The Best Arm Position for Therapeutic Ultrasound Application in Lateral Elbow Tendinopathy Patients
Objectives: To determine which is the best arm position for Therapeutic Ultrasound (TUS) application in Lateral Elbow Tendinopathy (LET) patients. Patients and Methods: A randomized clinical trial was carried out with 33 patients who had Let in a research center. They were randomly allocated to three groups. Group A (n=11) was treated with were treated with an exercise program and application of TUS with the wrist in full flexion. An exercise program and application of TUS with the wrist in mid position between flexion and extension was given to group B (n=11). Group C (n=11) received an exercise program and application of TUS with the wrist in full extension. All patients received three treatments per week for six weeks. The pain was evaluated using a visual analogue scale and function using a visual analogue scale and pain-free grip strength at the end of the four-week course of treatment (week 4) and one month (week 8) after the end of treatment. Results: The application of TUS with the wrist in full extension produced the largest effect in the reduction of pain and in the improvement of function at the end of the treatment (P<0.05) and at any of the follow-up time points (P<0.05). Conclusion: The application of TUS with the wrist in full extension was the most effective treatment. Future well-designed studies are needed to confirm the results of the present trial.
Introduction
Lateral elbow tendinopathy (LET) is the most common tendinopathy in the elbow area. Although the diagnosis of LET is simple and quick, the gold standard approach for the management of LET does not exist. A conservative treatment is usually advocated by the majority of physicians. Therefore, physiotherapy is provided. A lot of physical therapy approaches have been provided for the management of LET such as manual therapy, soft tissue manipulation, external support, physical agents and heavy-slow resistance exercise. Such a plethora of approaches suggests that the gold standard treatment strategy is unknown, and further research is needed to find the most effective treatment approach in LET patients.
The most effective physical therapy approach for LET is an exercise programme, supervised or in clinical placement [1, 2]. The LET exercise programme should be based on a progressive loading of the whole upper limb [3, 4]. An exercise program is usually combined with a plethora of physiotherapy techniques. One of the provided physiotherapy treatments is therapeutic ultrasound (TUS).
TUS utilizes a hand-held device to make and transport sound waves to the injured site [5]. It provides thermal and non-thermal effects to soft tissues in the body [5]. TUS is a dose-response modality and its effectiveness is based on parameters [6]. The use of TUS in treating LET has been widely researched and used in the clinic. TUS parameters for the management of LET have already been recommended [6]. However, no studies exist to determine which is the best arm position for TUS application in LET patients. Therefore, the aim of the present trial is to find out which arm position is the best for TUS application in LET patients.
Methods
A randomized controlled, mono-centre trial was conducted in the Cyprus Musculoskeletal and Sports Trauma Research Centre (CYMUSTREC) over 26 months to assess the best arm position for TUS application in LET patients. A parallel group design was used because crossover designs are limited in situations where patients are cured by the intervention and do not have the opportunity to receive the other treatments after crossover [7]. Three investigators were involved in the study: (1) a physiotherapist, the primary investigator, (DS) who evaluated the patients to confirm the LET diagnosis and allocated patients to groups, (2) a physiotherapist (AC) who performed all baseline and follow-up assessments, and gained informed consent and (3) a physiotherapist, (AZC), who administered the treatments. All assessments were conducted by AC who was blind to the patient’s therapy group. AC interviewed each patient to ascertain baseline demographic and clinical characteristics, including patient name, sex, age, duration of symptoms, previous treatment, occupation, the affected, arm and dominant arm.
Patients over 18 years old who were experiencing lateral elbow pain were examined and evaluated in the CYMUSTREC in Nicosia between September 2016 and July 2018. All patients lived in Cyprus, were native speakers of Greek, and were either self-referred or referred by their physician or physiotherapist.
Patients were included in the study if, at the time of presentation, they had been evaluated as having clinically diagnosed LET for at least 3 months. Patients were included in the trial if they reported (a) pain on the facet of the lateral epicondyle when palpated, (b) less pain during resistance supination with the elbow in 90∘ of flexion rather than in full extension and (c) pain in at least two of the following four tests [8]
- Tomsen test (resisted wrist extension)
- Resisted middle finger test
- Mill’s test (full passive flexion of the wrist)
- Handgrip dynamometer test.
Patients were excluded from the study if they had one or more of the following conditions: (a) dysfunction in the shoulder, neck (radiculopathy) and/or thoracic region; (b) local or generalized arthritis; (c) neurological deficit; (d) radial nerve entrapment; (e) limitations in arm functions; (f) the affected elbow had been operated on and (g) had received any conservative treatment for the management of LET in the 4 weeks before entering the study [9, 10, 11].
All patients received a written explanation of the trial prior to entry into the study. All patients gave signed informed consent to participate in the study. The study was approved by the Topical Research Ethics Committee and access to patients was authorised by the director (DS) of the CYMUSTREC.
The patients were randomly allocated to three groups by drawing lots. Patients in Group A were treated with exercise program and application of TUS with the wrist in full flexion, patients in Group B were treated with exercise program and application of TUS with the wrist in mid position between flexion and extension and patients in Group C were received an exercise program and application of TUS with the wrist in full extension.
All patients were instructed to use their arms during the course of the study but to avoid activities that irritated the elbow such as grasping, lifting, knitting, handwriting, driving a car and using a screwdriver. They were also told to refrain from taking anti-inflammatory drugs throughout the course of the study. Patient compliance with this request was monitored using a treatment diary.
Communication and interaction (verbal and non-verbal) between the therapist and patient were kept to a minimum, and behaviors sometimes used by therapists to facilitate positive treatment outcomes were purposefully avoided. For example, patients were given no indication of the potentially beneficial effects of the treatments or any feedback on their performance in the pre-application and post-application measurements [11].
The patients in three groups followed a supervised exercise programme as reported in previous case studies [12, 13] and trials [7, 9, 14, 15, 16, 17, 18]. The elbow was on the bed extended, the forearm pronated, the wrist in extension (and the hand hanging at the edge of the table. From this position, subjects flexed their wrists and then returned to the extension (starting position). In the starting position, subjects carried out an isometric contraction of wrist extensors. When the isometric contraction finished the subjects carried out the eccentric - concentric contraction and so on. The exercise involved isolated wrist extension and flexion paced to an external audio/visual cue on the patients’ smartphone (PR Metronome; http://eumlab.com/pro-metronome/). Subjects were to track the movement and listen to the sound of the metronome with their eyes. Each beat was ten seconds apart, so that the pace of the metronome was settled to 6 beats per minute. This allowed a ten second eccentric, concentric and isometric phase.
All groups performed three sets of 15 repetitions of slow progressive exercises of the wrist extensors at each treatment, with 1-minute rest interval between each set. Subjects were informed to continue with the exercise even if they complained of mild pain. However, subjects were informed to stop the exercise if the pain became disabling. The disabling and mild pain were monitored asking the subjects to rate the pain on VAS before and after treatment period. The definition of mild pain was below 4 on VAS whereas the definition of disabling pain was above 8 on VAS [7, 9]. When subjects were able to carry out the exercise programme without experiencing any discomfort or pain, free weights were used to increase the load.
The treatment groups performed static stretching exercises of the wrist extensors. Three times before and three times after the exercises six times totally were repeated the static stretching exercises at each treatment session, with a 30 second rest interval between each repetition. The other hand helped to be performed the static stretching exercises of the wrist extensors. The patient’s elbow was placed in an extended position, the forearm in a pronated position, and the wrist in ulnar deviation and flexion according to the patient’s tolerance. 30 - 45 seconds was holding this position each time and then releasing.
Furthermore, the scapular and rotator cuff muscles were strengthened. The strengthening exercises were included (i) shoulder lateral rotation and medial with the elbow in 90° and 0° of abduction; (ii) shoulder abduction to 900 with flexed elbow: (iii) scaption and (iv) diagonal pattern from flexion to extension. Upper trapezius, rhomboids, serratus anterior and levator scapulae were also strengthened. Each exercise was carried out twice at each treatment with 12 repetitions in each set and 1 min rest interval between each set. Subjects were informed to continue with the exercise even if they complained of mild pain. However, subjects were informed to stop the exercise if the pain became disabling. When subjects were able to carry out the strengthening exercises without experiencing any discomfort or pain, the load was increased using therabands or free weights.
Finally, the supinator was strengthened. Strengthening exercises of the supinator were carried out with the elbow extended on the table, the forearm pronated, the wrist in mid - position and the hand hanging over the edge of the table. From this position, the patient supinated their arm slowly while counting to 15 using chronometer, then return to the starting position (pronation).
The above reported exercise programme was followed 3 times per week for 6 weeks and was individualized on the basis of the patient’s description of pain experienced during the process.
The TUS parameters were as follows [6]: Frequency: 3 MHz Mode: pulsed, pulsed ratio 1:1 Intensity: 0.5-0/8 W/cm Duration of treatment: 2 minutes Movement or not of the soundhead (transducer): No stationary technique Coupling medium: ultrasound gel Treatment intervals: every other day Effective radiated area: The area of pain, usually the insertion of extensor carpi radialis brevis using small transducer-approximately 1 cm [6], moving the soundhead slowly in circular or in longitudinal pattern.
All patients received scripted instructions which stated that they were not to feel anything like warmth or any other sensation such as rubbing, tingling, or discomfort during the application of the TUS energy. During 6 wk of treatment, the patients received 18 sessions of TUS treatment, three times per week (Monday, Wednesday, and Friday). The application of TUS was performed before the exercise program.
Pain, function and drop-out rate were measured in the present study. Each patient was evaluated at the baseline (week 0), at the end of treatment (week 4) and at 1 month (week 8) after the end of treatment.
Pain was measured on a visual analogue scale (VAS), where 0 (cm) was “least pain imaginable” and 10 (cm) was “worst pain imaginable”. The pain VAS was used to measure the patient’s worst level of pain over the previous 24 h before each evaluation, and this approach has been shown to be valid and sensitive of the VAS [19].
Function was measured using a VAS, in which 0 (cm) was taken as “no function” and 10 (cm) as “full function”. Patients were instructed to report their overall level of elbow function over the previous 24 h before each evaluation, and this approach has been shown to be valid and sensitive of the VAS [19].
In addition, function was measured by pain-free grip strength. Pain-free grip strength is defined as the amount of force each patient is able to generate with an isometric gripping action before eliciting pain [11]. Force was measured in pounds with a Jamar hand dynamometer that had adjustable handles to accommodate different hand sizes. The arm was placed in a standardised position of elbow extension, forearm pronation and internal rotation of the upper limb such that the palmar aspect of the hand faced posteriorly with the upper limb placed by the patient’s side. Patients were then instructed to squeeze the dynamometer handles until they first experienced pain and then to release their grip [11]. The attained grip force was subsequently recorded, and the reading was not visible to the patient. Three measures of pain-free grip strength were recorded with a 30 seconds rest interval between each measurement, and the mean value of these repetitions was calculated.
A drop-out rate was also used as an indicator of treatment outcome. Reasons for patient drop out were categorized as follows: (1) a withdraw without reason; (2) not returned for follow-up and (3) request for an alternative treatment.
The change from baseline was calculated for each follow- up for each outcome measure. Differences in this change pain on the VAS, change in function on the VAS and change in pain-free grip strength was calculated between the groups and was determined using a one-way analysis of variance (one-way ANOVA). Paired t - test was used to measure the improvement in all groups when compared with the pretreatment baseline. Bonferroni post-hoc comparisons were conducted when the results from the one-way ANOVA were significant to determine how the three groups differed. A 5% level of probability was adopted as the level for statistical significance. SPSS version 20 statistical software was used for the statistical analysis.
Results
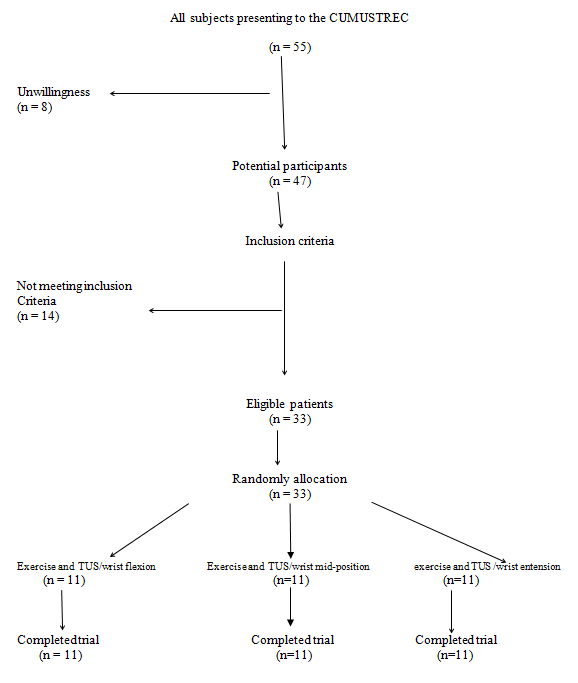
Fifty five patients eligible for inclusion visited the clinic within the trial period. Eight were unwilling to participate in the study and fourteen did not meet the inclusion criteria described above. The other 33 patients were allocated into one of the three possible groups: (1) exercise program and application of TUS with the wrist in full flexion (n=11; 4 male, 7 female; mean age = 41.8 years +-SD=4.7 years), (2) exercise program and application of TUS with the wrist in mid position of flexion-extension (n=11; 3 male, 8 female; mean age=46.2 years +_SD=5.1 years) and (3) exercise program and application of TUS with the wrist in full extension (n=11; 6 male, 5 female; mean age=45.4 years +_SD=4.3 years). Patient flow through the trial is summarized in a CONSORT flow chart (Figure 1).
At baseline there were more females in the groups (7 in total). The mean age of patients was approximately 44 years and the duration of LET was approximately six months. LET was in the dominant arm in 90% of patients. There were no significant differences in mean age (P<0.0005, one-way ANOVA) or the mean duration of complaints (P<0.0005, one- way ANOVA) between the groups. Drug therapy had been tried by all patients. All patients were manual workers.
Baseline pain on VAS was 6.8 cm (95% confidence interval (CI)= 6.6 - 7.4) for the whole sample (n=33) (Table 1). There were no significant differences between the groups for baseline pain (P>0.05 one-way ANOVA, Table 1). At week 4 there was a decline in VAS of approximately 4 units in all groups when compared with the pretreatment baseline (P<0.0005, paired t - test,) (Table 2). There was a significant difference in the magnitude of reduction between the groups (P<0.0005 one-way ANOVA, Table 2), so post-hoc tests were performed. The magnitude of reduction was significantly larger for exercise program and application of TUS with the wrist in full extension than for exercise program and application of TUS with the wrist in mid position of flexion- extension (+1.2 VAS units) and exercise program and application of TUS with the wrist in full flexion (+1.5 VAS units, P<0.05, Bonferroni, Table 2). There was no significant difference between exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion (+0.3 VAS units, P>0.05, Bonferroni, Table 2). Similarly at week 8 there were comparable magnitudes of reduction with larger reduction for exercise program and application of TUS with the wrist in full extension than exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion (P<0.05, Bonferroni, Table 2). There was not a significant difference between exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion at week 8 (P>0.05, Bonferroni, Table 2).
| Wk 0 | Wk 4 | Wk 8 | |
|---|---|---|---|
| Pain | |||
| EX TUS FLEXION | 6.8 (6.4-7.2) | 3.8 (2.8-4.5) | 3.6 (2.3-3.3) |
| EX TUS EXTENSION | 7 (6.6-7.3) | 2.5 (2 -2.9) | 2.1 (1.5-2.4) |
| EX TUS MID POSITION | 6.8 (6.3-7.1) | 3.5 (2.8-3.8) | 3.4 (2.2-3.2) |
| Function | |||
| Ex Tus Flexion | 4 (3.3-4.3) | 6.8 (6.4-7.1) | 6.9 (6.7-7.4) |
| Ex Tus Extension | 3.8 (3.4-4.4) | 8.1 (7.5-8.3) | 8.5 (8.1-8.8) |
| Ex Tus Mid Position | 3.8 (3.5-4.3) | 7.2 (6.7-7.5) | 7.3 (6.8-7.6) |
| Pain-Free Strength (Lb) | |||
| Ex Tus Flexion | 26 (23.7-27.8) | 64 (60.8-68.6) | 65 (61.7-70.3) |
| Ex Tus Extension | 25.9 (24.1-27) | 72 (67.7-77.4) | 75 (71.2-79.8) |
| Ex Tus Mid Position | 26 (24.8-27.2) | 66 (61.2-69.4) | 66 (62.2-70.1) |
Table 1: Pain, function, and pain-free grip strength. EX = Exercise Program TUS = Therapeutic Ultrasound Ex Tus Flexion = exercis
Table 1: Pain, function, and pain-free grip strength. EX = Exercise Program TUS = Therapeutic Ultrasound Ex Tus Flexion = exercise program and application of TUS with the wrist in full flexion Ex Tus Extension = exercise program and application of TUS with the wrist in full extension Ex Tus Mid Position = exercise program and application of TUS with the wrist in mid position of flexion-extension
| Ex Tus Flexion | Ex Tus Extension | Ex Tus Mid Position | One-way ANOVA on change in VAS from baseline (P) | Ex Tus Flexion Vs Ex Tus Extension | Ex Tus Flexion Vs Ex Tus Mid Position | Ex Tus Extension Vs Ex Tus Mid Position | |
|---|---|---|---|---|---|---|---|
| Pain | |||||||
| Wk 4 | 3 (5.8-2.4) | 4.5 (6.8-2.4) | 3.3 (5.3-2.4) | <.0005 | +1.5a (0.8-1.9) | +0.3 (0.05-0.5) | 1.2a (0.9-1.6) |
| Wk 8 | 3.3 (6.2-2.1) | 4.9 (7.2-3.1) | 3.4 (5.5-2.1) | <.0005 | +1.6a (0.9-1.8) | +0.1 (0.2-0.6) | 1.5a ( 0.9-1.9) |
| Function | |||||||
| Wk 4 | +2.8 (1.8-3.4) | + 4.3 (3.4-5.5) | + 3.2 (2.4-3.8) | <.0005 | +1.5a (0.2-1.1) | +0.4 (0.1-0.7) | 1.1a (0.6-1.4) |
| Wk 8 | + 2.9 (2.3-3.8) | + 4.7 (3.6-5.9) | + 3.4 (2.7-4.1) | <.0005 | +1.8a (0.4-1.5) | +0.5 (0.3-0.8) | 1.3a (0.9-1.8) |
| Pain-Free Grip Strength | |||||||
| Wk 4 | + 38 (31.5- 46.5) | + 46,1 (38.4- 55.6) | +40 (27.5- 50.5) | <.0005 | +8.1a (6.5-9.8) | +2 (1.8-4.5) | 6.1a (5.2- 16.3) |
| Wk 8 | + 39 (33.5- 47.6) | + 49.1 (47.2- 56.6) | + 40 (36.3- 47.1) | <.0005 | +10.1a (6.5- 12.2) | +1 (0.6-2.1) | 9.1a (8.3- 12.8) |
Table 2: Change in pain, function, and pain-free grip strength. EX = Exercise Program TUS = Therapeutic Ultrasound Ex Tus Flexion
Table 2: Change in pain, function, and pain-free grip strength. EX = Exercise Program TUS = Therapeutic Ultrasound Ex Tus Flexion = exercise program and application of TUS with the wrist in full flexion Ex Tus Extension = exercise program and application of TUS with the wrist in full extension Ex Tus Mid Position = exercise program and application of TUS with the wrist in mid position of flexion-extension ANOVA = analysis of variance VAS = visual analog scale a The mean difference is significant at the .05 level. Values are means (95% confidence interval).
Baseline function on VAS was 4.4 cm (95% confidence interval (CI)=3.9 – 4.6) for the whole sample (n=33) (Table 1). There were no significant differences between the groups for baseline function (P>0.05 one-way ANOVA, Table 1). At week 4 there was a rise in VAS of approximately 3 units in all groups when compared with the pretreatment baseline (P<0.0005, paired t - test, Table 2). There was a significant difference in the magnitude of improvement between the groups (P<0.0005 one-way ANOVA, Table 2), so post-hoc tests were performed. The magnitude of improvement was significantly larger for exercise program and application of TUS with the wrist in full extension than for exercise program and application of TUS with the wrist in mid position of flexion-extension (+1.1 VAS units) and exercise program and application of TUS with the wrist in full flexion (+1.5 VAS units, P<0.05, Bonferroni, Table 2). There was no significant difference between exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion (+0.4 VAS units, P>0.05, Bonferroni, Table 2). Similarly at week 8 there were comparable magnitudes of improvement with larger improvements for the exercise program and application of TUS with the wrist in full extension than exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion (P<0.05, Bonferroni, Table 2). There was not a significant difference between exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion at week 8 (P>0.05, Bonferroni, Table 2).
Baseline pain-free grip strength was 27lb (95% confidence interval (CI)=26.1 – 27.8) for the whole sample (n=33) (Table 1). There were no significant differences between the groups for baseline pain-free grip strength (P>0.05 one-way ANOVA, Table 1). At week 4 there was a rise in pain-free grip strength of approximately 40 units in all groups when compared with the pretreatment baseline (P<0.0005, paired t - test, Table 2). There was a significant difference in the magnitude of improvement between the groups (P<0.0005 one-way ANOVA, Table 2), so post-hoc tests were performed. The magnitude of improvement was significantly larger for the exercise program and application of TUS with the wrist in full extension than for exercise program and application of TUS with the wrist in mid position of flexion-extension (+6.1 pain-free grip strength units) and exercise program and application of TUS with the wrist in full flexion (+8.1 pain-free grip strength units, P<0.05, Bonferroni, Table 2). There was no significant difference between exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion (+2 pain-free grip strength units, P>0.05, Bonferroni, Table 2). Similarly at week 8 there were comparable magnitudes of improvement with larger improvements for the exercise program and application of TUS with the wrist in full extension than exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion (P<0.05, Bonferroni, Table 2). There was not a significant difference between exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion at week 8 (P>0.05, Bonferroni, Table 2).
There were no drop-outs and all patients successfully completed the study.
Discussion
The results obtained from this randomized clinical trial are novel, as to date there have been no data to determine which is the best arm position for TUS application in LET patients. The application of TUS with the wrist in full extension produced the largest effect at the end of treatment and at the follow-up.
In this trial, the Stasinopoulos protocol was followed; under supervision, with isometric-eccentric-concentric exercises, strengthening of arm and shoulder, scapula and supinator, and static stretches [10, 20, 21]. Under supervision, protocols present better results faster [20, 21, 22]. Exercise, according to Κaranasios, et al. seems to be the best intervention amongst others, however, the certainty degree is low 1. Isometric- eccentric- concentric contraction was used [14] since the earlier the isometrics begin the better and more long-term the results are [23] and eccentrics present the most beneficial effect when combined with other interventions [24, 25].
The exercise was done by the sounds of a metronome. This affects neuroplasticity [12, 13, 26] the relationship between pain and changes in motor control. Tendon neuroplastic training; TNT, affects the central sensitization that occurs in chronic pain [27]. Shoulder and scapula and supinator muscle strengthening was done because muscle weakness affects the joint mechanism and stability [18, 28, 29, 30].
Ultrasound is a modality that physiotherapists use daily in their clinical practice [31]. There is strong evidence that ultrasound has positive effects on tendon healing, collagen synthesis and regeneration [32, 33]. This strong evidence is supported by animal studies.
Luo, et al. [34] demonstrated the TUS is helpful to relieve pain for LET patients, but no such benefit could be found for grip strength. However, the ultrasonic treatment group showed no advantage against other conservative treatments like rest and brace. This could be explained because TUS does not use as a sole treatment but as a supplement to the main treatment approach. Papadopoulos, et al. [35] support the use of TUS to treat painful LET. Positive overall effects of TUS in LET pain are apparent but need to be further clinically substantiated.
The effectiveness of ultrasound is based on its parameters. It is recommended pulsed TUS instead of continuous because pulsed TUS changes the cellular environment, increases membrane permeability, activates the degranulation of macrophages and mast cells, enhances proliferation of fibroblasts, and affects wound contraction and protein synthesis by influencing the acoustic current and cavitation [36, 37, 38]. The effects of pulsed TUS are attributed primarily to a cavitation and acoustic streaming and to a lesser extent to micro massage.
Although the optimal parameters of TUS for the management of LET have also been recommended no studies exist to determine which is the best arm position for TUS application in LET patients. This pilot trial found that the application of TUS with the wrist in full extension produced the largest effect at the end of treatment and at the follow-up.
This could be explained by combining the positive effects of stretching [39] with the effects of pulsed TUS.
However, this trial does have some shortcomings. First, the sample was small without performing power analysis. Second, no placebo (sham) or no treatment group was included in the present trial. The placebo (sham)/no treatment group is important when the absolute effectiveness of a treatment is determined. However, the absolute effectiveness of technique based interventions is difficult to investigate because a good and trustworthy placebo (sham)/no treatment control for exercise programmes appears to be difficult or impossible to devise, due in part to difficulties in defining the active element of these treatments. Absolute effectiveness also does not provide the therapists with information as to which is the most appropriate treatment for the management of a condition, in this case LET. Third, other activities treatments patients might be getting when not in the clinic were not monitored. Patients’ diaries suggested that patients were compliant to the study instructions, although patients may have given incorrect details to please the investigators. For example, it was possible that patients followed the treatment but took analgesic medications at the same time, and the improvement of symptoms may be due to those medications. Therefore, ways should be found to measure how other treatments such as analgesic medications contribute to the improvement of symptoms. Finally, the blinding of patients and therapists would be problematic in that case, if not impossible, because patients know if they are receiving the exercise programme treatment and therapists need to be aware of the treatment to administer it appropriately. In addition to the previously reported weaknesses, structural changes in the tendons related to the treatment intervention were not shown, and the intermediate and long-term effects (6 months or more after the end of treatment) of treatments were not investigated. Further research is needed to establish the possible mechanism of action of this treatment approach, and the cost-effectiveness of such treatment, because the reduced cost is an important issue for the recommendation of any given treatment.
In conclusion, an exercise program and application of TUS with the wrist in full extension, full flexion or in mid position of flexion-extension reduced pain and improved function at the end of the treatment and at the follow- up. The exercise program and application of TUS with the wrist in full extension produced the largest effect at the end of the treatment and at follow-up. This means that choosing among these treatments, the exercise program and application of TUS with the wrist in full extension should be the first treatment option for therapists when they manage LET. If for some reason it is not possible to administer the exercise program and application of TUS with the wrist in full extension, exercise program and application of TUS with the wrist in mid position of flexion-extension and exercise program and application of TUS with the wrist in full flexion may be suitable. Future well-designed studies are needed to confirm the results of the present trial.
References
-
Karanasios S, Korakakis V, Whiteley R, Vasilogeorgis L, Woodbridge S, et al. (2021) Exercise interventions in lateral elbow tendinopathy have better outcomes than passive interventions, but the effects are small: a systematic review and meta-analysis of 2123 subjects in 30 trials. Br J Sports Med (55): 477-485.
-
Samaras P, Karanasios S, Stasinopoulos D, Gioftsos G (2022) Greek physiotherapists’ contemporary knowledge and practice for lateral elbow tendinopathy: An online survey. Musculoskelet Sci Pract pp: 102502.
-
Dimitrios S (2016) Lateral elbow tendinopathy: Evidence of physiotherapy management. World J Orthop 7(8): 463-466.
-
Dimitrios S (2015) Exercise for tendinopathy. World J Methodol 5(2): 51-54.
-
Holmedal O, Olaussen M, Mdala I, Natvig B, Lindbaek M (2019) Predictors for outcome in acute lateral epicondylitis. BMC Musculoskelet Disord (20): 375.
-
Stasinopoulos D, Chatzidamianos T, Cheimonidou A (2013) Are there effective ultrasound parameters in the management of lateral elbow tendinopathy? A systematic review of the literature. International Journal of Physical Medicine & Rehabilitation (1): 117.
-
Manias P, Stasinopoulos D (2006) A controlled clinical pilot trial to study the effectiveness of ice as a supplement to the exercise programme for the management of lateral elbow tendinopathy. British Journal of Sports Medicine 40(1): 81-85.
-
Haker E (1993) Lateral epicondylalgia: diagnosis, treatment and evaluation. Crit Rev Phys Rehabil Med (5): 129-154.
-
Stasinopoulos D, Stasin opoulos I (2006) Comparison of effects of Cyriax physiotherapy, a supervised exercise programme and polarized polychromatic non-coherent light (Bioptron light) for the treatment of lateral epicondylitis. Clinical Rehabilitation 20(1): 12-23.
-
Stasinopoulos D, Stasinopoulos I, Manias P, Stasinopoulou K (2010) Comparison of effects of a home exercise programme and a supervised exercise programme for the management of lateral elbow tendinopathy, British Journal of Sports Medicine 44(8): 579-583.
-
Vicenzino B, Wright A, Collins C (1996) The initials effects of a cervical spine manipulative physiotherapy treatment on the pain and dysfunction of lateral epicondylalgia. Pain 68(1): 69-74.
-
Welsh P (2018) Tendon neuroplastic training for lateral elbow tendinopathy: 2 case reports. J Can Chiropr Assoc (62): 98-104.
-
Stasinopoulos D (2019) The Management of Lateral Elbow Tendinopathy using Tendon Neuroplastic Training: A Case Report. Acta Scientific. Orthopaedics 2(1): 2-5.
-
Stasinopoulos D, Stasinopoulos I (2017) Comparison of effects of eccentric training, eccentric - concentric training and eccentric – concentric training combined with isometric contraction in the treatment of Lateral Elbow Tendinopathy. Journal of hand therapy 30(1): 13- 19.
-
Bhatt JB, Glaser R, Chavez A, Yung E (2013) Middle and lower trapezius strengthening for the management of lateral epicondylalgia: a case report. Journal of Orthopaedic and Sports Physical Therapy 43(11): 841- 847.
-
Sharma M, Eapen C, Kamath J (2015) Effect of adding rotator cuff strengthening to therapeutic ultrasound and wrist extensor eccentric exercise for lateral epicondylalgia-A randomized clinical trial. International Journal of Health Sciences and Research 5(7): 250-257.
-
Stasinopoulos D (2017) Scapular and rotator cuff strengthening in patients with lateral elbow tendinopathy. Hong Kong Physiotherapy Journal (37): 25-26.
-
Demosthenous M, Stasinopoulos D, Lamnisos D (2017) Comparison the effectiveness of eccentric – concentric training of wrist extensors and eccentric – concentric training combined with supinator strengthening in healthy population J. Orthop. Res. Physiother (3): 036.
-
Stratford P, Levy D, Gauldie S, Levy K, Miseferi D (1987) Extensor carpi radialis tendonitis: a validation of selected outcome measures. Physiother Can 39(4): 250-255.
-
Stasinopoulos D (2022) A Progressive Loading Supervised Exercise Program and Manual Therapy for The Management of Lateral Elbow Tendinopathy: A Case Report. J Clin Case St Rev Rep 4(6): 1-4.
-
Stasinopoulos D, Stasinopoulou K, Johnson MI (2005): An exercise programme for the management of lateral elbow tendinopathy. Br J Sports Med 39(12): 944-947.
-
Stasinopoulos D, Manias P (2013) Comparing Two Exercise Programmes for the Management of Lateral Elbow Tendinopathy (Tennis Elbow/Lateral Epicondylitis)-A Controlled Clinical Trial. The Open Access J Science Tech.
-
Jin-Young P, Hong-Keun, Jin-Hyung, Eun-Sun M, Byung- Soo K, et al. (2010) Prospective evaluation of the effectiveness of a home-based program of isometric strengthening exercises: 12-month follow-up. Clin Orthop Surg 2(3): 173-178.
-
Raman J, MacDermid JC, Grewal R (2012) Effectiveness of different methods of resistance exercises in lateral epicondylosis-a systematic review. J Hand Ther 25(1): 5-26.
-
Chen Z, Baker NA (2021) Effectiveness of eccentric strengthening in the treatment of lateral elbow tendinopathy: A systematic review with meta-analysis. J Hand Ther 34(1): 18-28.
-
Rio E, Kidgell D, Purdam C, Gaida J, Moseley GL, et al. (2015) Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br J Sports Med 49(19): 1277-1283.
-
Plinsinga ML, Brink MS, Vicenzino B, Wilgen CPV (2015) Evidence of Nervous System Sensitization in Commonly Presenting and Persistent Painful Tendinopathies: A Systematic Review. J Orthop Sports Phys Ther 45(11): 864-875.
-
Bhatt JB, Glaser R, Chavez A, Yung E (2013) Middle and lower trapezius strengthening for the management of lateral epicondylalgia: a case report. J Orthop Sports Phys Ther 43(11): 841-847.
-
Sharma M, Eapen C, Kamath J (2015) Effect of adding rotator cuff strengthening to therapeutic ultrasound and wrist extensor eccentric exercise for lateral epicondylalgia—a randomized clinical trial. Int J Health Sci Res 5(7): 250-257
-
Stasinopoulos D (2017) Scapular and rotator cuff strengthening in patients with lateral elbow tendinopathy. Hong Kong Physiother J (37): 25-26.
-
Pope GD, Mockett SP, Wright JP (1995) A survey of electrotherapeutic modalities: ownership and use in the national health service in England. Physiotherapy 81(2): 82-91.
-
Demir H, Menku P, Kirnap M, Calis M, Ikizceli I (2004) Comparison of the effects of laser, ultrasound, and combined laser + ultrasound treatments in experimental tendon healing. Lasers Surg Med 35(1): 84-89.
-
Ng GY, Ng CO, See EK (2004) Comparison of therapeutic ultrasound and exercises for augmenting tendon healing in rats. Ultrasound Med Biol 30(11): 1539-1543.
-
Luo D, Liu B, Gao L, Fu S (2022) The effect of ultrasound therapy on lateral epicondylitis: A meta-analysis. Medicine Baltimore 101(8): e28822.
-
Papadopoulos ES, Mani R (2020) The Role of Ultrasound Therapy in the Management of Musculoskeletal Soft Tissue Pain Int J Low Extrem Wounds 19(4): 350-358.
-
Tan JC (2006) Practical manual of physical medicine and rehabilitation. In Tan JC (Ed.), 2nd (Edn.), Philadelphia: Mosby, pp: 858.
-
Klaiman MD, Shrader JA, Danoff JV, Hicks JE, Pesce WJ, et al. (1998) Phonophoresis versus ultrasound in the treatment of common musculoskeletal conditions. Med Sci Sports Exerc 30(9): 1349-55.
-
Fu SC, Shum WT, Hung LK, Wong MW, Qin L, et al. (2008) Low-intensity pulsed ultrasound on tendon healing: a study of the effect of treatment duration and treatment initiation. Am J Sports Med 36(9): 1742-1749
-
Stasinopoulos D (2017) Tendinopathy: The role of stretching. AMJ 10(1): 63-65.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial