Manual Therapy versus Extracorporeal Shockwave Therapy in Treatment of Frozen Shoulder: Randomized Clinical Trial
Background: Frozen shoulder is the painful condition known as adhesive capsulitis of the shoulder results in a progressive loss of glenohumeral mobility in passive. The study aimed to determine whether shock wave or manual therapy was more successful in treating frozen shoulder. Material and Methods: Patients admitted to the Department of orthopaedic physical therapy diagnosed with frozen shoulders according to the guidelines presented in a previous study 11 were deemed eligible for inclusion in the study. The age range for inclusion was 40–60 years old, with shoulder joint pain and a restricted range of motion lasting more than four weeks (the stiffness stage of the frozen shoulder). We used manual therapy versus shockwave therapy 3 sessions per week for 4 weeks. Results: There were significant differences at all measure outcomes superior for the shockwave therapy group at p ≤ 0.05. Conclusion: This study discovered that shockwave approach, as opposed to conventional manual therapy, was more beneficial in helping patients with frozen shoulder restore the joint function.
Abbreviations
PNF: Proprioceptive Neuromuscular Facilitation; ESWT: Extracorporeal Shockwave Therapy; CHL: Coracohumeral Ligament; CAR: Capsule Wall in the Axillary Recess.
Introduction
Frozen shoulder is the painful condition known as adhesive capsulitis of the shoulder results in a progressive loss of glenohumeral mobility in passive [1]. A more pronounced restriction in flexion and abduction is typical of the pattern of restriction, followed by a more modest restriction in lateral rotation. Studies show that 3-5% of people in general have frozen shoulder, which usually goes away within a year [2]. Idiopathic frozen shoulder has an unclear precise etiology and cause. Clinical classification identifies three phases: the painful phase, the stiffening phase, and the thawing phase [3].
Frozen shoulder is often referred to as idiopathic or primary frozen shoulder because the pathogenetic process is still unknown and new criteria for frozen shoulder, such as main and secondary, have been proposed. Using this latter word, we conducted our inquiry. Previous studies have suggested that the frozen shoulder has a self-limiting nature that fits into a three-phase model. However, because there is little evidence to support either the phased technique or the path to self-resolution, more recent works have questioned both [4].
The primary objectives of treatment for frozen shoulder are pain reduction and improved range of motion. A number of surgical (hydro dilatation, mobilisation under anaesthesia, arthroscopic or open release) and conservative (physiotherapy, non-steroidal anti-inflammatory drugs, NSAIDs, oral steroids, steroid injections, etc.) therapies are available, but no widely accepted, standardised therapeutic protocol has been developed as of yet. Typically, a number of conservative measures are tried first, and if non-operative treatment is not successful, surgery is undertaken [5].
Most frozen shoulder treatments don’t involve surgery. Surgical intervention, such as arthroscopic capsular release or capsular incision, is only undertaken when nonsurgical treatment is ineffective. There is a large range in the advantages and iatrogenic risks associated with surgical procedures. Manual therapy is being utilised increasingly often to speed up patient recovery even if there isn’t enough evidence to prove it works. Proprioceptive neuromuscular facilitation (PNF) is a crucial method in manual therapy for rehabilitation [6].
Despite the lack of conclusive evidence to support its efficacy, manual therapy is being used more and more to help patients recover more quickly. Rehabilitation therapists have been using this stretching technique, which has been shown to positively impact patients with frozen shoulders’ active and passive range of motion and can increase muscle suppleness, to help patients with soft tissue injuries regain their range of functional activities as well as improve their general strength, balance, and coordination of muscular strength [7].
Extracorporeal shockwave therapy (ESWT) is among the best physical therapy treatment techniques. In this non-invasive method, high-amplitude sound waves are administered to the required body component. Due to its ability to enhance fibroblast differentiation and proliferation into myofibroblasts, it is a valuable approach for encouraging tissue healing. It increases local blood flow, promotes soft tissue healing, helps the inflammatory-mediated healing process, and increases the flexibility of the collagen fibres in the injured area [8].
The ligament in front of the greater tuberosity of the humerus is where the coracohumeral ligament (CHL) stretches obliquely downward and outward from the lateral margin of the coracoid process. According to MRI, people with frozen shoulder had notably thicker CHLs, and this was highly associated with their limited range of motion in the shoulder joint. The pain associated with symptoms of frozen shoulder is also significantly worsened by thickening of the capsule wall in the axillary recess (CAR). Correcting the abnormal structural changes to the shoulder joint is therefore essential to treating frozen shoulder [9]. The study’s goal was to determine whether shock wave therapy or manual therapy was more successful in treating frozen shoulder.
Materials and Procedures
Design of Research
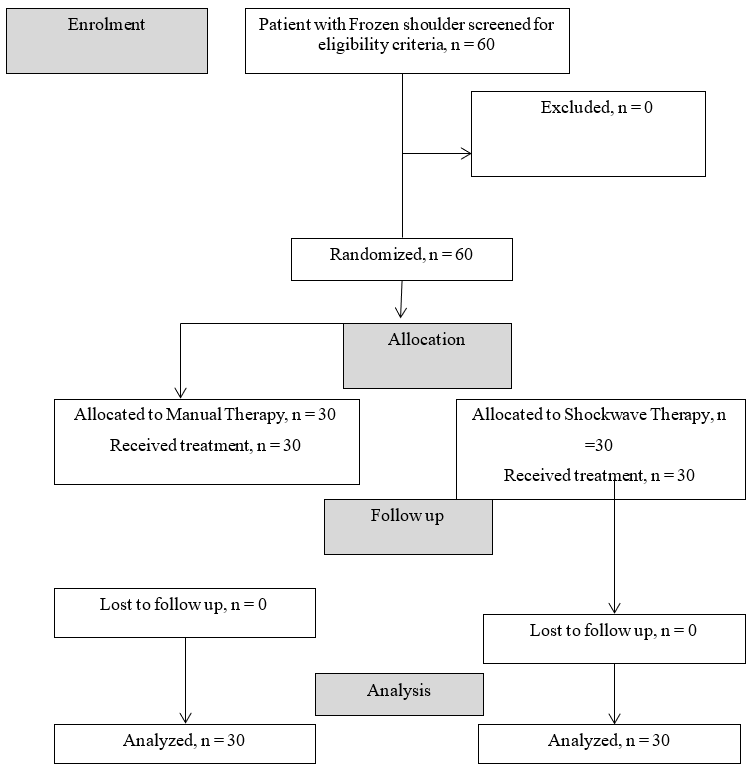
This research was a pilot randomized experiment conducted at a single Centre. The Hospital Ethics Committee accepted the clinical study protocol (NU3111) in November 2022 till January 2024 after it was found to be in compliance with the CONSORT clinical trial guidelines [10].
Prior to their involvement in the study, every participant signed an informed consent form.
Patients
Patients admitted to the Department of orthopaedic physical therapy diagnosed with frozen shoulders according to the guidelines presented in a previous study [11] were deemed eligible for inclusion in the study. The age range for inclusion was 40–60 years old, with shoulder joint pain and restricted range of motion lasting more than four weeks (the stiffness stage of frozen shoulder). The exclusion criteria included the following: involvement in other clinical trials; participation in shoulder trauma that has not been cured; severe osteoporosis or bone lesions as seen from X-rays of the shoulder joint bone; severe mental illness or impaired consciousness; shoulder tumors; rheumatoid or tuberculosis;
neck disease or other diseases radiated to the shoulder; and those who had received other treatments within two weeks prior to the start of the study.
Additionally, patients whose complete data cannot be collected or who got an intraarticular steroid injection during the last six weeks will be excluded. Excluded from the study were patients who withdrew willingly, requested to stop, or failed to finish the course of treatment after being included.
The referring hospital sent a letter of rehabilitation referral to each participant so they could take part in the study. A research leaflet outlining the steps involved in taking part in the study was also given to them. Following their signature on the written informed permission form, participants were divided into two groups using a computer-generated randomization technique: Age 51.22 ± 3.2, male-14, female-16) and manual therapy group (n = 30, age 52.61 ± 3.5, male 13, female-17) demographic data of participants (Table 1).
| Characteristics | Manual Therapy Group(n=30) | Shockwave Therapy Group(n=30) | P-Value |
|---|---|---|---|
| Age | 52.61 ± 3.5 | 51.22 ± 3.2 | 0.596 |
| Gender (Male) | 13(43%) | 14 (47%) | - |
| Gender (Female) | 17(57%) | 16(53%) | - |
| Body mass index(Kg/cm2) | 26.51 | 28.62 | 0.431 |
| Duration (Day) | 57 | 51 | 0.456 |
Table 1: Demographic data of participants.
Through the use of a disguised on-site computer system, a physiotherapy assistant assigned participants. To avoid manipulation, it is best if the person creating the sequence is not the one enrolling the participants. The treating therapist was the only one who knew each participant’s group assignment right before the first intervention. The participants were told they would get one of the two therapies, but they were not told which therapy they were receiving (blind participants).
The therapist who treated the patients could not be blinded because of the nature of the interventions. The concerned intervention was given to both groups for four weeks, at three sessions a week. A therapist who was blinded collected the primary and secondary outcome measures at baseline and four weeks later [12].
Manual Therapy Program
Internal rotation swings, side sliding, front-to-back, back-to-front, up-and-down, abduction sliding to the side of the foot, and separation traction were among the manual therapy techniques used. The patient’s shoulder joint condition informed the application of the Maitland four-level approach. Grade I and II procedures were used to treat joint pain and stiffness; grade III techniques were used to treat joint pain and stiffness; and grade IV techniques were used to treat joint movement limitation brought on by surrounding soft tissue adhesion and contracture.
Shockwave Therapy
Initially, an expert calibrated the ESWT (Zimmer, enPuls Version 2.0, Junkers strabe, Germany) in order to improve and standardize the device’s output. The participant in the ESWT group was instructed to sit with their forearm resting on a flat surface, their elbow flexed at 90_, and their shoulder passively abducted at 80. Under 1.5 bar of air pressure, the therapy began with 250 “warm up” pulses to prepare the patient for the radial ESWT treatment. After the patient was at ease with the procedure, the air pressure was raised to 3.5 bar and 2000 pulses were delivered using a 15-mm applicator at a frequency of 8 Hz of dose, with an energy flux density (EFD) of 0.16 mJ/mm2 and were administered in two shoulder regions. The first 1000 impulses were applied in an anterior-to-posterior direction at the anterior shoulder joint, and the upper margin of the treatment zone was about one finger’s breadth lateral to the coracoid process .The remaining 1000 impulses of the total 2000 impulses per session were applied in a posterior to- anterior direction on the posterior side of the shoulder joint located beneath the lateral border of the scapular spine [8]. For the placebo group, the same set of treatments was provided but in providing ESWT, a special head that blocked the shockwaves from occurring was used but it was indistinguishable to the study participants.
Outcome Measures
The visual analogue scale (VAS) was used to quantify the participant’s subjective pain intensity. The 10-cm point scale allowed for ratings ranging from ‘no pain’ (0) to ‘worst imaginable pain [13].
Flexibility of movement Measurements of lateral rotation and shoulder abduction were made using a universal goniometer. When performed by the same physical therapist, the goniometric passive range of motion assessments for the shoulder seem to be very accurate [14].
Ability to function with impairment the upper limb physical limitations and symptoms associated with frozen shoulder were measured using the limitations of the Arm, Shoulder and Hand questionnaire (Quick-DASH). It has eleven components overall, with each item’s five-point Likert scale measurement and total score ranging from 0 (no impairment) to 100 (most severe disability). The Quick-DASH is a reliable and valid tool that can be used to assess changes in impairment in individuals with shoulder problems [15].
Statistical Analysis
A statistician who was not involved in the study’s recruitment, assessment, or treatment phases carried out the data analysis. The Kolmogorov-Smirnov test was used to assess the homogeneity of the study. An intention-to-treat analysis was used to conduct the data analysis.
Following a 4-week follow-up period and the collection of all outcome variables between the two groups at baseline, the analysis was conducted step-by-step.
Commercial statistical software (IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY, IBM Corp.) was used to run the statistical analyses, and a significance level of p < 0.05 was used for all tests.
Results
There were no significance differences between both groups at demographic data at a level of significance of p ≤ 0.05 (Table 1).
There were no significance differences between both groups at pain measured by VAS before the treatment at manual therapy group was 7 ± 1.4 and at the shock wave group 7 ±1.6 after the treatment there were significance differences between both groups was at manual therapy group was 3 ± 1.1 and at the shock wave group 2 ±1.8 at p ≤ 0.001.
There were no significance differences between both groups at range of motion of abduction before the treatment at manual therapy group was 90 ± 3 and at the shock wave group 89 ±2 after the treatment there were significance differences between both groups was at manual therapy group was 117 ± 2 and at the shock wave group 122 ±4 at p ≤ 0.001.
There were no significance differences between both groups at range of motion of lateral rotation before the treatment at manual therapy group was 30 ± 2 and at the shock wave group 29 ±1 after the treatment there were significance differences between both groups was at manual therapy group was 44 ± 1 and at the shock wave group 49 ±2 at p ≤ 0.001.
There were no significance differences between both groups at functional disability Q DASH before the treatment at manual therapy group was 77 ± 2 and at the shock wave group 79 ±3 after the treatment there were significance differences between both groups was at manual therapy group was 45 ± 1 and at the shock wave group 34 ±2 at p ≤ 0.001 (Table 2).
| Variables | Manual Therapy group | Shockwave group | P value | Significance |
|---|---|---|---|---|
| VAS | 7 ± 1.4 | 7 ± 1.6 | 0.343 | No significance |
| Before treatment | ||||
| VAS | 3 ± 1.1 | 2 ± 1.8 | 0.001 | Significance |
| After treatment | ||||
| ROM of Abduction (Degrees) | 90 ± 3 | 89 ± 2 | 0.443 | No significance |
| Before treatment | ||||
| ROM of Abduction (Degrees) | 117 ± 2 | 122 ± 4 | 0,001 | Significance |
| After treatment | ||||
| ROM of lateral rotation (Degrees) | 30 ± 2 | 29 ± 1 | 0.367 | No significance |
| Before treatment | ||||
| ROM of lateral rotation (Degrees) | 44 ± 1 | 49 ± 2 | 0.001 | Significance |
| After treatment | ||||
| Functional Disability Q-DASH (0–100) Before the treatment | 77 ± 2 | 79 ± 3 | 0.455 | No significance |
| Functional Disability Q-DASH (0–100) after the treatment | 45 ± 1 | 34 ± 3 | 0.001 | Significance |
Table 2: comparison between both groups before and after treatment in all variables.
Discussion
The precise etiology of frozen shoulder remains unclear to this day. Studies on histology and immunocytochemistry have shown that fibroblasts converted to myofibroblasts in tandem with active fibroblast proliferation. Patients with frozen shoulder have also been shown to have fibrosis and inflammation in their shoulder joints. The main reason why individuals with frozen shoulder have restricted movement and pain is because of structural alterations in the soft tissues surrounding the shoulder joint. Reducing discomfort and increasing shoulder joint range of motion have long been the main goals of treatment for this illness [16].
Treating shoulder pain with an emphasis on ROM improvement, joint cavity volume expansion, and adhesive joint tissue loosing was a better approach. To date, there is a lack of high-quality research comparing the benefits of shoulder joint tissue adhesion improvement between rehabilitation manual treatment and joint loosening performed while under anesthesia. When treatment costs and patient acceptability are considered, manual therapy is still the most often utilized technique for treating frozen shoulder [17].
Patients with shoulder pain have previously been successfully treated with impairment-based therapies. The degree to which this study’s ROM, pain, and disability scores improved are consistent with those of prior studies examining the benefits of manual therapy in conjunction with exercise regimens. The training regimens detailed in the previously published literature, where generic non- stretching shoulder exercises were primarily used, are not comparable to the home stretching program utilized in the current study. Furthermore, unlike in the current study, interventions (either manual therapy or exercises) were not modified for their patients during and in between sessions. Our trial was unique in that treatment advancement at subsequent visits was contingent upon the results of the reassessment. Few studies, as far as we are aware, consider reassessment [18].
ESWT is the term used to describe a sequence of acoustic pulses with a certain energy density that are delivered by a suitable generator to a designated target area, hence producing a therapeutic effect. Shockwave energy can firstly enter the affected area through bodily fluids and tissue, enhance local blood flow distribution, encourage the activation of immunological and molecular reactions, stimulate angiogenesis, encourage microcirculation, raise cell oxygen carrying, produce anti-inflammatory effects, and reduce pain, and Secondly, ESWT has the ability to decrease nuclear factor kappa B expression, increase nitric oxide levels, and encourage the development of endothelial nitric oxide synthase activity. Third, shockwave therapy has the ability to create a cavitation effect between tissues, release intratissue, encourage adhesion separation, and release the tissue that is adhesive [19].
Fourth, this technique can alter the frequency at which nociceptors accept pain, alter the chemical mediators around nociceptors, alter the number of free radicals surrounding cells, produce analgesics, and prevent the transmission of pain signals. Fifth, super stimulation of nerve terminals, decreased sensitivity to nerves, interference with nerve conduction, and pain relief are all possible with local high- intensity shockwaves. Lastly, several basic investigations have shown an increase in tissue regeneration, a decrease in tissue apoptosis, and an effective recruitment of fibroblasts [20].
Our study was comparison between manual therapy and shockwave in treatment of frozen shoulder. There was improvement at pain measured by VAS and the range of motion at lateral rotation and abduction, beside improvement of functional activities measured by Functional Disability Q-DASH.
It was noteworthy that shockwave was evidently helpful for patients with frozen shoulder in our trial; nevertheless, there was insufficient data at the time to conclude that shockwave may be administered on its own to treat frozen shoulder, and additional clinical research may be required. Shockwave treatment may be used as an additional treatment for individuals who have frozen shoulders.
Limitation of this study was the small number of sample size and no Magnetic Resonance data available after the treatment.
Conclusion
This study discovered that shockwave approach, as opposed to conventional manual therapy, was more beneficial in helping patients with frozen shoulder restore the joint function. In addition, Shockwave approach proved to be more effective in reducing pain than conventional manual therapy. As a result, we draw the conclusion that shockwave approach is an efficient supplementary therapy for frozen shoulder.
Declarations
• Ethics Approval and Consent to Participate: All study procedures were performed in accordance with the Helsinki Declaration of Human Rights of 2013. The study was authorized by The Committee for Scientific Studies at the Hospital of Kasr Al Inini Orthopaedics in February
2022 (No. 148), and the trial started on 26 of February 2022 and finished on 26 of May 2023.
- Authors Contributions: Sahar Ahmed Abdalbary, did the conception, and design of the work, Abdoulrahman Saied, did the clinical tests and revision, Ehab El- Shaarawy, drafting the work or revising it for, Abdeaziz El- Shaarawy, did Statistical analysis and writing.
- Acknowledgements: The corresponding author would like to thank Mr. Abdallah A. Selim for his support and help with completing this article.
References
-
Rangan A, Brealey SD, Keding A, Corbacho B, Northgraves M, et al. (2020) Management of adults with primary frozen shoulder in secondary care (UK FROST): a multicentre, pragmatic, three-arm, superiority randomised clinical trial. Lancet 396(10256): 977-989.
-
Le HV, Lee SJ, Nazarian A, Rodriguez EK (2017) Adhesive capsulitis of the shoulder: review of pathophysiology and current clinical treatments. Shoulder Elbow 9(2): 75-84.
-
Ryan V, Brown H, Minns Lowe CJ, Lewis JS (2016) The pathophysiology associated with primary (idiopathic) frozen shoulder: a systematic review. BMC Musculoskelet Disord 17(1): 340.
-
Abrassart S, Kolo F, Piotton S, Chih-Hao Chiu J, Stirling P, et al. (2020) ‘Frozen shoulder’ is ill-defined. How can it be described better? EFORT Open Rev 5(5): 273-279.
-
Wong CK, Levine WN, Deo K, Kesting RS, Mercer EA, et al. (2017) Natural history of frozen shoulder: fact or fiction? A systematic review. Physiotherapy 103(1): 40-47.
-
Areeudomwong P, Buttagat V (2019) Proprioceptive neuromuscular facilitation training improves pain- related and balance outcomes in working-age patients with chronic low back pain: a randomized controlled trial. Braz J Phys Ther 23(5): 428-436.
-
Peteraitis T, Smedes F (2020) Scapula motor control training with proprioceptive neuromuscular facilitation in chronic subacromial impingement syndrome: a case report. J Bodyw Mov Ther 24(3): 165-171.
-
Zhang R, Wang Z, Liu R, Zhang N, Guo J, et al. (2022) Extracorporeal shockwave therapy as an adjunctive therapy for frozen shoulder: a systematic review and meta-analysis. Orthop J Sports Med 10(2): 23259671211062224.
-
Mengiardi B, Pfirrmann CW, Gerber C, Hodler J, Zanetti M (2004) Frozen shoulder: MR arthrographic findings. Radiology 233(2): 486-92.
-
Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, et al. (2012) CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg 10: 28-55.
-
Rangan A, Hanchard N, McDaid C (2016) What is the most effective treatment for frozen shoulder? BMJ 354: i4162.
-
Nambi G, Alghadier M, Ebrahim EE, Vellaiyan A, Tedla JS, et al. (2022) Comparative effects of Mulligan’s mobilization, spinal manipulation, and conventional massage therapy in cervicogenic headache-a prospective, randomized, controlled trial. Healthcare (Basel) 11(1): 107.
-
Riddle DL, Rothstein JM, Lamb RL (1987) Goniometric reliability in a clinical setting. Shoulder measurements. Phys Ther 67(5): 668-673.
-
Chan HBY, Pua PY, How CH (2017) Physical therapy in the management of frozen shoulder. Singapore Med J 58(12): 685-689.
-
Alnahdi AH (2021) Validity and reliability of the Arabic quick disabilities of the arm, Shoulder and Hand (QuickDASH-Arabic). Musculoskelet Sci Pract 53: 102372.
-
Mamarelis G, Moris D (2021) Frozen shoulder. Lancet 397(10272): 372-376.
-
Park YH, Park YS, Chang HJ, Kim Y (2016) Correlations between MRI findings and outcome of capsular distension in adhesive capsulitis of the shoulder. J Phys Ther Sci 28(10): 2798-2802.
-
Doner G, Guven Z, Atalay A, Celiker R (2013) Evalution of Mulligan’s technique for adhesive capsulitis of the shoulder. J Rehabil Med 45(1): 87-91.
-
Zhang J, Zhong S, Tan T, Li J, Liu S, et al. (2021) Comparative efficacy and patient-specific moderating factors of nonsurgical treatment strategies for frozen shoulder: an updated systematic review and network meta-analysis. Am J Sports Med 49(6): 1669-1679.
-
Yang QX, Tan YS (2020) Treatment of scapulohumeral periarthritis with massage combined with extracorporeal shock wave. Article in Chinese. Chin Manip Rehabil Med 7: 36-38.
- Electrolyte Considerations for Athletes
- Comprehensive Rehabilitation in Adults with Diabetic Peripheral Neuropathy: A Literature Review on Frequency, Intensity, and Duration Parameters
- Exercise Duration and Its Association with ADHD Symptom Severity in Children and Adolescents: A Parent-Reported Survey Study
- Adaptation of the Adult Neurophysiology of Pain Questionnaire for Use in Pediatrics
- A Non-Pharmacological Multidisciplinary Pain Program within a Hospital Wellness Program: A Mixed Methods Study
- The Effect of Frenkel's Exercise with PNF on Functional Reach in Stroke Survivors: A Randomized Control Trial