The Placenta in a Case of Thromboembolism and Covid-19
Patient of 37 years old at the 36 weeks of pregnancy with A1298C mutated heterocigote thrombophilia, NK cells, tobacco habit during ten years and cesarean section who received treatment for pulmonary thromboembolism, infection by SARS-CoV-2 and whose pregnancy was disrupted by to present oligohidramnios. The placenta was obtained for their study with light microscope. Destructive villitis, endothelial damage of vessels in stromal region of villi, fibrotic villi, syncytial damage, debris of villi are observed in the intervillous space and virocytes were found during the analysis. The placenta has been found with severe degenerative changes which motivated a rigorous or comprehensive structural study.
Introduction
The thrombus is an aggregation of platelets, fibrin and erythrocytes into a vein or artery provoking the occlusion of the vessel ‘lumen. These can to be retired of their place of formation and are transported to others regions. There is the possibility that maternal blood normally oxygenated has a restricted entry to the uterus-placental tissue by occlusion of uterus placental arteries provoking placental thromboembolism. The patients with thrombus of pelvic vein or deep venous thrombosis [DVT] of the left leg have pulmonary thromboembolism which is asymptomatic. The thrombosis venous of the higher extremity also produces pulmonary thromboembolism [1]. The woman has higher risk of to suffer DVT after delivery since the blood has more tendency to coalesce and the womens which are implicated with caesarean section have higher risk [2].
The incidence of venous thromboembolism during pregnancy is increased 4 to 50 times more when comparing with woman not in pregnancy by changes in the factors of coagulation. This is presented between 1 and 1.5 by each 1000 pregnancies [3]. There is a predominance of thrombotic events during the first trimester of pregnancy [4]. The accuracy of clinical diagnosis of DVT is limited with only half of the patients with DVT have presenting symptoms or positive findings on pertinent physical exam since the presentations of cellulitis, hematoma, venous phlebitis may often confound the diagnosis [5].The use of the thrombolytic therapy raises a concern of high risk of complications. There is a 8% risk of hemorrhage from genital tract [6]; however data has been limited to few case reports [7].
The outbreak of Coronavirus disease 2019[Covid-19] is caused by severe acute respiratory syndrome[SARS] coronavirus 2[SARS-CoV-2].The viruses have killed millions of people and have infected more of one hundred of millions in the world resulting in a pandemic. The transmission of the virus of mother to child is rare. If animals were found to be asymptomatic virus carriers there is the possibility of the spread of the virus as potential route of human to human transmission [8]. The primary mechanism of hypoxemia in early Covid-19 respiratory failure indicates perfusion loss caused by in situ thrombosis. So, postpartum women with diagnosed Covid-19 should undergo anticoagulation treatment [9].
The lesions observed in positive mothers with comorbidities mentioned in the literature of human placenta have seen: Villous oedema, decidual vasculopathy, intramural fibrin deposition, stromal vascular karyorrhexis, thrombosis, perivillous fibrin deposition, chronic villitis, obliterative vasculopathy, infarcts, infiltration of mononuclears cells, intervillous fibrin deposition, increased syncytial nodules, villous agglutination, intervillous hemorrhage, presence of macrophague and T cells,lympho-histiocytic inflammation, accelerated villous maturation, avascular villi, chorioamnionitis, delayed villous maturation and ischemic necrosis of syncytio. These results were obtained in woman pregnancy with diabetes, hypertension or obesity [10]. Many of these lesions have been reported also by us in woman pregnancy and fetal death [11, 12].
Case Report
Patient of 37 years old with 36 weeks of pregnancy, infected by Coronavirus which presented Neumony, severe oligohidramnios and A1298C mutated heterocigote thrombophilia, NK cells increased tobacco habit during ten years and caesarian section. General malaise, myalgy, arthralgy, hyperthermia of 38.6´C, and not productive cough. Received treatment for pulmonary thromboembolism and Covid-19.The pregnancy was disrupted by the presence of oligohidramnios and a live newborn of 3600gr-51cm and their placenta was obtained for observation.
Other placenta of normal pregnancy at term without any pathology was taken as control. Consent informed was given to the woman pregnancy and the approval of the ethical committee of our institution according to Helsinki Declaration. Of each placenta were obtained five small specimens of the maternal surface selected at random from the region central parabasal in the vertical plane.Three slides by specimen were prepared for light microscopy and 45 histological slides in total were stained with H&E. Each slide could to have of 1-3 cuts of 3-5um for their observation.
Results
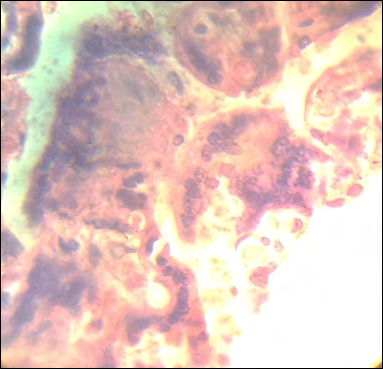
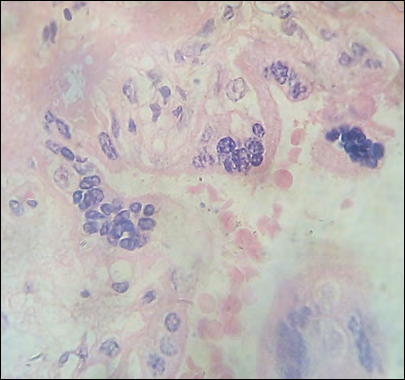
A destructive villitis prorogued by Coronavirus with fragmented villi was showed in the intervillous space (Figure 1). The viral activity attacked the stromal vessels achieving to modify their structure and furtherly the vascular tissue degenerated (Figure 2). In consecuence a fibrotic stroma is originated as noted in Figure 3. Some placental villi are observed with syncytial regions absent or detached (Figure 4). Large nucleus of cytotrophoblasts cells can to be seen when regions of syncytio have missing (Figure 5). Groups of nucleus of syncytio are noted sticking out of the structure of the placental villi (Figure 6). Syncytials nucleus stick out of the villi and resemble exceed the limits of the syncytial membrane (Figure 7). Debris of villi, syncytials picnotic nucleus more bands of fibrinoid are seen in the intervillous space (Figure 8). Some of these sections of the placental tissue showed that the virocyts [arrows] have been witness of the viral activity (Figure 9).
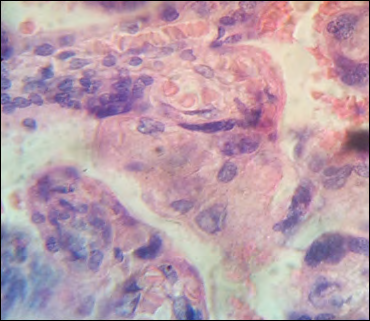
![Figure 2: Zone of stem villi [arrows] where has missing the vessels.H&E.1000x.](/fulltextimages/8023/fig_2.png)
![Figure 3: Some placental villi are observed with syncytial regions absent or detached (Figure 4). Large nucleus of cytotrophoblasts cells can to be seen when regions of syncytio have missing (Figure 5). Groups of nucleus of syncytio are noted sticking out of the structure of the placental villi (Figure 6). Syncytials nucleus stick out of the villi and resemble exceed the limits of the syncytial membrane (Figure 7). Debris of villi, syncytials picnotic nucleus more bands of fibrinoid are seen in the intervillous space (Figure 8). Some of these sections of the placental tissue showed that the virocyts [arrows] have been witness of the viral activity (Figure 9).](/fulltextimages/8023/fig_3.png)
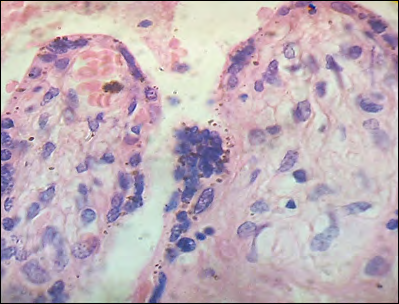
![Figure 4: Villi which has detached syncytial region [arrows] similarly to the indicated by the curba arrow.H&E.1000x.](/fulltextimages/8023/fig_4.png)
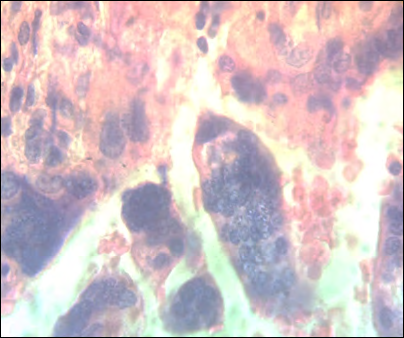
![Figure 9: Virocytes [arrows] or cells with form of owl eye.H&E.1000x.](/fulltextimages/8023/fig_9.png)
Discussion
SARS-CoV-2 infection induce cell tight junction destruction, cell death caused by apoptosis or nechrosis in the syncytio [13] and the platelet aggregation, fibrin deposition and clot formation in the vessels [14] could to be provoking an increased villitis which breaks the structure of the villi. The fetal vascular malperfusion, the thrombotic vasculopathy associated to hypoxia leads to disappearance of vessels [15].
When the placenta becomes infected or develops inflammation, Hofbauer cells may respond by producing pro-inflammatory cytokines or mediators. This reaction can to result in damage to the villous placental barrier and cause a villous fibrotic response associated with chronic inflammation [16]. The findings in placentas from SARS- CoV-2 include the occurrence of an unusual inflammatory lesion, chronic histiocyic intervillositis accompanied by syncytial nechrosis [17]. The trophoblast nechrosis was present predominantly in the areas of intervillositis with the electron microscopy it has been demonstrated the Coronavirus particles in the cytotrophoblasts observed including syncytio, fibroblasts and endothelial cells [18].
SARS-CoV-2 produces an increased multiplication of the nucleus at level of the syncytio with tendency to be expelled to the intervillous space. This latest character observed in our work could to be demonstrated as degeneration and nechrosis of the syncytio noted in the analysis of placenta with SARS-CoV-2 [19, 20]. The virocytes here found are cells of picnotic nucleus with perinuclear halo clear, they contain the virions which have been observed with transmission electron microscopy by Resta et al as spherical particles of 106,720nm with spicular electron dense projections in cellular prolongations [21]. These authors have found besides the destructive effect of the Coronavirus as destroyed syncytio, increased syncytial nodules, deposition of fibrin, infiltration of neutrophils, deciduitis associated to massive nechrosis and arterial thrombosis.
However, Hecht, et al. have found that ACE, a cellular receptor of SARS-CoV-2 is away from the maternal blood and the pronounced paucity of TMPRSS2 expression in the trophoblast are events that explain the limited placental and congenital infection by SARS-CoV-2 and that this virus can infect the placenta but is not associated with specific placental histopathology[22]. To date, placental histopathology in Covid-19 has been investigated in numerous papers although specific features or hallmarks have not been identified [23]. The largest systematic review available on 441 pregnant patients with Covid-19 found that preterm birth is the most common adverse neonatal outcome, reported in the 21% of women who delivered with SARS-CoV-2 [24].
In these cases of thromboembolism associated to Covid-19 whose viruses produce a further thrombosis the antithrombotic therapy is of notable urgency [25]. So, severe degenerative changes are associated to nechrosis of syncytio, stromal vessels destroyed, zones of cytotrophoblasts cells communicating directly with the intervillous space where there is fragments of villi more the presence of virocytes under a degenerated syncytio are the expression of an intensive viral attack to the structure of the placental villi which put in danger the normal interchange of gases and nutrients.
References
-
Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, et al. (2006) Harrison Principios de Medicina Interna, 16th (Edn.), Vol 11, Mexico: Mc Graw Hill.
-
Brewer S, Battarcharya S, Davies J, Meredith S, Preston P (2011) El Embarazo. Gran Bretaña: Dorling Kindersley LTD.
-
Ferrer FM, Oyarzin EE (2014) Trombosis venosa en el embarazo. Rev Med Clin Las Condes 25(6): 1004-1018.
-
Gherman RB, Goodwin TM, Leung B, Byrne JD, Hethumumi R, et al. (1999) Incidence, Clinical characteristics and timing of objectively diagnosed venous thromboembolism during pregnancy. Obstet Gynecol 94(5Pt1): 730-734.
-
Cranley JJ, Canos AJ, Sull WJ (1976) The diagnosis of deep venous thrombosis. Fallibility of clinical symptoms and signs. Arch Sur 111(1): 34-36.
-
Turrentine MA, Braems G, Ramirez MM (1995) Use of thrombolytic for the treatment of thromboembolism disease during pregnancy. Obstet Gynecol Surv 50(7): 534-541.
-
Goldbach D (2018) Catheter directed thrombolysis for massive pulmonary embolism in a pregnant patient. Chest J 154(4).
-
Grudlewska BK, Wiktorczyk KN, Walecka ZE, Kwiecińska- Piróg J, Buszko K, et al. (2021) SARS-CoV-2 Morphology, Transmission and diagnosis during pandemic, Review with elements of meta-analysis. J Clin Med 10(9): 1962.
-
Benhamou D, Keita H, Ducloy BAS (2020) Obstetric Anaesthesia and Critical care club working group. Coagulation changes and thromboembolic risk in Covid-19 obstetric patients. Anaesth Crit Care Pain Med 39(3): 351-353.
-
Sharps MC, Hayes LDJ, Lee S, Zou Z, A Brady C, et al. (2020) A structured review of placental morphology and histopathological lesions associated with SARS-CoV-2 infection. Placenta 101: 13-29.
-
Castejon SOC, Canache CLA, Lara AA, Veroes J (2019) Infection by Coronavirus in the placental villi. Rev Electron Biomed/Electron J Biomed 33: 42-49.
-
Castejon SOC, Canache CLA, Lara AA, Veroes J (2020) Fetal death by Coronavirus: a placental study. Rev Electron Biomed/Electron J Biomed.
-
Zhu N, Wang W, Liu Z, Liang C, Wang W, et al. (2020) Morphogenesis and cytopathic effect of SARS-CoV-2 infection in human airway epithelial cells. Nat Commun 11(1): 3910.
-
Belen AFB, Sarialioglu F (2020) Pulmonar intravascular coagulation in Covid-19: possible pathogenesis and recommendations on anticoagulant/thrombolytic therapy. J Thromb Thrombolysis 50(2): 278-280.
-
Schwartz DA, Graham Al (2020) Potential maternal and infant outcomes from Coronavirus 2019-nCoV [SARS- CoV-2] infecting pregnant woman: Lessons from SARS, MERS and other human coronavirus. Viruses 12(2): 194.
-
Castellucci M, Celoma A, Bartels H, Steininger B, Benedetto V, et al. (1987) Mitosis of the Hofbauer cell. Possible implications for a fetal macrophague. Placenta 8(1): 65-76.
-
Schwartz DA, Baldewijns M, Benachi A, Bugatti M, Collins RR, et al. (2021) Chronic Histiocytic Intervillositis with trophoblast nechrosis and risk factors associated with placental infection from Coronavirus disease 2019[Covid-19] and intrauterine maternal-fetal severe acute respiratory syndrome coronavirus2[SARS-CoV-2] transmission in liveborn and still born infants. Arch Pathol Lab Med 145(5): 517-528.
-
Hosier H, Farhadian SF, Morotti RA, Deshmukh U, Lu Culligan A, et al. (2020) SARS-CoV-2 infection of the placenta. J Clin Invest 130(9): 4947-4953.
-
Shanes ED, Mithal LB, Otero S, Azad HA, Miller ES, et al. (2020) Placental pathology in Covid-19. Am J Clin Pathol 154(1): 23-32.
-
Morotti D, Cadamuro M, Rigoli E, Sonzogni A, Gianatti A, et al. (2021) Molecular pathology analysis of SARS-CoV-2 in syncytiotrophoblast and Hofbauer cells in placenta from a pregnant woman and fetus with Covid-19. Pathogens 10(4): 479.
-
Resta L, Vimercati A, Cazzato G, Mazzia G, Cicinelli E, et al. (2021) SARS-CoV-2 and placenta: New insights and perspectives. Viruses 13(5): 723.
-
Hecht JL, Quade B, Deshpande V, Mino Kenudson M, Ting TD, et al. (2020) SARS-CoV-2 can infect the placenta and is not associated with specific placental histopathology: a series of 19 placentas from Covid-19 positive mothers. Modern Pathol 33(11): 2092-2103.
-
Bertero L, Borella F, Botta G (2021) Placenta histopathology in SARS-CoV-2 infection: analysis of a consecutive series and comparison with control cohorts. Virchow Arch 1:1-14.
-
Gajbhiyl R, Modi D, Mohale S (2020) Pregnancy outcomes, newborn complications and maternal fetal transmission of SARS-CoV-2 in woman with Covid-19:a systematic review of 441 cases. medRxiv.
-
Tarikul IR, Sadia H, Mayukh RM (2021) Venous thromboembolic event in a severe Covid patient despite on thrombophylaxis. Academia Letters.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer