexion. Phase 3 (P3) was the duration from maximum dorsiflexion of the ankle to the full extension of the hip. Phase 4 (P4) was the duration from hip extension to the end of movement [14].
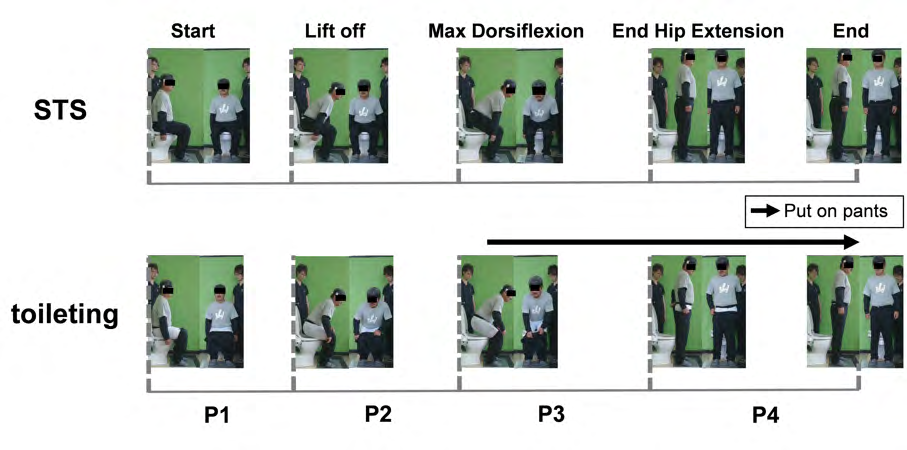
Figure 1: Sit-to-stand from a Western style toilet (STS) and STS during putting on of the pants (toileting) start to end are classified into four phases (P). The figure shows still images from the sagittal plane and the frontal plane at the start and end of P1–P4 each of STS and toileting: P1, from the beginning of any movement of the body to the annulment; P2, from the annulus to the maximum dorsiflexion of the ankle; P3, from the maximum dorsiflexion of the ankle to full extension of the hip; and P4, from the full extension of the hip to the end of the motion. The black arrow in the figure indicates the period from the start to the end of putting on the pants.
Data Calculation and Normalization Processing
The time taken for the entire motion was represented as 100%, with each phase attributed a certain “percent of motion” [15]. The distance from the toe to the heel was defined as the foot length (FL). The distance between the outer edges of both feet was defined as the foot distance (FD) and was calculated using image software (Image J; http:// rsbweb.nih.gov/ij) [16]. From the foot pressure distribution analysis tool, we calculated the anterior–posterior (AP) and medial–lateral (ML) COP displacement and force on the sole of the foot (foot force) applied to the paretic and non- paretic sides. The COP displacement was normalized by dividing the AP direction COP displacement by the FL and the ML direction COP displacement by the FD to remove the influence of individual foot position and foot size [17]. Force on the foot sole was normalized by dividing by the weight of the individual participant to remove the effect of weight on the results [18]. P1 before liftoff was excluded from the measurement restrictions of the foot pressure distribution analysis tool. Data from P2, P3, and P4 were used for analyses. From the portable three-dimensional motion analysis tool, the authors obtained data on trunk acceleration in each of the AP, ML, and vertical directions to determine the magnitude of the force applied to the body.
Statistical Analyses
Measured data from P2 to P4 were analyzed. The maximum values of COP displacement in each direction, foot force on the paretic side and non-paretic side, and trunk acceleration in each direction were processed using statistical analysis software (SPSS ver. 22; SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk test was applied to confirm the presence or absence of normality. The paired Student’s t test was used if the distribution was normal. The Wilcoxon test was used if the distribution was not normal. The significance level of each test was 5%. The effect size was calculated using Cohen’s [19].
Results
Comparison of the Total COP Trajectory
The total COP trajectories projected on the bilateral plantar images of STS and toileting are shown in Figure 2. The difference in the transition of the COP between STS and toileting was distinguishable by two patterns. Those who showed Pattern A had increased displacement of the COP toward the paretic side during toileting compared to STS. In one example (# 1) shown in the upper panel of Figure 2, during STS, the COP trajectory changed on the non-paretic side from start to end. During toileting, however, the COP started almost at the center of the posterior direction, moved forward, backward, left, and right and moved forward from the center at the end. Eight of the 10 participants showed a pattern similar to Pattern A (# 1–8). In eight participants, the COP moved on the non-paretic side during toileting, as in STS; however, in some participants, the COP was temporarily displaced to the paretic side during motion. Participants who showed Pattern B had a greater decrease in the displacement of the COP toward the paretic side during toileting than during STS. In one example (# 9) shown in the lower panel of Figure 2, during STS, the COP trajectory was always on the non-paretic side from start to end. During toileting, the COP always remained on the non-paretic side. The displacement decreased more toward the paretic side during toileting than during STS, increasing the asymmetry. Two out of 10 participants showed a pattern similar to Pattern B (# 9–10).
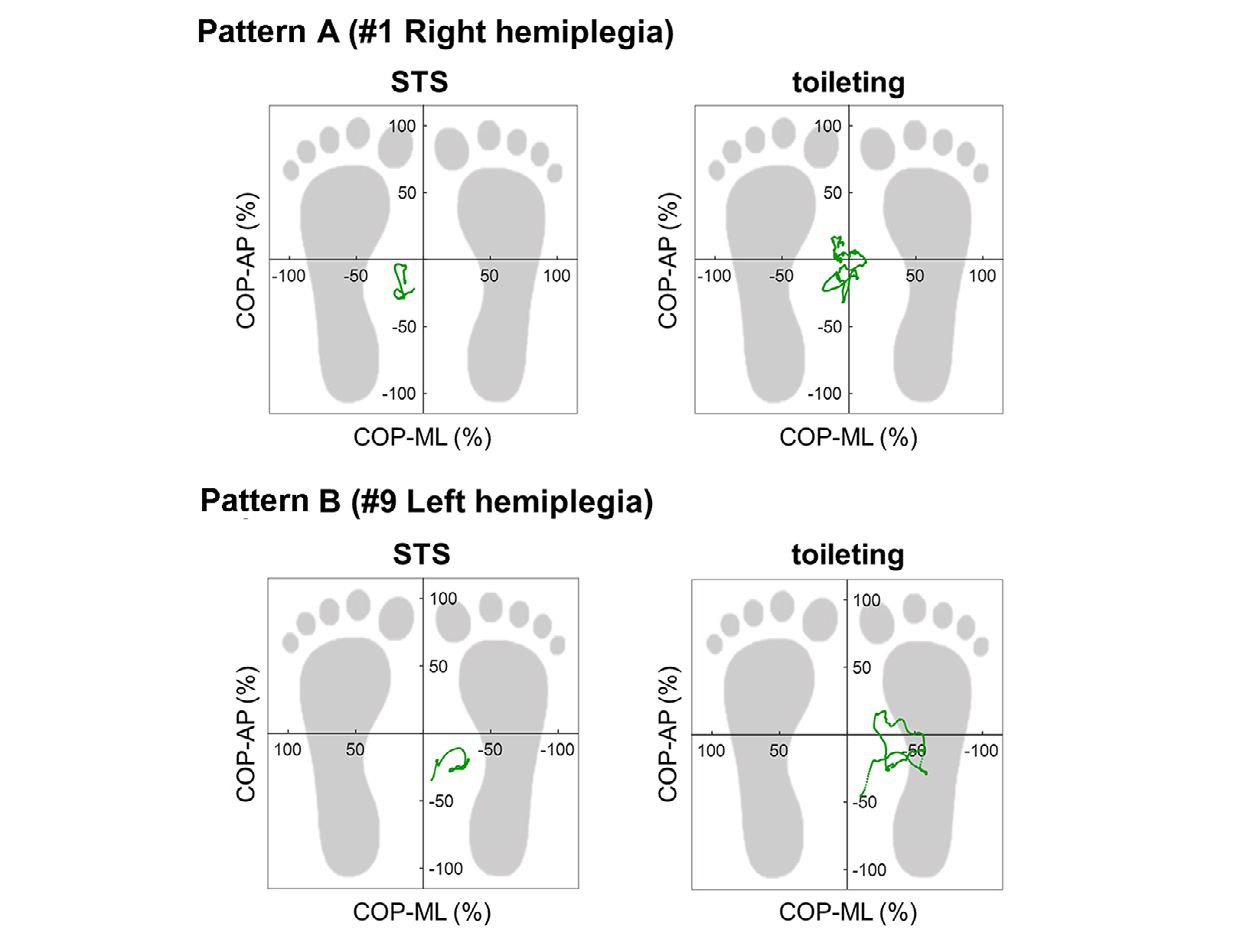
Figure 2: Example showing comparison of the total trajectory of center of pressure (COP). Left and right present STS and toileting, respectively. The horizontal axis represents the normalized COP medial–lateral (ML) transition, with plus denoting the paretic side and minus denoting the non-paretic side. The normalized COP anterior– posterior (AP) transition is shown, with plus denoting anterior and minus denoting posterior.
Transition in the COP, Foot Force, and Trunk Acceleration in Pattern A
The transitions of COP-AP, COP-ML, foot force on the paretic side and non-paretic side, and trunk acceleration (AP, ML, and vertical) in Pattern A are shown in Figure 3. The STS COP-ML remained on the non-paretic side from the start to the end of the motion. However, the COP-ML changed near the center during toileting while the participant pulled up their pants in P3 and P4. At that time, repeated displacement to the paretic side occurred.
Regarding foot force, during STS, values on the non- paretic side were high during all phases, whereas during toileting, foot force values on the non-paretic side were three times the value in P3 and P4. The paretic side showed high values. Trunk acceleration increased and decreased repeatedly while the participant pulled up their pants in P3 and P4 during toileting but not during STS. The amplitude increased in all directions (AP, ML, and vertical); however, the change in the ML direction was the largest.
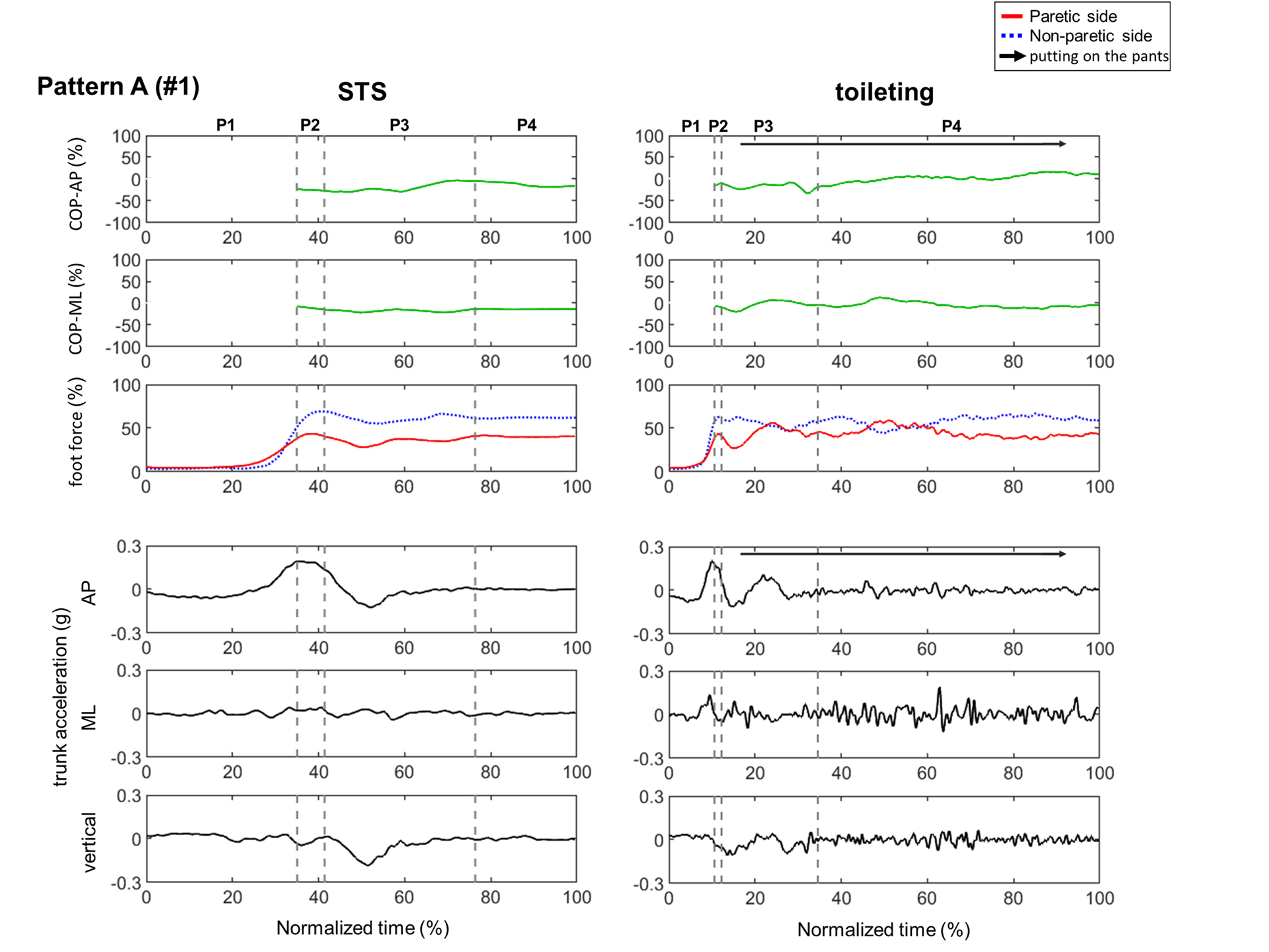
Figure 3: Changes in COP, force on the sole of the foot (foot force), and trunk acceleration in the example showing Pattern A. Left and right show the STS and toileting, respectively. The horizontal axis shows the time required for normalized operation. The vertical axes, respectively, show the changes in COP in the AP directions and ML directions; the changes in foot force on the paretic side and non-paretic side; and the changes in trunk acceleration in the AP, ML, and up–down (vertical) directions. Abbreviations here are used in figure 4.
Transition in the COP, Foot Force, and Trunk Acceleration in Pattern B
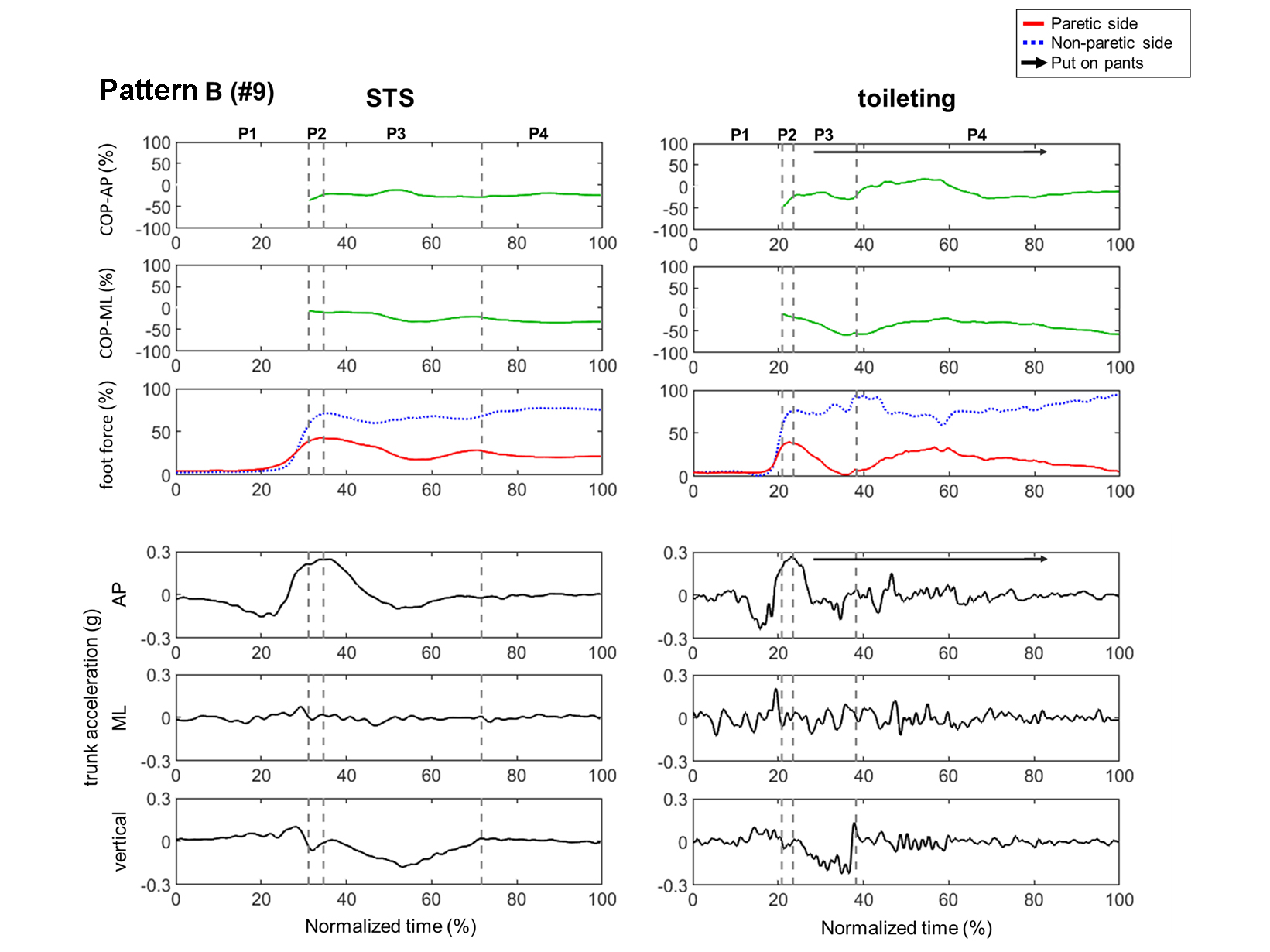
The transitions of COP-AP, COP-ML, foot force on the paretic side and non-paretic side, and trunk acceleration (AP, ML, and vertical) in Pattern B are shown in Figure 4. The results showed that the STS COP-ML always remained on the non-paretic side from the start to the end of the motion.
The toileting COP-ML started from the non-paretic side and then moved further toward the non- paretic side while the participant pulled up their pants in P3 and P4. The foot force on the non-paretic side increased and the foot force on the paretic side decreased during toileting while the participants pulled up their pants in P3 and P4, and increasing asymmetry was noted on the paretic side and non- paretic side during STS. Trunk acceleration increased and decreased repeatedly during the pulling up of pants in P3 and P4 during toileting but not during STS. The amplitude increased in all directions (AP, ML, and vertical), with the amplitude in the ML direction showing the highest value.
Comparison of STS and Toileting for all Participants
The results obtained from the comparison of the STS and toileting tasks are shown in Table 2. The maximum displacement of the COP was significantly different in the non-paretic side direction in P2 (p <.05, d = 0.64). At P3, a significant difference was found in the paretic side direction (p<.05, d = 1.12). At P4, a significant difference was found in the posterior direction (p <.05, d = 1.08) and non- paretic side direction (p <.05, d = 1.04). The maximum foot force was significantly different on the paretic side in P3 (p <.05, d = 1.20). In P4, a significant difference was found on the non-paretic side (p <.01, d = 1.10). The maximum trunk acceleration was significantly different in the posterior direction (p <.05, d = 0.73) in P2. At P3, a significant difference was found in the posterior direction (p <.05, d = 0.49) and paretic side direction (p <.01, d = 2.59), non-paretic side direction (p <.01, d = 2.25), and up direction (p <.05, d = 0.95). At P4, significant differences were found in all directions: anterior direction (p <.01, d = 1.59), posterior direction (p <.01, d = 2.26), paretic side direction (p <.01, d = 2.59), non- paretic side direction (p < .01, d = 2.25), up direction (p <.01, d = 2.76), and down direction (p <.01, d = 4.22).
Maximum COP-anterior (%) P2a -26.4 (13.72) -22.1 (16.70) .103 (0.28) P3a 1.6 (13.39) -1.3 (9.28) .557 (0.25) P4b 0.5 (11.40) 2.9 (9.83) .799 (0.23) Maximum COP-posterior (%) P2a 36.3 (17.07) 38.6 (20.34) .538 (0.12) P3a 35.4 (12.27) 32.8 (15.50) .450 (0.19) P4a 14.6 (8.20) 24.8 (10.48) .019* (1.08) Maximum COP-Paretic side (%) P2b -6.1 (8.14) -8.8 (7.12) .093 (0.35) P3a -4.7 (9.17) 8.6 (14.12) .040* (1.12) P4a -6.0 (10.82) -2.0 (10.37) .333 (0.38) Maximum COP-Non-paretic side (%) P2b 9.4 (8.28) 14.8 (8.69) .039* (0.64) P3b 21.6 (13.66) 25.2 (14.10) .285 (0.26) P4a 14.2 (11.08) 27.0 (13.47) .005 (1.04) Maximum Paretic side foot force (%) P2a 42.0 (6.57) 40.1 (7.04) .098 (0.28) P3b 42.6 (6.03) 53.4 (11.25) .028* (1.20) P4a 41.2 (8.22) 46.3 (9.61) .120 (0.57) Maximum Non-paretic side foot force (%) P2a 62.5 (6.21) 63.9 (7.86) .264 (0.20) P3b 64.4 (6.21) 67.8 (10.35) .508 (0.40) P4a 61.1 (8.06) 71.3 (10.35) .003 (1.10) Maximum Trunk Acceleration-anterior (g) P2a 0.17 (0.06) 0.16 (0.06) .356 (0.17) P3b 0.11 (0.07) 0.11 (0.06) .508 (0.00) P4b 0.02 (0.01) 0.06 (0.04) .005 (1.59) Maximum Trunk Acceleration-posterior (g) P2a -0.10 (0.06) -0.05 (0.08) .029* (0.73) P3a 0.08 (0.03) 0.10 (0.05) .044* (0.49) P4b 0.02 (0.01) 0.06 (0.02) .005 (2.26) Maximum Trunk Acceleration-Paretic side (g) P2a 0.03 (0.03) 0.04 (0.02) .312 (0.49) P3a 0.04 (0.01) 0.09 (0.03) .000 (2.59) P4a 0.02 (0.01) 0.11 (0.04) .000 (3.13) Maximum Trunk Acceleration-Non-paretic side (g) P2a 0.01 (0.02) 0.03 (0.03) .321 (0.79) P3a 0.04 (0.01) 0.09 (0.03) .000 (2.25) P4a 0.02 (0.01) 0.12 (0.03) .000 (4.76) Maximum Trunk Acceleration-up (g) P2a 0.00 (0.04) 0.00 (0.04) .849 (0.05) STS (SD) Toileting (SD) p-value (Cohen’s d)
| P3b | 0.03 | (0.02) | 0.06 | (0.04) | .047* | (0.95) |
|---|---|---|---|---|---|---|
| P4a | 0.02 | (0.01) | 0.07 | (0.02) | .001** | (2.76) |
| Maximum Trunk Acceleration-down (g) | ||||||
| P2b | 0.07 | (0.05) | 0.07 | (0.03) | .878 | (0.00) |
| P3b | 0.12 | (0.04) | 0.12 | (0.05) | .799 | (0.00) |
| P4b | 0.01 | (0.01) | 0.06 | (0.02) | .005** | (4.22) |
Table 2: Comparison of STS and toileting by all participants a Student’s t-test, b Wilcoxon Rank Sum test, * Significant differen
Discussion
Earlier studies have reported that, in hemiplegic stroke patients, standing up induces load asymmetry and COP displacement biased toward the non-paretic side [20, 21]. Therefore, these results suggest that the asymmetry of the COP and load would be further increased during toileting because the task of standing up and pulling up pants is a dual task; however, the results were partially different.
This study specifically examined the pulling up of pants in P3 and P4 during the toileting task. That is, P3 of toileting is a phase in which the body moves upward while raising the pants, and P4 involves pulling up the pants in a standing posture, in an adjusting phase. This shows the process of fitting the pants to the body after pulling them up. In general, it is necessary for the COP to move constantly within the range of physical stability in both the AP and ML directions during walking and ADLs [22]. In this study, our STS results were similar to those of earlier studies [20, 21]. In the toileting task, P2 and P4 tended to increase the asymmetry of foot force and COP displacement compared to the STS task. However, P3 applied a load to the paretic side during the dual task of raising the pants while standing up. The COP was displaced toward the paretic side. Trunk acceleration is often used as an index of body sway [10, 11, 12]. This study demonstrated the magnitude of the force applied to the body during the movement. It is apparent that greater force was generated in each direction during toileting than during STS. During toileting in P3, the task of raising the pants while standing up generates a force on the body in the paretic side direction, causing displacement of the COP in the paretic side direction. In addition, stroke shows weakened muscle strength on the paretic side and decreased joint moment [23] and decreased balance ability [24], suggesting significant findings that make it difficult for hemiplegic patients to perform toileting motion.
In this study, the maximum values of the COP, foot force, and acceleration were used for statistical analysis. Hemiplegic stroke patients used three strategies to avoid falling: stepping, pivoting, and hopping [25]. However, failure of these compensation strategies when the COP deviates from the base of support can lead to falls. Most falls in hemiplegic stroke patients occur during postural changes. Internal factors are often affected by impaired balance, movement, and cognition. The most common places to fall are one’s own room or day room, followed by the bathroom/toilet [26]. Falls occur in hemiplegic patients due to a low rate of increase in force when standing up and a large displacement of the COP [20]. Weight training on the Paretic side reduces STS asymmetry, improves COP displacement and speed, and reduces falls [22]. However, improvement in stroke patients’ balance occurs independent of the paretic side function and load asymmetry [27]. Clinical occupational therapists and physiotherapists provide guidance for improving lower limb function and balance ability to improve basic movements and prevent falls.
Multiple factors, such as lower limb function, cognitive function, and trunk function are involved in independent toilet activity in hemiplegic stroke patients [2]; thus, improvement in each function is crucial, as in basic movement. However, considering that toileting has different task characteristics from those of STS, occupational therapists and physiotherapists must consider the task characteristics of toilet motion and perform training not only for STS motion but also for the actual toilet motion.
One limitation of this study was that all participants were actually able to go to the toilet independently. In addition, whether the magnitudes of the load on the paretic side of the lower limb, COP displacement, and trunk acceleration are directly related to falls remain unclear. Therefore, additional research is needed, including a comparison between healthy subjects and hemiplegic stroke patients and a comparison between independent and non-independent patients.
Conclusions
The comparison between toileting and STS tasks showed that a force is applied to the body in the posterior direction, ML direction, and upward direction when standing up and pulling up pants, thereby causing a load on the paretic side and displacement of the COP in the paretic side direction. This finding suggests that differences in task characteristics between STS and Toileting in individuals with hemiplegia who were independent in toileting. Occupational therapists and physiotherapists need to provide independent toileting activity instructions to hemiplegic stroke patients that cover the actual toileting motion in addition to the STS motion.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Author Contributions HT, YT, and HF conceived and designed the study. HT, YT, NM, KI, HS, ST, and YS participated in data acquisition. HT, NC, and HF analyzed data and wrote the draft of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Acknowledgments We acknowledge the staff of the Department of Rehabilitation at Yamagata Saisei Hospital for cooperating with this study.
References
-
Sakata S, Otaka Y, Sato M, Sakagami S, Kondo K (2015) The difficult components of a toileting task in post- stroke hemiplegia. Sogo Rehabilitation 43: 233-240.
-
Sato A, Okuda Y, Fujita T, Kimura N, Hoshina N, et al. (2016) Cognitive and physical functions related to the level of supervision and dependence in the toileting of stroke patients. PhysTherRes19(1): 32-38.
-
Keith RA, Granger CV, Hamilton BB, Sherwin FS (1987) The functional independence measure: a new tool for rehabilitation. Adv Clin Rehabil 1: 6-18.
-
Lee SK, Lee S.Y (2016) The effects of changing angle and height of toilet seat on movements and ground reaction forces in the feet during sit-to-stand. J Exerc Rehabil 12(5): 438-441.
-
Fujikura M, Fujii H, Kafuku T, Kimura Y, Fukuda E (2012) Sit-to-stand from a toilet seat by hemiplegic subjects using a one-point cane. Phys Occup Ther Geriatr 30(2): 150-164.
-
Koike Y, Sumigawa K, Koeda S, Shiina M, Fukushi H, et al. (2015) Approaches for improving the toileting problems of hemiplegic stroke patients with poor standing balance. J Phys Ther Sci 27(3): 877-881.
-
Hiragami S, Nagahata T, Koike Y (2018) Lower garment- lifting postural control characteristics during toilet- related activities in healthy individuals and a post-stroke hemiplegic patient undergoing rehabilitation. J Phys Ther Sci 30(12): 1462-1467.
-
Torii S, Ishioka T, Koike Y, Hamaguchi T, Nakamura H (2019) Postural stability while standing among clients with hemiparesis during pulling up trousers: A comparison between independent and surveillance groups. Japanese Occup Ther Res 38(6): 654-662.
-
Boukadida A, Piotte F, Dehail P, Nadeau S (2015) Determinants of sit-to-stand tasks in individuals with hemiparesis post stroke: A review. Ann Phys Rehabil Med 58(3): 167-172.
-
Regterschot GRH, Folkersm M, Zhang W, Baldus H, Stevens M, et al. (2014) Sensitivity of sensor-based sit-to-stand peak power to the effects of training leg strength, leg power and balance in older adults. Gait Posture 39(1): 303-307.
-
Mancini M, Horak FB, Zampieri C, Carlson Kuhta P, Nutt JG, et al. (2011) Trunk accelerometry reveals postural instability in untreated Parkinson’s disease. Park Relat Disord 17(7): 557-562.
-
Wada O, Asai T, Hiyama Y, Nitta S, Mizuno K (2017) Root mean square of lower trunk acceleration during walking in patients with unilateral total hip replacement. Gait Posture 58: 19-22.
-
Sekiguchi Y, Kato T, Honda K, Kanetaka H, Izumi SI (2017) Effects of grab bar on utilized friction and dynamic stability when elderly people enter the bathtub. Clin Biomech 47: 7-13.
-
Schenkman M, Rlley P, Mann RW (1990) Whole-body movements during rising to standing from sitting. Phys Ther 70(10): 51-64.
-
Millington PJ, Myklebust BM, Shambes GM (1992) Biomechanical analysis of the sit-to-stand motion in elderly persons. Arch Phys Med Rehabil 73(7): 609-617.
-
Ashnagar Z, Hadian MR, Olyaei G, Talebian MS, Rezasoltani A, et al. (2017) Reliability of digital photography for assessing lower extremity alignment in individuals with flatfeet and normal feet types. J Bodyw Mov Ther 21(3): 704-710.
-
de Haart M, Geurts AC, Huidekoper SC, Fasotti L, van Limbeek J (2004) Recovery of standing balance in postacute stroke patients: a rehabilitation cohort study. Arch Phys Med Rehabil 85(6): 886- 895.
-
Rocha DS, Jose R, Michaelsen SM (2010) Non-paretic lower limb constraint with a step decreases the asymmetry of vertical forces during sit-to-stand at two seat heights in subjects with hemiparesis. Gait Posture 32(4): 457-463.
-
Cohen J (1988) Statistical power analysis for the behavioral sciences. 2nd (Edn,). Hillsdale, NJ: Lawrence Erlbaum Associates.
-
Cheng PT, Liaw MY, Wong MK, Tang FT, Lee MY, et al. (1998) The sit-to-stand movement in stroke patients and its correlation with falling. Arch Phys Med Rehabil 79(9): 1043-1046.
-
Roy G, Nadeau S, Gravel D, Malouin F (2006) The effect of foot position and chair height on the asymmetry of vertical forces during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin Biomech 21(6): 585-593.
-
Cheng P, Wu S, Liaw M, Wong AMK, Tang F (2001) Symmetrical body-weight distribution training in stroke patients and its effect on fall prevention. Arch Phys Med Rehabil 82(12): 1650-1654.
-
Lomaglio MJ, Eng JJ (2005) Muscle strength and weight- bearing symmetry relate to sit-to-stand performance in individuals with stroke. Gait Posture 22(2): 126-131.
-
Tyson SF, Hanley M, Chillala J, Selley A, Tallis RC (2006) Balance disability after stroke. Phys Ther 86(1): 30-38.
-
Honeycutt CF, Nevisipour M, Grabiner MD (2016) Characteristics and adaptive strategies linked with falls in stroke survivors from analysis of laboratory-induced falls. J Biomech 49(14): 3313-3319.
-
Nyberg L, Gustafson Y (1995) Patient falls in stroke rehabilitation. A challenge to rehabilitation strategies Stroke 26(5): 838-842.
-
Laufer Y, Sivan D, Schwarzmann R, Sprecher E (2003) Standing balance and functional recovery of patients with right and left hemiparesis in the early stages of rehabilitation. Neurorehabil Neural Repair 17(14): 207- 213.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial