Merger and Consolidation-Carcinosarcoma-Uterine Cervix
Carcinosarcoma of uterine cervix is an exceptionally encountered, high grade neoplasm composed of malignant epithelial and mesenchymal elements. Additionally designated as malignant mixed mesodermal tumour, homologous neoplasms of uterine cervix are denominated as carcinosarcoma.
Introduction
Carcinosarcoma of uterine cervix is an exceptionally encountered, high grade neoplasm composed of malignant epithelial and mesenchymal elements. Additionally designated as malignant mixed mesodermal tumour, homologous neoplasms of uterine cervix are denominated as carcinosarcoma.
Majority of neoplasms incriminating uterine cervix emerge as extensions of tumefaction arising within the endometrium. Besides, neoplasm may appear as a secondary lesion following exposure to radiation therapy employed for alleviating malignancies as squamous cell carcinoma of uterine cervix.
Carcinosarcoma confined to uterine cavity upon initial representation is frequently encountered and associated with superior prognostic outcomes.
Mean age of disease emergence is 50 years to 65 years although the neoplasm may appear within young subjects as 12 years or elderly population of up to 93 years [1, 2].
Human papilloma virus deoxy ribonucleic acid (HPV DNA) is comprehensively (100%) encountered within neoplastic cells configuring carcinosarcoma of uterine cervix [1, 2].
Cytological assessment with conventional Papanicolaou smear is moderately sensitive for discernment of carcinosarcoma of uterine cervix. Generally, neoplasm may be categorized as a carcinoma in the absence of a distinct mesenchymal component [1, 2].
Occurrence of advanced stage uterine disease with incrimination of lower uterine segment or cervix is accompanied by enhanced proportion of exfoliated, high grade, malignant cells with significant cellular and nuclear pleomorphism. Besides, tumour necrosis may be encountered. Mitotic figures are occasionally exemplified. A definitive mesenchymal component appears absent [2, 3]. Grossly, neoplasm represents as a polypoid tumefaction associated with variable tumour necrosis.
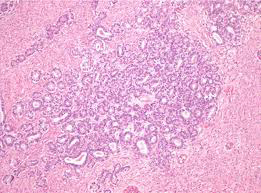
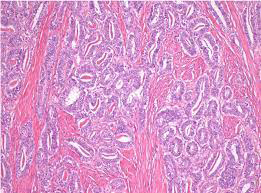
Upon microscopy, carcinosarcoma of uterine cervix appears reminiscent of neoplasm confined to uterine cavity. Tumefaction is comprised of malignant epithelial and mesenchymal components. Frequently, neoplasm is associated with high grade squamous intraepithelial lesion. Tumefaction exhibits an invasive epithelial cellular component which may configure as adenoid basal carcinoma, adenoid cystic carcinoma, basaloid squamous cell carcinoma or keratinizing squamous cell carcinoma. However, an accompanying element of adenocarcinoma is absent [3, 4].
Sarcomatous component of the neoplasm appears as a homologous configuration which recapitulates fibrosarcoma or endometrial stromal sarcoma. Neoplasm is associated with prominent myxoid alterations of surrounding stroma.
Malignant heterologous component of encompassing stroma frequently (~50%) emerges as a rhabdomyosarcoma. Besides, foci of chondrosarcoma or liposarcoma may be exemplified [3, 4].
The biphasic tumour is comprised of an amalgam of adjoining, high grade carcinomatous and sarcomatous elements. Carcinomatous element is preponderantly comprised of high grade endometrioid or serous uterine carcinoma. Nevertheless, majority (~75%) of neoplasms are articulated of serous carcinoma or an admixture of serous and high grade endometrioid carcinoma. Infrequently, clear cell carcinoma may constitute the neoplasm.
Commonly, hybrid cellular morphology ranging between high grade endometrioid carcinoma and serous carcinoma or an undifferentiated carcinoma is encountered [3, 4].
Additionally, epithelial components as squamous cell, mucinous or neuroendocrine cellular components are exceptionally exemplified.
Sarcomatous elements are frequently configured of spindle shaped cells and pleomorphic cellular components [3, 4].
An estimated 50% lesions are constituted of heterologous elements as rhabdomyosarcoma or chondrosarcoma. Notwithstanding, foci of osteosarcoma-like, liposarcoma- like or angiosarcoma-like differentiation are uncommonly enunciated.
Vascular and lymphatic invasion is commonly exemplified, especially within the carcinomatous component [3, 4].
TNM staging of carcinoma cervix 2021 as per American Joint Committee on Cancer (version 9) [3, 4].
Primary Tumour
- TX: primary tumour cannot be assessed
- T0: no evidence of primary tumour
- Tis: carcinoma in situ
- T1: carcinoma cervix confined to the uterus and subcategorized as
- T1a: invasive carcinoma singularly diagnosed by microscopy with depth of invasion < 5 millimetres
- T1b: clinically visible lesion confined to the cervix
- T2: carcinoma cervix which invades beyond the uterus with absent extension to pelvic wall or lower third of vagina
- T2a: tumour with absence of parametrial invasion
- T2b: tumour associated with parametrial invasion
- T3: tumour extends into pelvic wall and/or involves lower third of vagina, and/or causes hydronephrosis
- T3a: tumour involves lower third of vagina with absent extension into pelvic wall T3b: tumour extends into pelvic wall and/or causes hydronephrosis or nonfunctioning kidney T4: tumour invades mucosa of urinary bladder or rectum and/or extends beyond true pelvis
Regional Lymph Nodes
•NX: regional lymph nodes cannot be assessed •N0: regional lymph node metastasis absent •N1: regional lymph node metastases singularly confined to pelvic lymph nodes •N2: regional lymph node metastasis into para-aortic lymph nodes along with or devoid of pelvic lymph node metastasis
Distant Metastasis
•M0: distant metastasis absent •M1: distant metastasis into sites such as pulmonary parenchyma, hepatic parenchyma, distant or inguinal lymph nodes, bone or intraperitoneal disease. Tumour metastasis into pelvic lymph nodes, para-aortic lymph nodes or vagina are to be excluded.
Epithelial and mesenchymal components of carcinosarcoma appear immune reactive to epithelial membrane antigen(EMA), keratin or vimentin. Sarcoma-like component appears immune reactive to muscle specific actin (MSA), smooth muscle actin (SMA) or desmin [5].
Carcinosarcoma of uterine cervix requires segregation from neoplasms such as squamous cell carcinoma with sarcoma-like stroma [5]. Carcinomsarcoma of uterine cervix may be appropriately managed with total abdominal hysterectomy. Contingent to individual specifications, adjuvant radiation therapy or chemotherapy may or may not be employed for disease alleviation [5, 6, 7].
References
-
Fowler JR, Maani EV, Dunton CJ, Brian WJ (2023) Cervical Cancer. Book.
-
Lee JW, Ouh YT, Chang HK, Ha KC, Kyung JM, et al. (2023) Trends in Gynecologic Carcinosarcoma Based on Analysis of the Surveillance Epidemiology End Result (SEER) Database. J Clin Med 12(3): 1188.
-
Shu X, Zhou Y, Wei G, Chen X, Qiu M (2021) Cervical Carcinosarcoma: Current Understanding on Pathogenesis, Diagnosis, Management and Future Perspectives. Clin Med Insights Oncol 15: 11795549211056273.
-
Serouart B, Cordoba A, Martinez-Gomez C (2023) Results of a 20 Year Retrospective Analysis of Early-Stage Cervical Cancer: Should 3 cm Be Considered the New Ariadne’s Thread in Early Cervical Cancer Treatment? Cancers (Basel) 15(5): 1570.
-
Denschlag D, Ulrich UA (2018) Uterine Carcinosarcomas– Diagnosis and Management. Oncol Res. Treat 41(11): 675-679.
-
Comert GK, Turkmen O, Karalok A, Basaran D, Bulbul D, et al. (2017) Therapy Modalities, Prognostic Factors, and Outcome of the Primary Cervical Carcinosarcoma: Meta- analysis of Extremely Rare Tumor of Cervix. Int J Gynecol Cancer 27(9): 1957-1969.
-
Image 1 and 2 Courtesy: BMJ case reports.
- The Muculent Bleb-Mucinous Cystic Neoplasm-Hepatobiliary Region
- Insulin Sensitizers as Anti-Aging Agents: Unveiling Synergies with Albumin, GLP-1RA, Klotho Protein, and Metformin in the Quest to Combat Aging
- Reprogramming of GLP-1 Response at Prediabetes for the Prevention of Type 2 Diabetes: The Role of Albumin and GLP-1 Receptor Agonists
- The Mingled Allies-Combined Hepatocellular Carcinoma and Cholangiocarcinoma
- Compilation and Embodiment-Leydig Cell Tumour Testis
- Glucolipotoxicity: A Novel Different Perspective on the Causes of Cancer