Dry Needling and Pain Drawings: An Exploratory Study
Background: Emerging evidence shows that altered cortical brain maps play a key role in the initiation and maintenance of a human pain experience and therapeutic treatments may positively influence these maps and reduce pain and disability. Objective: To determine if dry needling for spinal pain can positively alter body pain diagrams and if those changes correlate to a reduction in self-reported pain ratings. Design: Case series with pre- and immediate post-intervention measurements. Methods: A convenience sample of adult patients attending physical therapy with back or neck pain meeting inclusion criteria for dry needling was recruited for the study. Prior to dry needling, patients completed a demographics questionnaire, filled in a body pain diagram (color where you hurt) and a self-reported pain rating (numeric pain rating scale). Patients then received a standard dry needling session for the affected area and immediately following dry needling completed a body pain diagram, self-reported pain rating and satisfaction with the treatment using the global rating of change scale. Results: Forty-three patients (76.74% female) participated in the study with 19 patients presenting with low back pain and 24 with neck pain. Following dry needling, mean pain rating for the whole cohort was reduced (p<0.001), with larger effect for low back pain (p < 0.001) than neck pain (p = 0.031). Overall, the whole patient sample’s body pain diagram decreased in size by 50.16% following DN (95%CI = 10.8, 22.6; t(42)=5.67, p < 0.001). When broken down between neck and low back pain, low back maps shrunk by 61.84% (95%CI= 16.1 - 38.6), t(18)=5.1, p < 0.001), whereas neck maps decreased by 33% (95%CI= 4.3 - 12.2, t(23)=4.4, p < .001). Positive correlations were found between the size of the body pain drawings and pain intensity (rs = 0.461 (p = 0.002) as well as reduction of pain after dry needling and reduction in body map drawings (rs = 0.305 (p = 0.047). Conclusion: Dry needling can reduce body map drawings, which correlates to the intensity of pain. A potential underlying mechanism of dry needling may be its effect on neuroplasticity. Additional research is needed to further explore these emerging results.
Introduction
In the mid-1990’s evidence-based practice was introduced to healthcare, including rehabilitation [1]. With the introduction of evidence-based practice clinical decision- making was shifted towards treatments backed by evidence, especially higher levels of evidence including meta-analyses, systematic reviews and high-quality randomized clinical trials. Now, armed with research, clinicians could drive treatment choices based on evidence, versus traditional approaches typically rooted in expert opinion [2].
Evidence-based medicine and the resultant increase in research is not just confined to clinical research but has found its way into basic science research. For example, some evidence supports the use of manual therapy, especially high-velocity thrust techniques in a sub-group of patients with low back pain, especially in the acute phase [3, 4, 5]. With the growing evidence for manual therapy for spinal pain, a newfound interest in the mechanisms behind manual therapy emerged. Old, mechanical explanations for the proposed mechanisms soon gave way to new theories, based on the increase in basic science research [6]. Bialosky and colleagues in 2008 published a seminal paper proposing mechanisms of manual therapy including more than just mechanical mechanisms, now including pain-related brain circuitry, pain modulatory circuitry, changes in the central and peripheral nervous system and mechanical influences [7]. In 2018, Bialosky and colleagues updated this model, adding characteristics of the patient and provider [8]. With increased basic science research, a more biopsychosocial viewpoint of manual therapy emerged, which not only allows for a better potential understanding of the underlying mechanisms of manual therapy, but also the potential to enhance clinical trials. For example, it is well established that the physical body of a person is represented in the brain by a network of neurons, often referred to as a representation of that particular body part in the brain [9, 10, 11]. These neuronal representations of body parts are dynamically maintained [12, 13, 14] and changes in shape and size of body maps seem to correlate to increased pain and disability [11, 15]. Emerging research is beginning to strengthen the notion that manual therapy may be a form of sensory discrimination and integration, positively influencing these altered cortical maps and easing pain [16, 17, 18, 19]. Not only has it been shown that patients can understand this neuroplasticity view of manual therapy, but it yields superior results to mechanical explanations for manual therapy [16].
Another treatment often used by physical therapists is dry needling (DN). Emerging and growing evidence seem to support the use of DN for spinal pain, especially low back pain [20, 21]. As with manual therapy, research into DN has not only focused on clinical trials and systematic reviews, but looked towards basic science to develop a greater understanding of the underlying mechanisms of DN. A lot of current focus is on DN and its effect on inhibitory pain mechanisms and sensitization of the nervous system [22, 23, 24]. Similarly, some emerging pain science research is beginning to tie DN to potential influences on cortical maps, similar to manual therapy. O’Neill and colleagues recently showed that DN yield significant improvements in left-right judgement tasks as well as two-point discrimination – both tests often used to determine altered cortical maps in clinical practice [25]. Wand and colleagues, even though specifically focusing on acupuncture, showed that active patient attention to needle placement, part of sensory discrimination and integration, play a role in the mechanism of needling [26].
In clinical practice it is commonplace to have patients complete a body diagram, indicating where they hurt. It is argued that this allows patients to additionally express their pain experience and allow clinicians much needed additional information needed to develop a diagnosis. Body diagrams have enormous variability [27] and it has often been shown to poorly correlate to levels of pain and disability, compared to other standardized measures [28, 29]. Even though a lot is unknown about body diagrams completed by patients, a recent study on fibromyalgia showed a potential link to patient body diagrams and altered cortical body maps seen on advanced brain scans [30].
Given the emerging evidence that tactile treatment such as manual therapy or more discrete needle placement in DN may positively influence cortical maps, could DN positively influence body diagrams of pain? This study aimed to determine if DN of spinal pain (low back and neck) would result in positive changes of body diagrams and if such changes correlate to improvements in pain and patient experience.
Methods
Study Design
Two private practices in Iowa and Virginia gave permission for this study and research review board approval was obtained from Southwest Baptists University, Bolivar MO. Given the exploratory aim of the study a case series design was chosen with pre- and post-intervention measures.
Participants
A convenience sample of patients, meeting the inclusion criteria, presenting with low back or neck pain in physical therapy was asked to participate in the study. Participation was entirely voluntary and signed informed consent was obtained. The goal was to capture data over a 4-month period. In line with previous DN studies, during the physical therapy physical examination if palpation tenderness over the affected area was found, indicative of an active trigger point (taught band, twitch response and referred pain), [31, 32] patients were asked to participate in the study [20, 33]. Per DN study protocols, patients were excluded if they were under the age of 18; not able to read/write the English language; have undergone recent surgery in the DN area; have a fear/phobia of needles; not willing to give consent for DN; lack sensation in the proposed area of DN; bleeding disorders; immune compromised; pregnant; have seizure disorders; allergic to metals or have implants in the affected area [20, 33, 34].
Therapist and Intervention
The therapists delivering the DN have undergone post- graduate training in DN; uses DN on a regular clinical basis and practices DN in accordance with current state laws. The clinics in which the study was conducted provided consent for the delivery of DN and collecting data for the study. No personal identifiable information was collected. Patients were assigned a code as they enter the study, as patient 1; patient 2, etc. The DN was applied to the muscles containing active trigger points over the affected area per clinical discretion of the physical therapist in line with current treatment principles of DN for musculoskeletal pain.
Outcome Measures
Upon consent, patients completed a demographics questionnaire with no identifiable information being captured or shared with the research team, other than the practicing physical therapist. Five formal tests were conducted before and immediately after the intervention.
Self-reported pain rating – Numeric pain rating scale (NPRS): Spinal pain was measured with the use of a NPRS, as has been used in various studies for musculoskeletal pain [35, 36, 37, 38]. The minimal clinical important difference (MCID) for the NPRS for acute/sub-acute low back pain is reported to be 2.0 [39] and for chronic low back pain is 1.7 [40]. For neck and upper extremity pain, an MCID of 3 has been advised [41].
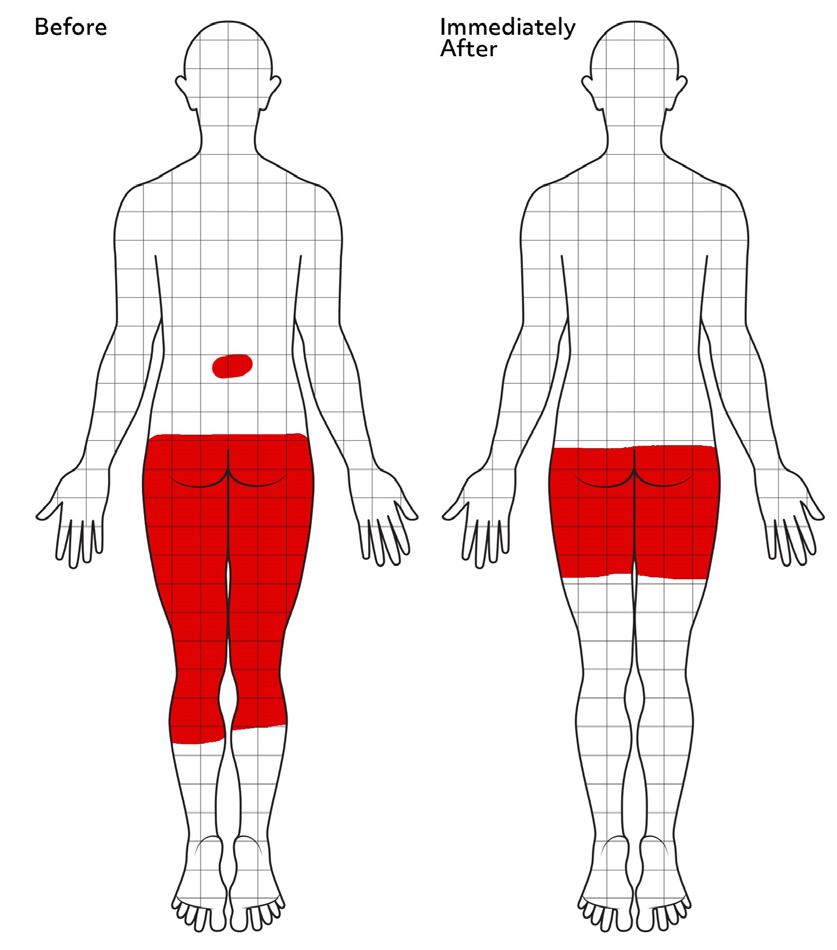
Body chart (grid allocation): Prior to and immediately after DN, patients were asked to “color in the area they experience pain.” Recent pain science research has pointed to body chart drawings as a potential indication of the integrity of the S1 region of the brain [19, 42]. Body charts were quantified with an overlay grid system to produce a count of blocks covered during the drawings before and after DN [19]. This method has been used in previous studies to quantify increase and/ or decrease in body pain drawings for musculoskeletal pain (Figure 1) [19, 43, 44, 45].
Global rate of change scale: The GROC scale is global rating of improvement and satisfaction over the course of treatment [46]. It does not measure a specific dimension such as pain or function but allows the patient to decide what they consider important. The GROC is a commonly used outcomes tool in clinical research, especially as it relates to musculoskeletal care [47, 48]. The most common formats of the GROC is typically a 7, 11, or 15 point scale on a number line with 0 in the middle and moving out one integer in the positive and negative numerical direction. The end anchors also contain the negative and positive words of “very much worse” and “very much improved” or ”completely better” with “no change” being in the middle at the zero [49]. For purposes of this study the recommended 15 -point scale were used (-7 = very much worse, 0 = unchanged, 5 = completely recovered). [49] The MCID for the GROC for musculoskeletal pain has been reported as a positive shift of 3 points or more (+3) [50].
All measures were conducted by an independent, non- treating therapists to ensure results are blinded for the therapist providing the treatment. Upon completion of the immediate post-intervention measures, patients continued with their regular plan of care per discretion of the physical therapist.
Analysis
All 43 observations in the original dataset were used calculating descriptive statistics such as sample means, standard deviations, and within-group correlations calculated and reported below. No observations were permanently discarded or modified in any analysis. Paired sample t-tests were used to evaluate any differences between GROC, NPRS, and Body Maps before and after treatment for observations with full information regarding pre- and post- treatment measurements.
Results
Patients
Forty-three patients participated in this study, with a mean age of 47.09 years (standard deviation [SD] = 12.81). Thirty-three of the patients (76.74%) identified as female. Table 1 showcases the patient demographic broken out as either low back pain (n = 19) or neck pain (n = 24).
| Low back pain | Patients (n = 19) |
|---|---|
| Mean age (years) | 47.95 (11.67) |
| Female (%) | 15 (78.95) |
| Mean disability (Oswestry Disability Index) | 15.84 (8.32) |
| Duration of pain (months) | 32.68 (81.98) |
| Mean self-reported pain rating (NPRS) | 4.97 (1.93) |
| Mean body diagram-colored blocks | 44.26 |
| Neck pain | Patients (n = 24) |
| Mean age (years) (SD) = 46.42 (SD=13.85) | 46.42 (13.85) |
| Female(%) | 18 (75) |
| Mean disability (Neck Disability Index) | 13.46 (6.07) |
| Mean duration of pain (months) | 43.17 (55.74) |
| Mean self-reported pain rating (NPRS) | 4.69 (2.07) |
| Mean body-diagram-colored blocks | 25 (26.11) |
Table 1: Patient demographics broken out between low back and neck pain.
Self-Reported Pain
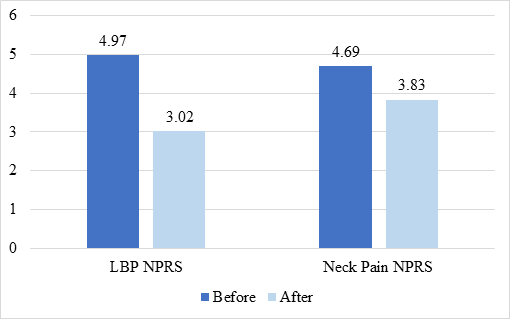
Prior to DN, the combined sample of patients with spinal pain reported a mean self-reported pain rating of 4.81. Immediately following DN the sample’s mean pain rating improved significantly by 1.34 points (p < 0.001; t(42)=4.7, (95%CI= 0.8 - 1.9) to 3.48. Region-specific measures (Figure 2) show DN to significantly reduce low back pain by 1.94 points (95%CI= 1.1, 2.8) t(18)=4.8 (p < 0.001) and neck pain by 0.86 points (SD=1.8), 95%CI = .1-1.6, t(23)=2.3, (p = 0.031).
Patient Satisfaction
The mean GROC score after DN was 2.53 (SD=2.86). Twenty-five patients (58.1%) met or exceeded the MCID of +3 points following DN. The mean GROC for low back pain was 3.21 and for neck pain 2.0 after DN. A positive GROC score had moderate correlation (r = 0.62) with a positive shift in self-reported pain scores after DN.
Body Diagrams
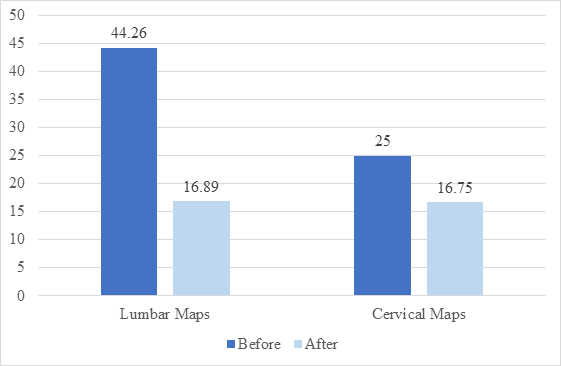
Overall, the whole patient sample’s body diagram decreased in size by 50.16% following DN (95%CI = 10.8, 22.6; t(42)=5.67, p < 0.001). When broken down between neck and low back pain, low back maps shrunk by 61.84% (95%CI= 16.1 - 38.6), t(18)=5.1, p < 0.001), whereas neck maps decreased by 33% (95%CI= 4.3 - 12.2, t(23)=4.4, p < .001) (Figure 3).
Correlations
Various correlations were run on the available data from the study. Three significant correlations (Spearman Rho) were found: Higher intensities of pain were moderately correlated with larger body map drawings (rs = 0.461 (p = 0.002).
A weak correlation was found between the reduction of pain after DN and reduction in body map drawings (rs = 0.305 (p = 0.047).
Higher scores on the GROC were found to have a moderate correlation with reduction in pain after DN (rs = 0.614 (p < 0.001).
Discussion
The results of this study show that DN in a cohort of patients attending physical therapy for back or neck pain reduce the size of body pain diagrams. Although only a weak correlation, the decrease in body map diagrams seem to correlate with a reduction in pain after DN. More robust changes are found for low back pain compared to neck pain. This is the first study to specifically demonstrate a change in body pain diagrams after DN.
Although this is the first study specific to body map drawings and DN, the results concur with a growing body of evidence supporting the notion that DN may in fact affect cortical maps of the body, which play a pivotal role in pain. O’Neill et. al.’s study showed that DN positively influenced two-point discrimination, [25] a clinical test well-described and used in measuring tactile perception and acuity [51, 52]. It is hypothesized that two-point discrimination changes are associated with cortical map changes [52, 53]. Similarly, recent work on patients with fibromyalgia pointed to a link between altered body pain diagrams and altered maps in the brain [30]. For the longest time, altered cortical maps in clinical practice was associated with rare, very complex pain conditions such as phantom limb pain and complex regional pain syndrome [12, 14, 54] neither conditions typically treated with DN. Emerging research, however is showing that altered cortical maps play a potentially larger role in commonly seen pain conditions including back pain, radiculopathy, knee osteoarthritis, and more – all conditions commonly treated in physical therapy with DN [13, 14, 19]. All of these results, and the growing body of evidence, pushes the agenda that clinicians should become more and more aware of the interplay between their treatments and its potential effect on cortical body maps as a means to influence a positive outcomes. Long gone are the days where these types of anomalies are only to be thought of in rare, complex clinical cases and may be more main stream. Additionally, authors, researchers, and clinicians in the field of DN should add cortical remapping as a potential underlying mechanism of DN’s positive effect on spinal pain.
The study showed that DN yields immediate positive shifts in pain, especially low back pain. A striking difference in this study, as it pertains to pain and body pain diagrams, is the difference between patients with low back pain and those with neck pain. In this study, DN as an intervention to alter body pain diagrams and self-reported pain, was more effective for patients presenting with low back pain compared to neck pain. Overall, the pain distribution, as seen by number of grid boxes colored by patients, prior to intervention was higher in those presenting with low back pain compared to neck pain. Similarly, starting low back pain was rated higher than starting neck pain, with the results also pointing out that pain intensity had some correlation to body area represented in the pain drawings. This result concurs with previous studies correlating pain intensity with the extent of a body pain diagram [55]. This would imply that the current study adds to the growing body of evidence that higher pain intensities are associated with larger body pain diagrams. Conversely, it is thus argued that smaller body pain diagrams are associated with lower pain intensity. Again, the results of this study strengthen that argument since reducing body pain drawings with DN in this study showed some positive correlation to smaller body pain drawings after intervention. In regards to neck and low back pain, in terms of brain maps, it is also important to acknowledge that two-point discrimination norms are different between the neck and the low back, which may also potentially explain the difference in body pain drawing results after DN [45, 52].
The study contains various limitations. Even though it’s not uncommon to use case-series designs in exploratory studies, the case series design is limited since there’s no control group to compare the results to. Second, the study did not delineate acute, sub-acute or chronic pain, which is likely a confounding variable and should be considered in future studies. It is suggested that cortical mapping issues are more prevalent in chronic pain and future studies may want to focus on that sub-group of neck and low back pain. A significant shortcoming of this study was not to add additional sensory tests such as two-point discrimination or even psychosocial measures such as pain catastrophizing, which has been studied in this line of research to further aid in connecting the body of research here.
References
-
Sturmberg JP (2019) Evidence-based medicine-Not a panacea for the problems of a complex adaptive world. J Eval Clin Pract 25(5): 706-716.
-
Bouffard M, Reid G (2012) The good, the bad, and the ugly of evidence-based practice. Adapt Phys Activ Q 29(1): 1-24.
-
Rubinstein SM, Terwee CB, Assendelft WJJ, Boer MRD, Tulder MWV (2012) Spinal manipulative therapy for acute low-back pain. The Cochrane database of systematic reviews 38(3): E158-177.
-
Flynn T, Fritz F, Whitman J, Wainner R, Magel J, et al. (2002) A clinical prediction rule for classifying patients with low back pain who demonstrate short-term improvement with spinal manipulation. 27(24): 2835- 2843.
-
Childs JD, Fritz JM, Flynn TM, Irrgang JJ, Johnson KK, et al. (2004) A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation. Ann Intern Med 141(12): 920-928.
-
Twomey LT (1992) A rationale for the treatment of back pain and joint pain by manual therapy. Phys Ther 72(12): 885-892.
-
Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ (2009) The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Manual therapy 14(5): 531-538.
-
Bialosky JE, Beneciuk JM, Bishop MD, Coronado RA, Penza CW, et al. (2018) Unraveling the Mechanisms of Manual Therapy: Modeling an Approach. J Orthop Sports Phys Ther 48(1): 8-18.
-
Wand BM, Parkitny L, O’Connell NE, Luomajoki H, McAuley JH, et al. (2011) Cortical changes in chronic low back pain: current state of the art and implications for clinical practice. Manual therapy 16(1): 15-20.
-
Stavrinou ML, Penna SD, Pizzella V, Torquati K, Cianflone F, et al. (2007) Temporal dynamics of plastic changes in human primary somatosensory cortex after finger webbing. Cereb Cortex 17(9): 2134-2142.
-
Kregel J, Meeus M, Malfliet A, Dolphens M, Danneels L, et al. (2015) Structural and functional brain abnormalities in chronic low back pain: A systematic review. Seminars in arthritis and rheumatism 45(2): 229-237.
-
Maihofner C, Handwerker HO, Neundörfer B, Birklein F (2003) Patterns of cortical reorganization in complex regional pain syndrome. Neurology 61(12): 1707-15.
-
Moseley GL, (2008) I can’t find it! Distorted body image and tactile dysfunction in patients with chronic back pain. 140(1): 239-243.
-
Lotze M, Moseley GL (2007) Role of distorted body image in pain. Curr Rheumatol Rep 9(6): 488-496.
-
Lloyd D, Findlay G, Roberts N, Nurmikko T (2008) Differences in low back pain behavior are reflected in the cerebral response to tactile stimulation of the lower back. 33(12): 1372-1377.
-
Louw A, Farrell K, Landers M, Barclay M, Goodman E, et al. (2017) The Effect of Manual Therapy and Neuroplasticity Education on Chronic Low Back Pain: A Randomized Clinical Trial. Journal of Manual & Manipulative Therapy 25(5): 227-234.
-
Louw A, Kevin F, Lauren W, Justine U, Katherine M, et al. (2015) Immediate effects of sensory discrimination for chronic low back pain: a case series. New Zealand Journal of Physiotherapy 43(2): 58-63.
-
Louw A, Schmidt SG , Louw C, Puentedura EJ (2015) Moving without moving: immediate management following lumbar spine surgery using a graded motor imagery approach: a case report. Physiotherapy Theory and Practice 31(7): 509-517.
-
Wand BM, Keeves J, Bourgoin C, George PJ, Smith AJ, et al. (2013) Mislocalization of sensory information in people with chronic low back pain: a preliminary investigation. The Clinical journal of pain 29(8): 737-743.
-
Furlan AD, Tulder MV, Cherkin D, Tsukayama H, Lao L, et al. (2005) Acupuncture and dry-needling for low back pain: an updated systematic review within the framework of the cochrane collaboration. Spine 30(8): 944-963.
-
Hu HT, Gao H, Rui-Jie M, Xiao-Feng Z, Hong-Fang T, et al. (2018) Is dry needling effective for low back pain?: A systematic review and PRISMA-compliant meta-analysis. 97(26): e11225.
-
Tellez-Garcia M, de-la-Llave-Rincón AI, Salom-Moreno J, Palacios-Ceña M, Ortega-Santiago R, et al. (2015) Neuroscience education in addition to trigger point dry needling for the management of patients with mechanical chronic low back pain: A preliminary clinical trial. Journal of bodywork and movement therapies 19(3): 464-472.
-
Fernandez-de-Las-Penas C, Nijs J (2019) Trigger point dry needling for the treatment of myofascial pain syndrome: current perspectives within a pain neuroscience paradigm. J Pain Res (12): 1899-1911.
-
Han JS (2003) Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci 26(1): 17-22.
-
O’Neill M, Louw A, Podalak J, Maiers N, Cox T, et al. (2021) A Case-Series of Dry Needling as an Immediate Sensory Integration Intervention. J Man Manip Ther 30(3): 165- 171.
-
Wand BM, Abbaszadeh S, Smith AJ, Catley MJ, Moseley GL (2013) Acupuncture applied as a sensory discrimination training tool decreases movement-related pain in patients with chronic low back pain more than acupuncture alone: a randomised cross-over experiment. British journal of sports medicine 47(17): 1085-1089.
-
George SZ, Bialosky JE, Wittmer VT, Robinson ME (2007) Sex differences in pain drawing area for individuals with chronic musculoskeletal pain. J Orthop Sports Phys Ther 37(3): 115-121.
-
Rhon DI, Lentz TA, George SZ (2017) Unique Contributions of Body Diagram Scores and Psychosocial Factors to Pain Intensity and Disability in Patients With Musculoskeletal Pain. J Orthop Sports Phys Ther 47(2): 88-96.
-
Rhon DI, Lentz TA, George SZ (2020) Utility of catastrophizing, body symptom diagram score and history of opioid use to predict future health care utilization after a primary care visit for musculoskeletal pain. Fam Pract 37(1): 81-90.
-
Ellingsen DM, Beissner F, Alsady TM, Lazaridou A, Paschali M, et al. (2021) A picture is worth a thousand words: linking fibromyalgia pain widespreadness from digital pain drawings with pain catastrophizing and brain cross-network connectivity. Pain 162(5): 1352- 1363.
-
Fernandez-de-Las-Penas C, Alonso-Blanco C, Cuadrado ML, Gerwin RD, Pareja JA (2006) Myofascial trigger points and their relationship to headache clinical parameters in chronic tension-type headache. Headache 46(8): 1264-1272.
-
Fernandez-de-Las-Penas C, Alonso-Blanco C, Miangolarra JC (2006) Myofascial trigger points in subjects presenting with mechanical neck pain: A blinded, controlled study. Man Ther 12(1): 29-33.
-
Téllez-García M, de-la-Llave-Rincón AI, Salom-Moreno J, Palacios-Ceña M, Ortega-Santiago R, et al. (2014) Neuroscience education in addition to trigger point dry needling for the management of patients with mechanical chronic low back pain: A preliminary clinical trial. J Bodyw Mov Ther 19(3): 464-472.
-
Hosseini L, Shariat A, Ghaffari MS, Honarpishe R, Cleland JA (2018) The effect of exercise therapy, dry needling, and nonfunctional electrical stimulation on radicular pain: a case report. J Exerc Rehabil 14(5): 864-869.
-
Moseley GL (2003) Joining forces - combining cognition- targeted motor control training with group or individual pain physiology education: a successful treatment for chronic low back pain. J Man Manip Therap 11(2): 88-94.
-
Moseley L (2002) Combined physiotherapy and education is efficacious for chronic low back pain. Aust J Physiother 48(4): 297-302.
-
Moseley GL (2005) Widespread brain activity during an abdominal task markedly reduced after pain physiology education: fMRI evaluation of a single patient with chronic low back pain. Aust J Physiother 51(1): 49-52.
-
Cleland JA, Childs JD, Whitman JM (2008) Psychometric properties of the Neck Disability Index and Numeric Pain Rating Scale in patients with mechanical neck pain. Arch Phys Med Rehabil 89(1): 69-74.
-
Childs JD, Piva SR, Fritz JM (2005) Responsiveness of the numeric pain rating scale in patients with low back pain. Spine 30(11): 1331-1334.
-
Farrar JT, Young Jr JP, LaMoreaux L, Werth J, Poole MR (2001) Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain (2): 149-158.
-
Stratford PW, Spadoni G (2001) The reliability, consistency and clinical application of a numeric pain rating scale. Physiotherapy Canada 53(2): 88-91.
-
Matthews M, Rathleff MS, Vicenzino B, Boudreau SA (2018) Capturing patient-reported area of knee pain: a concurrent validity study using digital technology in patients with patellofemoral pain. Peer J (6): e4406.
-
Lacey RJ, Lewis M, Jordan K, Jinks C, Sim J (2005) Interrater reliability of scoring of pain drawings in a self- report health survey. Spine 30(16): e455-458.
-
Sanders NW, Mann NH 3rd, Spengler DM (2006) Pain drawing scoring is not improved by inclusion of patient- reported pain sensation. Spine 31(23): 2735-2741.
-
Gerhardt A, Eich W, Janke S, Leisner S, Rolf-Detlef T, et al. (2016) Chronic Widespread Back Pain is Distinct From Chronic Local Back Pain: Evidence From Quantitative Sensory Testing, Pain Drawings, and Psychometrics. Clin J Pain 32(7): 568-579.
-
Dworkin RH, Turk DC, FarrarJT, Haythornthwaite JA, Jensen MP, et al. (2005) Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 113(1-2): 9-19.
-
Pengel LH, Refshauge KM, Maher CG, Nicholas MK, Herbert RD, et al. (2007) Physiotherapist-Directed Exercise, Advice, or Both for Subacute Low Back PainA Randomized Trial. Annals of Internal Medicine 146(11): 787-796.
-
Hancock MJ, Maher CG, Latimer J, McLachlan AJ, Cooper CW, et al. (2007) Assessment of diclofenac or spinal manipulative therapy, or both, in addition to recommended first-line treatment for acute low back pain: a randomised controlled trial. The Lancet. 370(9599): 1638-1643.
-
Kamper SJ, Maher CG, Mackay G (2009) Global rating of change scales: a review of strengths and weaknesses and considerations for design. Journal of Manual & Manipulative Therap 17(3): 163-170.
-
Puentedura EJ, Cleland JA, Landers MR, Mintken PE, Louw A, et al. (2012) Development of a clinical prediction rule to identify patients with neck pain likely to benefit from thrust joint manipulation to the cervical spine. The Journal of orthopaedic and sports physical therapy 42(7): 577-592.
-
Shooter D (2005) Use of two-point discrimination as a nerve repair assessment tool: preliminary report. ANZ J Surg 75(10): 866-868.
-
Catley MJ, O’Connell NE, Berryman CB, Ayhan FF, Moseley GL (2014) Is Tactile Acuity Altered in People With Chronic Pain? A Systematic Review and Meta-analysis. The Journal of Pain 15(10): 985-1000.
-
Akatsuka K, Noguchi Y, Harada T, Sadato N, Kakigi R (2008) Neural codes for somatosensory two-point discrimination in inferior parietal lobule: an fMRI study. Neuroimage 40(2): 852-858.
-
Flor H, Nikolajsen L, Jensen TS (2006) Phantom limb pain: a case of maladaptive CNS plasticity? Nature reviews. Neuroscience 7(11): 873-881.
-
Barbero M, Moresi F, Leoni D, Gatti R, Egloff M, et al. (2015) Test-retest reliability of pain extent and pain location using a novel method for pain drawing analysis. European journal of pain 19(8): 1129-1138.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial