Bioequivalence Trial of Two Piracetam 800 Mg Immediate- Release Oral Tablets in Mexicans: Insights in the Use and Abuse of Nootropics
Objective: To share pharmacokinetic data and a bio-analytical method for the conduction of a bioequivalence trial of Piracetam 800-mg immediate release tablets in Mexicans. Methods: Twelve male and 18 female healthy volunteers were administered with a single oral dose of one 800-mg Piracetam tablet under fasting conditions, in a cross-over design study, with blood sampling up to 24 h post-dose. Piracetam was measured by tandem Mass Spectrometry coupled to Ultra-Performance Liquid Chromatography (UPLC-MS/MS) using metronidazole as internal standard. Logarithmic ratios of maximal plasma concentration (Cmax ) and Area Under the Curve (AUC) were used to establish 90% Confidence Intervals [CI] for bioequivalence. Results: Both formulations (Nootropil™ as reference product, and PIRACETAM generic formulation as test product) were safe and well tolerated. The analytical method proved to be linear with accuracy and precision within a range of 1-60 μg/mL; 90% CI for and were [82.62–94.68] and [95.22–102.06]. Cmax was reached at approximately 1 h, and plasma elimination half-life (t1/2) was around 5.1 h for both products. Conclusion: Assayed products met the criteria established by the Mexican regulatory agency (COFEPRIS) to be declared bioequivalent. Mexican population appears to be a high absorber of Piracetam, exhibiting a 300% higher and an ABC0-inf 60% greater than other populations previously reported.
Introduction
Piracetam (PIR) [2-(2-oxopyrrolidin-1-yl) acetamide] (CAS No. 7491-74-9) is the first small molecule (142.074 g/mol) synthetized with nootropic properties, that means “a cognitive enhancer”. PIR is a cyclic derivative of the neurotransmitter gamma-aminobutyric acid with a very high-water solubility (479 mg/mL at 20°C; log P=-1.7) and basic characteristics [1]. PIR is a white powder that exists as a combination of two major polymorphic crystal forms (predominantly P3, and P2 in a less amount; P1 is a metastable form produced during sublimation conditions); P3 is more stable and lightly less soluble than P2, and there is a possible conversion of P3 toward P2 during wet granulation along the tablet manufacturing [2, 3]. Due to these properties, PIR is commercially available in Mexico as oral solutions and immediate-release tablets.
Because of PIR is almost freely soluble in water, and its bioavailability is complete (almost 100%) it is classified as BCS class I product, with a linear pharmacokinetic over a range of doses from 400 mg to 3200 mg/day [4]. Following a single oral dose during fasting conditions, PIR is fast and extensively absorbed, with a peak plasma concentration ( max C ) of around 1 h; food intake decreases max C by 17% and prolong time to reach max C ( max T ) up to 1.5 h. Peak concentrations in cerebrospinal liquid is observed 5 h post- dose. Volume of distribution is 0.6 L/kg, diffusing to all tissues except adipose one, and penetrates into many cellular membranes (neurons, endothelium and erythrocytes). PIR is not bound to plasma proteins and it is not metabolized by humans; thus, it is practically eliminated unaltered (more than 90%) in the urine. Its plasma elimination half-life is around 5 h, with a total body clearance of 80-90 mL/min [1].
Formerly, PIR has been used in the therapy of vascular cognitive impairment (senile dementia), vertigo, sickle cell anemia and stroke. It might increase Reading comprehension in dyslexic children, improve alertness, socialization and cognition in elderly psychiatric patients, without depicting sedation, stimulation or addiction. PIR has also been used in the control of alcoholism, and apparently during long- term treatment seems to slow the progression of Alzheimer’s disease [5]. It is interesting to note in the PubMed monitoring that during the last decade it has had a notorious increase in the number of papers related to nootropic molecules, from molecular mechanisms to novel clinical applications, particularly on central nervous system disorders such as: a) cognition/memory, b) epilepsy/seizures, c) protection in neurodegenerative diseases, d) stroke/ischemia and e) stress management / anxiety. Recent meta-analysis has demonstrated that PIR exhibited neuroprotective effects when used during coronary bypass surgery. It was also effective in the treatment of cognitive disorders of vascular or traumatic origins; and also, its anxiolytic effect was higher than its memory enhancer properties. As an adjuvant, it appears to benefit in myoclonus epilepsy and tardive dyskinesia [6].
Therapeutic effects of PIR seem to be related with at least four mechanisms at cellular level. The first one is mediated by its low affinity to the AMPA- glutamatergic receptor; the density of such receptors is up-regulated in the synaptic zone, promoting the calcium influx in brain cells and the potassium- dependent release of glutamate at the CNS. The second -rheological mechanism- is through the interaction of PIR with the negative polar heads of phospholipids in aged membrane cells, restoring membrane fluidity that may repair vascular endothelial functions such as production of prostacyclin and nitric oxide, and increasing blood flow in compromised cerebral regions [5, 7]. Third - anti- inflammatory mechanism- is related to the inhibition of alpha TNF -induced production of the chronic pro- inflammatory cytokine IL-1beta and a decrease of oxidative stress markers [8]. Finally, new insights suggest a fourth anti- apoptotic mechanism, in which PIR blunts the translocation of mitochondrion-specific proteins of caspase- independent pathway, and attenuates oxidative DNA fragmentation [9].
Thus, considering the previous information and the lack of bio-waiver in our regulatory framework, it is important to share pharmacokinetic data in Mexican population through a controlled bioequivalence trial of a generic product of Piracetam, a nootropic molecule which new evidences suggest that could play important roles along the rehabilitation of language abilities in aphasia of post- stroke patients [10], in the overall management of vascular cognitive impairment [11], in the prevention of suicide associated with certain pharmacogenomic biomarkers [12], and in the reduction of prenatal ethanol-induced neuronal damage [13].
What is Known about this Subject?
- Piracetam is the therapy of election in the treatment of vascular cognitive impairment in elderly patients, vertigo, sickle cell anemia, and numerous other cognitive problems associated to Alzheimer´s disease and stroke.
- Its mechanism of action counteracts biochemical changes in cell membranes, restoring signal transduction in endothelium associated to a better blood perfusion and tissue oxygenation, preventing chronic inflammation and neuronal apoptosis.
What this Study Adds
- There is very succinct information concerning PIR bioequivalence trials.
- Pharmacokinetic data obtained in present study carried out in Mexicans (Latins) shows that this population is a higher/faster absorber compared to original data reported in the information for prescription.
- The Piracetam generic product was well tolerated and met the requirements of Mexican Regulatory Agency (COFEPRIS) to be declared bioequivalent.
- Try to offer a warning about new uses and potential abuse of nootropic molecules.
Material and Methods
Selection of Subjects
Volunteers were recruited at our Clinical facilities. Subjects underwent screening evaluations within 30
days prior to dosing of the first experimental period. Inclusion criteria were: showing willingness to participate, indistinct gender, aged between 18 and 50 years, body mass index between 18 and 27 kg/m2 (inclusive), normal electrocardiogram and clinical history, laboratory values (hematology, urinalysis, serum biochemistry, and liver function) within normal ranges, non-smokers and without active alcoholism, and negative for AIDS, hepatitis B and C, and pregnancy test for women. Exclusion criteria include any kind of allergy, pregnancy, positive results for the rapid assay in urine of drug abuse (benzodiazepines, methamphetamines, cocaine and tetrahydrocannabinol), and any serious health condition that would affect the development of the trial. In addition, subjects who had participated in a bioequivalence study, who had donated blood, or who had been tattooed within 90 days prior to the present trial were excluded.
Volunteer withdrawal situations throughout the study considered any type of hypersensitivity reactions, the loss of two or more blood samples around max C , vomiting between administration times and 2-fold max T , or any dietary transgression. Besides all these, subjects who had increased tobacco consumption or alcohol 48 h prior to dose administrations, or who had taken any prescription and over- the-counter medications, were also withdrawn from the study.
Study Design
The current trial was authorized by the Institutional Review Board registered in the Mexican Regulatory Agency (COFEPRIS registration trial No. 193300410B0194/2019) and conducted in compliance with the latest Declaration of Helsinki, the Good Clinical Practice (ICH) and Mexican regulatory guidelines for bioequivalence trials [14].
The clinical study was controlled, double-blinded (to the medical staff and the analytical investigator), cross- over, two periods (sampling up to 24 h post-dose, with a washout period of 7 days) both under fasting conditions, two treatments (Nootropil™ 800-mg oral tablet from Productos Farmacéuticos, S.A. de C.V. -Mexico- as Reference product and Piracetam 800-mg oral tablet produced by IFA-Celtics S.A. de C.V. -Mexico- as Test product), with two randomized and balanced administration sequences.
The 30 selected volunteers provided their signed informed consent before initial screening procedures and were medically monitored along the entire trial. All subjects were confined within the clinical facility of Pharmometrica on the afternoon prior to drug administration and were assigned a number to maintain the confidentiality of their identity. They received dinner at 8 pm and fasted overnight for 12 h. An intra-vein catheter was placed in the non-dominant arm the following morning and pre-dose samples were taken. At 8 am, all volunteers received a single oral dose of 800 mg of immediate-release PIR tablets of the corresponding product -according to the randomization schedule- with 250 mL of tap water. A mouth-check was done immediately after the tablets were swallowed in order to verify complete tablet intake.
Approximately 5 mL of blood was drawn from each participant for each sampling time through the catheter at 0 h (before dosing), and 0.33, 0.66, 1.00, 1.16, 1.33, 1.50, 1.66, 1.83, 2.00, 2.33, 2.66, 3.00, 4.00, 6.00, 9.00, 12.00, and 24.00 h after PIR administration.
Samples were collected in vacuum heparinized tubes and centrifuged at 4,000 rpm for 5 min at 20 °C for plasma separation. Plasma was placed into identified cryovials and stored at -70 °C until PIR quantitation. Breakfast, lunch, and dinner were served at 10 am, 3 pm, and 9 pm, respectively.
Analytical Method
Several methodologies have been previously reported based on HPLC-UV [15, 16], and more recently in HPLC coupled to tandem mass spectrometry, but employing molecules such as oxiracetam or levetiracetam with no adequate chromatographic performance, or expensive deuterated as internal standards [17, 18]. Thus, it was decided to develop a new method based on UPLC-MS/MS and to validate this according to Mexican guidelines [14], US- FDA guidelines [19], and international considerations for the quantitation of small molecules in biological fluids [20, 21].
Briefly, 20 μL of human plasma (samples of volunteers and calibration standards) was pipetted into 1.5-mL polypropylene micro-tubes. Samples were fortified with 25 μL of metronidazole solution (Internal Standard 400 ng/mL). Tubes were briefly vortex-mixed, and then plasma proteins were precipitated with 500 μL of pure cold methanol. Samples were vortex-mixed for 1 minute and centrifuged at 17,000 × g at 4 °C for 5 min. Fifty μL of supernatant was diluted with 950 μL of pure water, and 2 μL was injected into the chromatographic system (Acquity™ Class- I; Waters Co., Milford, MA, USA). A UPLC BEH C8 column (2.1 x 50 mm, 1.7- μm particle size) at 40°C was used under isocratic conditions (ammonium acetate 10 mM: acetonitrile (99:01 v/v)) at a flux of 0.4 mL/min.
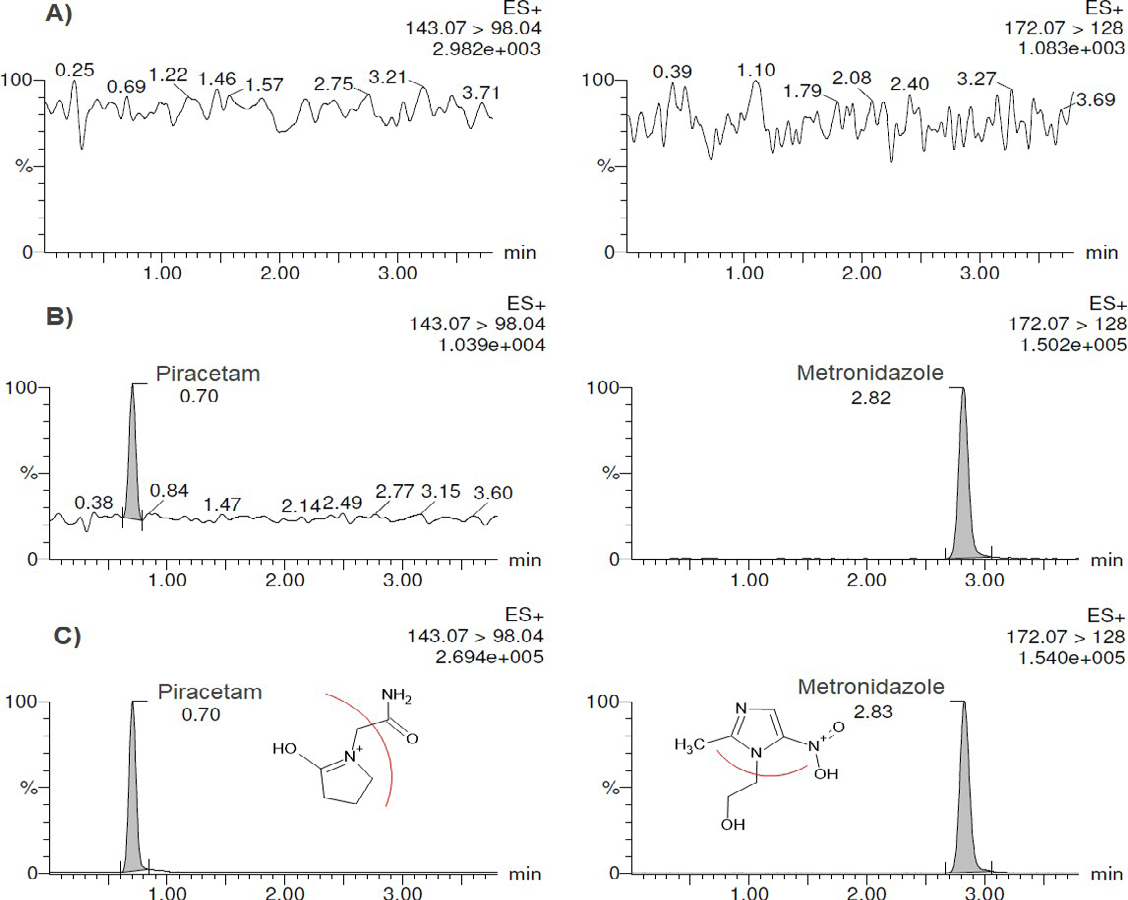
Detection was performed by positive electrospray in a tandem mass spectrometer (Xevo TQ-S Waters Micromass; Manchester, UK), employing the transitions m/z1+ 143.07– 98.04, and 172.07–128.0 for Piracetam and Metronidazole, respectively. Linearity was demonstrated within the range of 1-60 μg/mL. Stability assays covered all of the quantitation- related procedures (on the benchtop, freeze-and-thaw cycles, in the autosampler, long-term).
Statistical Analysis
All statistical calculations for Pharmacokinetics (PK) were performed using Phoenix™ WinNonlin ver. 8.3 software (Pharsight Co., CA, USA). PK parameters were calculated according to the Mexican Norm NOM-177 Statistical Appendix [14] by programming plasma data, a single extravascular dose, and a non-compartmental model.
Maximal plasma drug concentration ( max C ), time to reach maximal plasma concentration following drug administration ( max T ), plasma elimination half-life (t½), area under the plasma concentration–time curve from time zero to last measurable concentration ( 0-24h AUC ), and AUC from time zero extrapolated to infinity ( 0-inf AUC ) comprised the software outputs.
Linear regression of the standardized residuals and the Grubbs test (alpha 0.02) were utilized to detect atypical behaviors in the samples of the subjects evaluated.
ANOVA was employed to evaluate and discard the effects of the sequence, period, and/or treatment in the experimental design.
90% Confidence Intervals (90% CI) of logarithm- transformed relationships for Cmax, 0-24h AUC and 0-inf AUC between both formulations were built. Bioequivalence was concluded if the 90% CI fell within the range of 80-125% for these three PK parameters.
Results
Demographic Description
A total of 30 volunteers were enrolled in the study (12 males and 18 females); all of them completed both periods of the trial and their data were included in the pharmacokinetic and statistical analyses. Demographic data of participants were (mean ± SD): age 33.70 ± 10.47 years; height 1.63 ± 0.07 m; weight 61.80 ± 6.87 kg, and BMI 23.42 ± 2.17 kg/m2.
Pharmacovigilance
The duration of the clinical phase of the protocol was 12 days, including the wash-out period and the date of the last follow-up. Both reference and test products were well tolerated. Three non-serious adverse events were reported during the first period associated with the reference product (moderate pulsatile headache, borborygmus, and one liquid evacuation) in three different male volunteers.
Bioanalytical Method
No missed samples were reported by the clinical staff. Figure 1 shows chromatograms of Piracetam and internal standard in plasma; the bio-analytical method fulfilled all regulatory requirements during its validation, demonstrating linearity (1, 10, 20, 30, 40, 50 and 60 μg/mL; weighting 1/x) with accuracy and precision in a total run time of 4 min (chromatographic capacity factor [k’] = 1.66 for PIR and 9.34 for metronidazole). PIR in plasma probed to be stable at -70°C for at least 65 days.
Pharmacokinetics and Statistical Evaluations
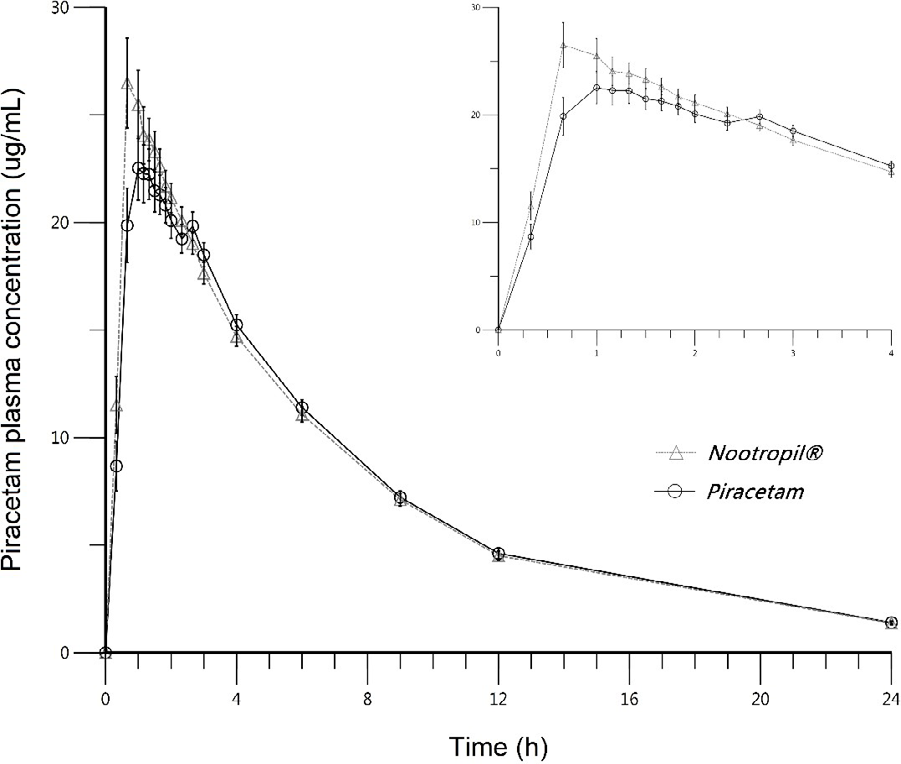
The PK parameters for both test and reference formulations are summarized in Table 1. Mean PIR plasma concentration–time profile is shown in Figure 2.
| Nootropil™ | Piracetam test | |||||
|---|---|---|---|---|---|---|
| Min | Max | Mean | Min | Max | Mean | |
| C max (µg/mL) | 18.89 | 46.82 | 31.7 (22.59) | 19.65 | 39.32 | 27.9 (20.26) |
| T max (h) | 0.66 | 3 | 1.06 (55.0) | 0.66 | 3 | 1.29 (52.5) |
| AUC 0–24h (µg*h/mL) | 113.63 | 265.03 | 168.62 (21.24) | 121.47 | 267 | 166.42 (21.9) |
| AUC 0–inf (µg*h/mL) | 127.93 | 283.58 | 184.42 (19.11) | 137.13 | 289.12 | 182.53 (18.67) |
| t 1/2 (h) | 3.47 | 7.16 | 5.11 (22.21) | 3.31 | 6.79 | 5.1 (22.22) |
Table 1: Mean PIR plasma concentration–time profile is shown in Figure 2.
Table 1: Pharmacokinetic parameters of Piracetam (PIR) after a single oral dose of one 800-mg tablet in a healthy Mexican population under fasting conditions. Geometric Mean ± (%CV). N = 30 (18 females and 12 males) max C (maximal drug plasma concentration), Tmax (time to reach max C 0-24h AUC ), 0-24h AUC (Area Under the Curve up to 24 h), 0-inf AUC (Area Under the Curve extrapolated to infinity), t½ (plasma elimination half-life).
One volunteer was detected as potential outlier for max C and another one for 0-inf AUC according to the Grubbs test (alpha = 0.02). Particularly, the last one was a female volunteer that declared the use of over-the-counter metronidazole vaginal ovules; however, it was decided to include both volunteers in the statistical evaluation due to mandatory conditions by Mexican regulatory guidelines, and none of them impact in the final bioequivalence result.
During ANOVA, no significant sequence or period effects were detected for log- transformed PK parameters. Neither was pre-dose concentrations detected, concluding that the clinical phase was properly conduced.
The 90% CI are reported in Table 2, showing that both formulations meet the requirements established in the Mexican regulatory guidelines for being declared bioequivalent.
| Parameter | Intra- Subject | 90% Confidence Intervals | % Ratio (Test/Reference) | |
|---|---|---|---|---|
| %CV | Lower | Upper | ||
| log (C ) max | 15.61 | 82.62 | 94.68 | 88.45 |
| log (AUC ) 0-24h | 7.91 | 95.22 | 102.06 | 98.58 |
| log (AUC ) 0-inf | 6.14 | 96.46 | 101.79 | 99.09 |
Table 2: Statistics bioequivalence of Piracetam 800-mg immediate - release tablets (Test product) and Nootropil™ 800 mg tablets.
Discussion
Concerning the population that participated in the trial, it may be considered homogeneous in terms of age, weight and body mass index.
In terms of tolerability, it is interesting to note a very low frequency of adverse effects, all of them during the first experimental period and attributable to the reference product; however, all of these were resolved spontaneously during the course of the experimental day (without medication). Regard to the quantitative assay, the present method was fit-for-the purpose of present trial, depicting a short running time and a high throughput with a single-step protein precipitation. Internal standard -metronidazole- was easy to obtain, not expensive, sharing many physic-chemical properties of structure and ionization whit piracetam, and having and adequate chromatographic behavior.
The most remarkable finding of present work is the higher bioavailability of PIR in Mexicans. As can be noted in Table 3, the max C reached on present trial is almost three times higher than that reported in other populations; and ABC0-inf is around 60% greater than reported on these works. Due to PIR is not metabolized by humans (t½ were quite similar among all populations), it suggests that such difference might be attributable to a higher but not a faster absorptive phase ( max T were also very similar. Brazilians seems to be the exception).
| Pharmacokinetics | Pakistanian16 population | Brazilian18 population | German21 population | Mexican population |
|---|---|---|---|---|
| Cmax (µg/mL) | 12.88 ± 2.48 | 9.20 ± 1.90 | 13.70 ± 3.50 | 31.7 ± 7.16 |
| T (h) max | 1.02 ± 0.73 | 2.90 ± 1.40 | 1.50 ± 1.20 | 1.06 ± 0.58 |
| AUC (µg*h/mL) 0–inf | 103.50 ± 29.2 | 128.40 ± 32.1 | 112.60 ± 24.9 | 184.42 ± 35.24 |
| t (h) 1/2 | 5.07 ± 1.61 | 8.90 ± 1.10 | 5.13 ± 0.92 | 5.11 ± 1.13 |
| Sample size (N) | 18 males | 30 both sexes | 8 males | 30 both sexes |
Table 3: Pharmacokinetics of Piracetam after a single oral dose of 800-mg in different populations (Mean ± Standard Deviation).
Finally, considering the growing interest for nootropic drugs and the easy way to obtain it in different countries for non-medical indications, it is essential to raise awareness about the myth of “cognitive enhancers” in order to discourage its consumption among students and professionals, and in the other hand, to avoid the presence of such drugs in dietary supplements and free-access products [22, 23, 24, 25].
Conclusion
The test formulation (Piracetam 800-mg tablets) met the COFEPRIS criteria of bioequivalence as compared with Nootropil™ of Productos Farmacéuticos, S.A. de C.V. Mexico- as Reference product after a single oral dose under fasting conditions, exhibiting minimal adverse effects to those of the reference product.
The contribution of this type of clinical trials lies in their evidencing differences in pharmacokinetics among populations, and strongly suggest as possible to perform bioequivalence trial in the customer population with the local reference product that has evidenced safety and efficacy.
Finally, a warning to sanitary authorities for the potential abuse of nootropics by general population during consumption of non-prescribed products such as dietary supplements.
Acknowledgements
The authors wish to thank Enrique Juárez (Information Services Coordinator, CIDS, Hospital General de México) for his support, as well as Maggie Brunner, M.A., for her editorial assistance. We also thanks to Investigación Farmacéutica S.A. de C.V. (IFA-Celtics) who encourage and share current pharmacokinetic data in Mexican population.
Financial Disclosure
The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Ethical Aspects of the Investigation
The authors state that the clinical protocol was reviewed and approved by an independent Institutional Review Board. In addition, the authors obtained COFEPRIS approval for the conduction of present study. Volunteers signed informed consent, which was formulated according to the latest version of the Declaration of Helsinki (64th General Meeting, Fortaleza, Brazil, October 2013).
References
-
Piracetam is a nootropic cyclic GABA derivative used in myoclonus, sickle cell disease, alcohol dependence, and as a general cognitive enhancer. Piracetam.
-
Potter C, Kollamaram G, Zeglinski J, Whitaker D, Croker M, et al. (2017) Investigation of polymorphic transitions of piracetam induced during wet granulation. Eur J Pharm Biopharm. 119: 36-46.
-
Szeleszczuk T, Pisklak D, Gubica T, Matjakowska K, Kazmierski S, et al. (2019) Application of combined solid-state NMR and DFT calculations for the study of piracetam polymorphism. Solid State Nucl Magn Reson 97: 17-24.
-
Saevels J, De Braekeleer K, Corthout J (2005) Piracetam preparations on the Belgian market: a comparative study. J Pharmacie Belguique 60(3): 92- 96.
-
Winnicka K, Tomasiak M, Bielawska A (2005) Piracetam – an old drug with novel properties? Acta Poloniac Pharm 62(5): 405-409.
-
Malykh AG, Sadaie MR (2010) Piracetam and piracetam- like drugs: from basic science to novel clinical applications to CNS disorders. Drugs 70(3): 287-312.
-
Froestl W, Pfeifer A, Muhs A (2014) Cognitive enhancers (nootropics) Part 3: drugs interacting with targets other than receptors or enzymes. Disease-modifying drugs. J Alzheimer Dis 34(1): 1-114.
-
Navarro S, Serafim K, Mizokami S, Hohmann M, Casagrande R, et al. (2013) Analgesic activity of piracetam: effect on cytokine production and oxidative stress. Pharmacol Biochem Behav 105: 183-192.
-
Verma D, Gupta S, Biswas J, Joshi N, Raju KS, et al. (2018) Metabolic enhancer piracetam attenuates the translocation of mitochondrion-specific proteins of caspase-independent pathway, Poli [ADP- ribose] polymerase 1 up-regulation, and oxidative DNA fragmentation. Neurotox Res 34(2): 198-219.
-
Zhang J, Wei R, Chen Z, Luo B (2016) Piracetam for aphasia in post-stroke patients: a systematic review and meta-analysis of randomized controlled trials. CNS Drugs 30(7): 575-587.
-
Farooq M, Min J, Goshgarin C, Gorelik P (2017) Pharmacotherapy of vascular cognitive impairment. CNS Drug 31(9): 759-776.
-
Niculescu AB, Niculescu HL, Levey DF, Phalen PL, Dainton PL, et al. (2017) Precision medicine for suicidality: from universal to subtypes and personalization. Mol Psychiatry 22(9): 1250-1273.
-
Yang Y, Feng J, Xu F, Wang J (2017) Piracetam inhibits ethanol (EtOH) -induced memory deficit by mediating multiple pathways. Brain Res 1676: 83-90.
-
Guidelines for Bioequivalence Trials in Mexico.
-
Curticapean A, Imre S (2007) New validated method for piracetam HPLC determination in human plasma. J Biochem Biophys Methods 69(3): 273-281.
-
Barkat K, Ahmad M, Minhas M, Malik M, Sohail M (2014) Development of a simple chromatographic method for the determination of piracetam in human plasma and its pharmacokinetic evaluation. Drug Res (Sttutg) 64(7): 384-388.
-
Wang X, Zhu J, Xu R, Yang X, Wu H, et al. (2010) Determination of piracetam in rat plasma by LC-MS/ MS and its application to pharmacokinetics. Biomed Chromatogr 24(10): 1108-1112.
-
Mendes G, Traldi G, Silveira A, Cama J, Lopes R, et al. (2016) Assessment of pharmacokinetic interaction between piracetam and L- carnitine in healthy subjects. Biomed Chromatogr 30(4): 536-542.
-
(2018) Food & Drug Administration, USA.
-
Woolf E, McDougall S, Fast D, Andraus M, Barfield M, et al. (2014) Small Molecule Specific Run Acceptance, Specific Assay Operation, and Chromatographic Run Quality Assessment: Recommendation for Best Practices and Harmonization from the Global Bioanalysis Consortium Harmonization Teams. AAPS J 16(5): 885-893.
-
Kummer von M, Stadler L (1986) Bioäquivalenz von Piracetam nach akutdosierung einer oralen lösung und zweir tablettenpräparationen an probanden. Arzneim- Forsch/ Drug Res 36: 839-845.
-
Carton L, Cabé N, Ménard O, Deheul S, Caous AS, et al. (2018) Pharmaceutical cognitive doping in students: A chimeric way to get-a-head? Therapie 73(4): 331-339.
-
Wilms W, Karczewska MW, Corvini P, Chrzanowski L (2019) Nootropic drugs: Methylphenidate, modafinil and piracetam -Population use trends, occurrence in the environment, ecotoxicity and removal methods- A review. Chemosphere 233: 771-785.
-
Cohen P, Zakharevich I, Gerona R (2020) Presence of piracetam in cognitive enhancement dietary supplements. JAMA Intern Medicine 180(3): 458-459.
-
Sharif S, Guirguis A, Fergus S, Schifano F (2021) The use and impact of cognitive enhancers among university students: A systematic review. Brain Sci 11(3): 355.
- Effects of 5-HTP and Melatonin on the Sleep Cycle of Medical Students
- Adsorption of Bisphenol A on NH4OH- Modified Rice Husk and Sugar Cane Bagasse Biochar
- Comparative Assessment of the Reinforcement Efficiency of Palm Fruit Fibre and Coconut Fibre in High Density Polyethylene (HDPE) Matrix Composite
- Importance of Bio Compounds Naturally Present in Food with Functionality in Animal Metabolism
- Sub-Acute Study on the Cardiotoxic Effects of Monosodium Glutamate Ingestion in Albino Rat
- Weight Management and Its Natural Solutions: A Review