Satisfaction and Reduction of Pain Following Tele-Physiotherapy of Patients with Musculoskeletal Disorders during the COVID- 19 Pandemic Disorders
Introduction: This study aimed to investigate the rate of satisfaction and pain reduction in musculoskeletal patients by using tele-physiotherapy during the COVID-19 pandemic infection disease. Methods: Eighteen patients with shoulder, knee, neck, and thoracic pain received some advice through video conferencing or video calls. All participants received different exercises based on the patient’s pathology or using some accessible modalities such as cold or hot packs. Interventions were followed by online platforms such as chat/massage and video conferencing by WhatsApp or Telegram program. Pain intensity was assessed by the Numeric Rating Scale, and satisfaction was evaluated by the Telehealth Satisfaction Questionnaire. Results: Statistical analysis showed a significant reduction of pain (p< 0.001), with a high effect size = 2.9. The rate of satisfaction of patients was detected high about all questions. Conclusion: This study suggests that tele-physiotherapy can effectively reduce pain and increase satisfaction during pandemic infected disease or for patients in remote areas.
Introduction
The most significant public health disaster has recently been severe acute respiratory syndrome caused by Coronavirus disease 2019 (COVID-19) [1]. In this situation staying at home and social distancing with limited outpatient Investigation Paper care have been recommended. Thus, an innovative method has been employed to provide physical therapy and rehabilitation for different patients [2, 3]. Accordingly, using Information and Communication Technologies (ICT) for online management and digital-based physiotherapy is safe for patient’s care [2]. Some services that can be provided by tele-physiotherapy during this pandemic are remote assessment, prescription of exercise therapy, and monitoring of progress [3]. Self-management of patients in tele-physiotherapy leads to more patient involvement with positive impacts on the clinical outcomes. However, the lack of adequate skills to use tele Care safely and effectively by patients may be a barrier for some therapists [4].
Previous systematic reviews reported positive experiences, significant clinical outcomes, and high patient satisfaction using tele-physiotherapy [5, 6], even compared to in-person care [7]. Some patients also preferred to receive tele-physiotherapy with a combination of office- based treatment [8]. As respects musculoskeletal disorders (MSDs) are common problems with costly affected both individual and society economic, hence physical functioning, mental status, and quality of life of these patients are also affected. In patients with MSDs, conservative treatment is considered the first-line approach [8]. During the pandemic infection disease, it seems virtual consultations and tele- physiotherapy can be helpful for these patients. Previous studies revealed acceptable results with positive efficiency of telerehabilitation in patients with MSDs, knee arthritis, and pediatric disorders [9, 10, 11]. According to the review article, there were only a few studies and knowledge gaps regarding patient satisfaction, perception, and effect size of telerehabilitation services during COVID-19 pandemic infection disease [12, 13, 14]. The purpose of this study was to evaluate the pain improvement and patient satisfaction after tele-physiotherapy in patients with musculoskeletal disorders.
Materials and Methods
Study Design
Eighteen patients with musculoskeletal disorders referred to the physiotherapy department volunteered to contribute to tele-physiotherapy sessions. This study was approved in Tehran University of Medical Sciences with ethical member IR.TUMS.FNM.REC.1401.015.
Participants
Participants with aged between 15 to 40 years without problem in using videoconferencing at home volunteered to participation in this study. Participants with a history of surgery, neurological or vestibular disorders were excluded from the study. Information about age, gender, systemic illness, specific joint disorders and painful function, the involved joint, pain intensity, and pain duration were collected. After clinical assessment, , a customized treatment protocol includes exercises and some home accessible modalities such as heat/cold pack was designed for each patient based on their situation through WhatsApp or Telegram program.
Before starting physiotherapy, the main problems were discussed with each patient using a 3D anatomy model. Each patient identified their functional goals for the treatment plan. The therapist closely monitored patient movements and actively monitored patients during exercises performed. In some cases, the physiotherapist explained how to perform exercises, or sometimes available videos were sent to the patients. Available equipment at home was also recommended for exercise therapy and monitoring patients’ clinical progress.
The first exercise session was conducted using a videoconferencing tool for all patients, and based on patient condition and convenience, the treatment sessions were conducted daily or every other day. Research Ethics Committee at the XXX University of Medical Sciences and followed the principles of the Declaration of Helsinki.
Outcome measures
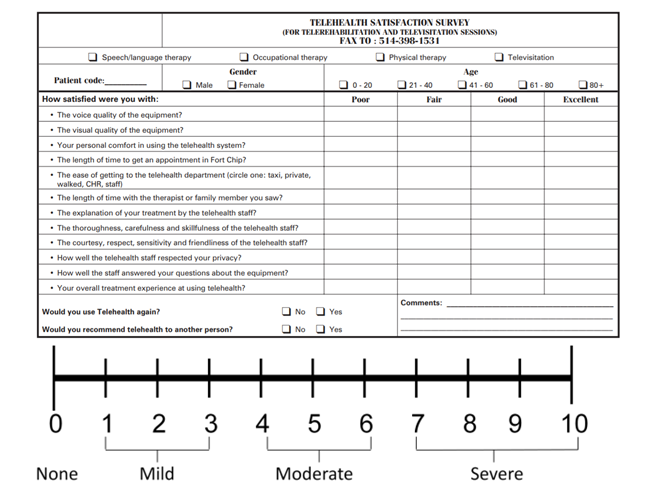
The outcome was measured based on two parameters – pain intensity and patient satisfaction. Pain intensity was assessed by the Numeric Pain Rating Scale (NPRS) at baseline and after 10 sessions by oral description of pain intensity experienced in the last 24 hours [15]. NPRS is an 11-point scale (0 being no pain and 10 being the worst imaginable pain) (Figure 1).
Patient satisfaction was evaluated by Telehealth Satisfaction Questionnaire. These questions were included in Table 2.
The patients answered questions based on 0 to 100% satisfaction. These questions evaluated the patient experience during the intervention sessions. Patient satisfaction and feedback of patients on various aspects of tele-physiotherapy were obtained by some questions designed on Google form questionnaire.
Statistical Analysis
SPSS software (Version 22.0) was used for data analysis. The Wilcoxon signed-rank test was employed to determine NPRS changes. Effect size of pain reduction was calculated by Cohen’s d effect size. Cohen’s d scores equal to 0.20 indicate a small effect, d= 0.50 indicates a medium effect, and d= 0.80 indicates a large effect size [16].
| Gender | Age (year) | Pathology | Pain before treatment | Pain after treatment |
|---|---|---|---|---|
| male | 30 | Low back pain | 6 | 4 |
| male | 18 | Knee pain (ACL partial rupture) | 5 | 3 |
| male | 29 | Shoulder pain (biceps tendinitis) | 7 | 3 |
| male | 27 | Shoulder pain (impingement) | 7 | 3 |
| male | 28 | Shoulder and cervical pain (myofascial pain) | 5 | 3 |
| female | 27 | Shoulder pain (impingement syndrome) | 4 | 2 |
| female | 30 | Knee pain: patellofemoral syndrome (pfps) | 5 | 3 |
| female | 25 | Shoulder pain (scapular dyskinesia) | 4 | 3 |
Table 1: Demographic characteristics of patients and pain score before and after treatment.
- female
- 22
- Shoulder pain (subacromial pain syndrome)
- 5
- 2 female
- 25
- Knee pain (pfps)
- 5
- 2 female
- 27
- Knee pain (knee valgus & pfps)
- 4
- 2
- Male
- 28
- Thoracic spinal pain (hyper kyphosis)
- 5
- 3 female
- 25
- Kyphotic posture + shoulder internal rot
- 5
- 2 female
- 25
- Kyphotic posture + shoulder pain
- 5
- 2 male
- 32
- Knee pain: patellofemoral syndrome (pfps)
- 5
- 2 female
- 38
- Back pain
- 5
- 3 male
- 25
- Kyphotic posture
- 6
- 2 male
- 28
- Back pain
- 5
- 2
Table 2: Demographic characteristics of patients and pain score before and after treatment.
| Question | Percentage |
|---|---|
| The voice quality of equipment? | 85% |
| The visual quality of equipment? | 85% |
| Your personal comfort in using the Telehealth system? | 94% |
| The length of time to get an appointment in Fort Chip? | 87% |
| The ease of getting to the Telehealth department? | 90% |
| The length of time with the therapist or family member you saw? | 89% |
| The explanation of your treatment by the Telehealth staff? | 93% |
| The thoroughness, carefulness and skillfulness of the Telehealth staff? | 85% |
| The courtesy, respect, sensitivity and friendliness of the Telehealth staff? | 97% |
| How well the Telehealth staff respected your privacy? | 89% |
| How well the staff answered your questions about the equipment? | 99% |
| Your overall treatment experience of using Telehealth? | 88% |
Table 3: Of satisfaction (percentage) for different questions from the tele-health questionnaire.
Results
Demographic characteristics, kind of pathologies, and pain intensity (9 males and 9 females with age 27± 0.5) are listed in Table 1. Pain intensity significantly reduced after 10-session of tele-physiotherapy (2.8 ± 0.1) compared to before intervention (5.2 ± 0.2) (p< 0.001). Effect size calculated with Cohen’s d effect size of pain reduction was 2.9, indicating a very large effect size [16]. Table 2 presents patient satisfaction results showing high satisfaction results regarding received tele-physiotherapy.
Discussion
Telehealth and tele-physiotherapy are recommended during pandemic infectious diseases, especially COVID-19 disease. Besides easy access and reduced travel and waiting time, access to high-quality and cost-effective care are other benefits of tele-physiotherapy [17, 18, 19, 20]. Previous research has shown positive effects of cardiac and neurological tele-rehabilitation and the management of patients with depression [21]. Moreover, previous studies confirmed the low to moderate positive effects of tele-physiotherapy in patients with musculoskeletal disorders [22, 23]. A few studies reported significant pain reduction with tele- rehabilitation [24, 25]. In line with previous results, the results of our study confirmed significant pain reduction after tele-physiotherapy and tele-consultation. The mean score of pain in patients at baseline was 5.2, indicating the presence of moderate pain in most of the patients.
Most of the patients suffered from chronic musculoskeletal pain, and treatment sessions ranged from 10 to 12 sessions. Despite various patient characteristics like age, gender, and pain duration, we found a significant pain reduction (mean = 2.8) at the end of treatment (p< 0.001), with a high effect size equal to 15.2. This finding is comparable with previous results [26]. Mundhada (2021) revealed a positive correlation between changes in pain intensity, patient-reported functional goals, and patient satisfaction [26]. Also, patient satisfaction in all questions was above 80%. Comfortable using an online system and quality of image and sound shown greater than 80% satisfaction. The patients also found the virtual interaction easy and useful. Satisfaction percentage regarding experience and treatment method, explanation of physiotherapist about disease and treatment was more than 90%.
Although our results revealed high satisfaction among the patients for tele-physiotherapy, we did not ask patients’ points of view for a combination of hands-on and tele- physiotherapy. For example, parents in pediatric centers prefer a combination of hands-on and remote physiotherapy for their children [10]. There is a lack of evidence about standard ways for delivering telerehabilitation in musculoskeletal disorders. We suppose having one session of hands-on physiotherapy each week to receive some modalities may lead to better results. It seems that if tele- physiotherapy is executed efficiently and effectively, the patients/physiotherapists continue to demand it, and most of the previous barriers to virtual visits will be diminished. Further research for the standardization of tele- physiotherapy and teleconsultation is necessary, and even when the problems with the COVID-19 have ended, it can help and facilitate interventions for musculoskeletal and neurologic disorders.
Limitations
There are several limitations to this paper. The sample size was rather small. There was no follow-up assessment to see if the results could last. Also, the data was gathered during a real-time public health crisis with different pathologies in different age groups; therefore, there was a lack of experimental control and standardized methods. In this study, there was no control group.
Conclusion
In conclusion, it seems tele-physiotherapy effectively reduces pain intensity among patients with musculoskeletal disorders. Moreover, this method was acceptable since the patients ported high satisfaction levels.
References
-
Jin, Y, Haiyan Yang, Wangquan Ji, Weidong Wu, Shuaiyin Chen, et al. (2020) Virology, Epidemiology, Pathogenesis, and Control of COVID-19. Viruses 12(4): 372.
-
Lee A, Karen Finnin, Lesley Holdsworth, Dianne Millette, Chris Peterson (2019) Report of the WCPT/INPTRA Digital physical therapy practice task force. WCPT/ INPTRA Digital Practice Final Report vs 7: p 15.
-
Theodoros D, Russell T (2008) Telerehabilitation: current perspectives. Stud Health Technol Inform 131(1): 191-209.
-
Hinman R, Nelligan RK, Bennell KL, Delany C (2017) “Sounds a Bit Crazy, But It Was Almost More Personal:” A Qualitative Study of Patient and Clinician Experiences of Physical Therapist–Prescribed Exercise For Knee Osteoarthritis Via Skype. Arthritis care & research 69(12): 1834-1844.
-
Lawford B, Delany C, Bennell KL, Hinman RS (2018) I was really sceptical... But it worked really well: a qualitative study of patient perceptions of telephone-delivered exercise therapy by physiotherapists for people with knee osteoarthritis. Osteoarthritis and cartilage 26(6): p. 741-750.
-
Adamse C, Weering MGD, Etten Jamaludin FS, Stuiver MM (2018) The effectiveness of exercise-based telemedicine on pain, physical activity and quality of life in the treatment of chronic pain: A systematic review. J Telemed Telecare 24(8): 511-526.
-
Cottrell MA, Shaun PO Leary, Maree Raymer, Anne J Hill, Tracy Comans (2019) Does telerehabilitation result in inferior clinical outcomes compared with in-person care for the management of chronic musculoskeletal spinal conditions in the tertiary hospital setting? A non- randomised pilot clinical trial. Journal of telemedicine and telecare 27(7): 444-452.
-
Qaseem A, Wilt TJ, McLean RM, Forciea MA (2017) Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians. Ann Intern Med 166(7): 514-530.
-
Xie SH, Wang Q, Wang LQ, Wang L, Song KP, et al. (2021) Effect of Internet-Based Rehabilitation Programs on Improvement of Pain and Physical Function in Patients with Knee Osteoarthritis: Systematic Review and Meta- analysis of Randomized Controlled Trials. J Med Internet Res 23(1): 21542.
-
Otadi K (2021) Satisfaction of patients following online managing and hands- on rehabilitation of patients during the COVID- 19 pandemic in pediatric center 16(1).
-
Latif Zade T, Tucci B, Verbovetskaya D, Bialkin E, Brian Ng, et al. (2021) Systematic Review Shows Tele- Rehabilitation Might Achieve Comparable Results to Office-Based Rehabilitation for Decreasing Pain in Patients with Knee Osteoarthritis. Medicina 57(8): 764.
-
Makhni MC, Riew GJ, Sumathipala MG (2020) Telemedicine in Orthopaedic Surgery: Challenges and Opportunities. J Bone Joint Surg Am 102(13): 1109- 1115.
-
Siow MY, Walker JT, Britt E, Kozy JP, Zanzucchi A, et al. (2020) What was the change in telehealth usage and proportion of No-show visits for an orthopaedic trauma clinic during the COVID-19 pandemic? Clinical Orthopaedics and Related Research 478(10): 2257- 2263.
-
Murphy EP, Fenelon C, Murphy RP, O Sullivan MD, Pomeroy E, et al. (2020) Are Virtual Fracture Clinics During the COVID-19 Pandemic a Potential Alternative for Delivering Fracture Care? A Systematic Review. Clin Orthop Relat Res 478(11): 2610-2621.
-
Seidel HM (2010) Mosby’s Guide to Physical Examination. Elsevier Health Sciences.
-
Cohen J (2013) Statistical power analysis for the behavioral sciences. Academic press.
-
Mars M (2013) Telemedicine and advances in urban and rural healthcare delivery in Africa. Prog Cardiovasc Dis 56(3): 326-335.
-
Xue Y, Liang H, Mbarika V,Hauser R, Schwager P (2014) Understanding Healthcare Professionals’ resistance Of Telemedicine: An Empirical Study In Ethiopia.
-
Heinzelmann PJ, Lugn NE, Kvedar JC (2005) Telemedicine in the future. J Telemed Telecare 11(8): 384-390.
-
Kohnke A, Cole ML, Bush R (2014) Incorporating UTAUT predictors for understanding home care patients’ and clinician’s acceptance of healthcare telemedicine equipment. Journal of technology management & innovation 9(2): 29-41.
-
Holst A, Nejati S, BjOrkelund C, Eriksson MCM, Hange D, et al. (2017) Patients’ experiences of a computerised self-help program for treating depression - a qualitative study of Internet mediated cognitive behavioural therapy in primary care. Scand J Prim Health Care 35(1): 46-53.
-
Mani S, Sharma S, Omar B, Paungmali A, Joseph L (2017) Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: a systematic review. J Telemed Telecare, 23(3): 379-391.
-
Gal N, Andrei D, Nemeş DI, Nadaşan E, Tivadar VS (2015) A Kinect based intelligent e-rehabilitation system in physical therapy, in Digital Healthcare Empowering Europeans. IOS Press 489-493.
-
Fransen M, McConnell S, Harmer AR, Vander Esch M, Simic M, et al. (2015) Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med 49(24): 1554-1557.
-
Doi T, Akai M, Fujino K, Iwaya T, Kurosawa H, et al. (2008) Effect of home exercise of quadriceps on knee osteoarthritis compared with nonsteroidal antiinflammatory drugs: a randomized controlled trial. Am J Phys Med Rehabil 87(4): 258-269.
-
Sheetal M, Preeti M, Rekha K, Divya S,Ashutosh M, et al. (2021) Telerehabilitation for musculoskeletal disorders during the COVID-19 pandemic. International Journal of Physiotherapy and Research 9(1): 3765-3772.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial