Protracted and Tedious-Indolent T Lymphoproliferative Disorder of Gastrointestinal Tract
Indolent T lymphoproliferative disorder of gastrointestinal tract is an exceptional disorder associated with infiltration of monoclonal T cells within mucosa of gastrointestinal tract.
Editorial
Indolent T lymphoproliferative disorder of gastrointestinal tract is an exceptional disorder associated with infiltration of monoclonal T cells within mucosa of gastrointestinal tract. Generally, a non-destructive infiltrate constituted of miniature, monotonous lymphoid cells demonstrating an immuno-phenotype of CD4+ / CD8- or CD4- / CD8+ appears to infiltrate gastrointestinal mucosa. The exceptionally discerned, indolent T lymphoproliferative disorder of gastrointestinal tract commonly arises within middle aged male subjects, frequently manifests with diarrhoea and exemplifies an indolent clinical course. Although small intestine and colon are commonly incriminated, entire gastrointestinal tract may depict the lesions and no segment of the gut is spared. Indolent T lymphoproliferative disorder represents with a chronic clinical course associated with frequent episodes of disease relapse, inadequate response to cogent chemotherapy and extended survival.
The infrequent, indolent T lymphoproliferative disorder of gastrointestinal tract is predominantly discerned within fifth decade to sixth decade with demonstrable age of disease emergence within 23 years to 79 years. A male predominance is observed with male to female proportion at 2.4:1. The condition is devoid of specific contributory factors [1, 2].
Of obscure aetiology, indolent T lymphoproliferative disorder of gastrointestinal tract preponderantly incriminates small intestine and colon. Nevertheless, no site of gastrointestinal tract is exempt from disease emergence. Exceptionally, lesions are accompanied by regional or abdominal lymph node enlargement or incrimination of bone marrow.
Commonly, indolent T lymphoproliferative disorder of gastrointestinal tract represents with clinical symptoms as abdominal pain and diarrhoea. Additionally, symptoms such as vomiting, weight loss or associated features of malabsorption may be discerned [1, 2]. Clinically, indolent T lymphoproliferative disorder of gastrointestinal tract can simulate diverse inflammatory bowel diseases as ulcerative colitis or Crohn’s disease. Few subjects may demonstrate a history of Crohn’s disease. Besides, indolent T lymphoproliferative disorder is a chronic condition associated with frequent disease relapses. Generally, the disorder is persistent and accompanied by prolonged clinical course with extended survival. Occasionally, the disorder may progress to aggressive T cell lymphoma, a neoplasm delineating adverse prognostic outcomes [1, 2].
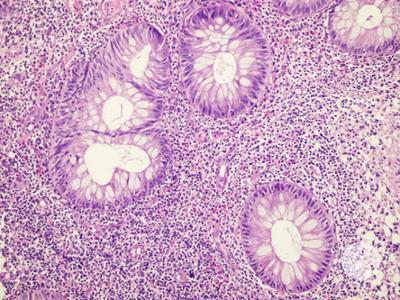
Upon microscopy, lesions demonstrate an intense lymphoid infiltrate confined to lamina propria or superimposed mucosal surface of gastrointestinal tract. Occasionally, the lymphoid infiltrate extends to subjacent submucosa. Lymphoid infiltrate is essentially non- destructive wherein adjacent mucosal glands appear displaced and distorted [3, 4]. The lymphoid infiltrate is comprised of monomorphic, miniature lymphoid cells incorporated with minimal, pale staining cytoplasm, mildly irregular nuclear contour, mature nuclear chromatin and inconspicuous nucleoli. Indolent T lymphoproliferative disorder incriminating the oral cavity may manifest as ulcers accompanied with subjacent infiltrate of lymphoid cells. Characteristically, lesions are devoid of necrosis, ulceration or foci of angiocentric lymphoid infiltrate and angiodestruction [3, 4] (Figures 1,2 & Table 1).

| Presenting clinical symptoms | Recurrent genetic alterations | |
|---|---|---|
| Enteropathy associated T cell lymphoma | Abdominal pain, anorexia, adenopathy, fatigue, infection | Activating mutations of JAK1 and STAT3 |
| Inflammatory bowel disease •ulcerative colitis •Crohn’s disease | Abdominal pain, cramps, diarrhoea, haematochezia, fever, fatigue, anorexia, unintended weight loss | Germline mutations of IL10RA, IL10RB, integrin genes |
| Indolent T lymphoproliferative disorder of GI tract | Abdominal pain, diarrhoea, dyspepsia, food intolerance, vomiting | STAT3-JAK2 fusions in CD4+ lesions |
| NK cell enteropathy | Constipation, diarrhoea, GI bleeding, vague abdominal pain, vomiting | JAK3 K563_CD565del |
| Monomorphic epitheliotropic intestinal T cell lymphoma | Abdominal pain, bowel obstruction, diarrhoea, intestinal bleeding, perforation, weight loss | STAT5B, N642H, loss of function mutations of SETD2 |
Table 1: Differential Diagnosis of Indolent T Lymphoproliferative Disorder of Gastrointestinal Tract [3,4].
Indolent T lymphoproliferative disorder of gastrointestinal tract appears immune reactive to CD2, CD3, CD5, CD7, T cell intracellular antigen 1(TIA1) and T cell receptor beta F1 (TCR-BF1). Besides, lesions exhibiting an immuno-phenotype CD4+ / CD8- or CD4- / CD8+ may be equivocally delineated. Exceptionally, an immuno- phenotype of CD4+ / CD8+ or CD4- / CD8- may appear. Decimation of CD7 is infrequently exemplified. Indolent T lymphoproliferative disorder of gastrointestinal tract is associated with minimal Ki67 proliferative index of ~5%. Indolent T lymphoproliferative disorder of gastrointestinal tract is immune non-reactive to CD30, CD56, granzyme, T cell receptor gamma delta (TCRγδ) or Epstein Barr virus (EBV) [5, 6].
Upon flow cytometry, indolent T lymphoproliferative disorder of gastrointestinal tract simulates cellular immuno- phenotype of mature T lymphocytes. Exceptionally, aberrant decimation of CD7 is observed. Indolent T lymphoproliferative disorder of gastrointestinal tract delineates clonal genetic rearrangements of T cell receptor (TCR) as discerned by polymerase chain reaction (PCR) assay. Repetitive chromosomal translocation t (9; 17) (p24.1; q21.2) STAT3/JAK2 genetic fusion is encountered, especially within instances immune reactive to CD4+ [5, 6]. Genetic alterations as reoccurring genetic mutations and novel rearrangements incriminating genes configuring JAK/STAT pathway are frequently observed [5, 6].
Indolent T lymphoproliferative disorder of gastrointestinal tract requires segregation from neoplasms such as intestinal T cell lymphomas as denominated by enteropathy associated T cell lymphoma (EATL) and monomorphic epitheliotropic intestinal T cell lymphoma (MEITL), celiac sprue and inflammatory bowel disease (IBD) as ulcerative colitis or Crohn’s disease [5, 6]. Surgical tissue sampling of site incriminated within gastrointestinal tract is optimal for discerning the condition [5, 6].
Indolent T lymphoproliferative disorder of gastrointestinal tract demonstrates an unsatisfactory therapeutic response to conventional chemotherapy and immunotherapy. Currently, a suitable treatment regimen employed to manage the condition remains undefined. Factors contributing to pertinent prognostic outcomes remain undocumented [5, 6].
References
-
Fan W, Niu L, He H, Yuan J, Yuan F, et al. (2022) Indolent T-cell lymphoproliferative disorder of gastrointestinal tract with unusual clinical courses: report of 6 cases and literature review. Virchows Arch.
-
David R, Mishra K, Gilbert ER, Mirza KM, Hendler S (2022) Indolent T-Cell Lymphoproliferative Disease: A Rare Case of a Benign Lymphoma of the Gastrointestinal Tract With Extra-Gastrointestinal Involvement. ACG Case Rep J 9(10): e00879.
-
Can K, Li W, Hua Y (2020) Indolent T-Cell Lymphoproliferative Disease of the GI Tract: Insights for Better Diagnosis, Prognosis, and Appropriate Therapy. Frontiers in Oncology 10: 1276
-
Weng CY, Ye C, Fan YH, Bin Lv, Zhang CL, et al. (2022) CD8- positive indolent T-Cell lymphoproliferative disorder of the gastrointestinal tract: A case report and review of literature. World J Clin Cases 10(15): 4971-4984.
-
Soderquist CR, Bhagat G (2022) Indolent T- and NK-Cell Lymphoproliferative Disorders of the Gastrointestinal Tract: Current Understanding and Outstanding Questions. Hemato 3(1): 219-231.
-
Soderquist CR, Patel N, Murthy VV, Aggarwal N, Young KH et al. (2020) Genetic and phenotypic characterization of indolent T-cell lymphoproliferative disorders of the gastrointestinal tract. Haematologica 105(7): 1895- 1906.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer