A Case of Atopic Dermatitis with Concurrent Psoriasis Vulgaris: Successful Treatment with Upadacitinib
A case of 22-year-old man with atopic dermatitis (AD) who developed concurrent psoriasis vulgaris (PSO) is presented. PSO is primarily mediated by T-helper (Th) 17 immune responses, whereas AD is predominantly Th2-mediated. Both are distinct diseases, but overlapping cases occur, suggesting they may represent opposite ends of a spectrum of T-cell–mediated inflammatory diseases. The clinical course of this case demonstrates an interesting example of the immunological instability of AD. Based on his clinical feature, this case is suggested to be an intrinsic, Th17-dominant phenotypes different from that of typical AD. The clinical course of this case suggests that the immune environment of intrinsic AD shifted to the opposite direction. Cytokine-targeted therapies may shift immune responses across the disease spectrum. Therefore, upadacitinib, a Janus kinase (JAK) inhibitor, was selected, leading to the satisfactory result. Treatment of atopic dermatitis requires individualized therapeutic choices.
Abbreviations
AD: Atopic Dermatitis; PSO: Psoriasis Vulgaris; TARC: Thymus and Activation-Regulated Chemokine.
Introduction
Atopic dermatitis (AD) and psoriasis vulgaris (PSO) are distinct diseases; however, occasionally co-occur in the same patient. In this case report, we present a case of AD in which clinical findings of PSO emerged during topical steroid therapy. We describe the clinical course and therapeutic strategy employing a systemic agent.
Patient: 22-year-old man. Past history: AD in childhood, which improved after adolescence First visit: February, Year X The patient presented with skin eruptions that had worsened over the preceding month.
Findings at first visit: Eczematous lesions were observed on both forearms and lower legs. No other skin eruptions or generalized skin dryness were observed. Blood tests revealed an immunoglobulin E (IgE) level of 1480 IU/mL (0∼173) and a thymus and activation-regulated chemokine (TARC) level of 794 pg/mL.
Clinical course
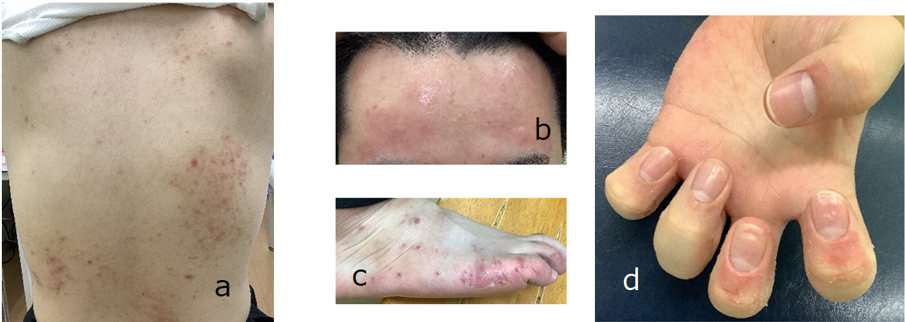
From the initial visit, the use of topical steroids improved the eruptions. • July, Year X: Partially keratotic erythematous plaques appeared on the forehead, and keratotic reddish papules approximately 1 cm in diameter developed on the trunk and extremities. These were mixed with atopic skin lesions and accompanied by intense itching and erosion due to scratching (Figure 1A–C). Many lesions were unresponsive to topical steroids (betamethasone butyrate propionate) but improved with a combination of steroids and active vitamin D3 (betamethasone butyrate propionate + maxacalcitol; hereafter, “combination preparation”), which is primarily used for psoriasis (PSO). Topical steroids were applied to the AD-like eruptions, and the combination preparation was applied to the PSO-like keratotic erythema. Both manifestations improved.
• August, Year X: A biopsy was taken of the keratotic eruptions on the dorsum of the foot after a 3-week washout period for topical agents.
• September, Year X: Periungual inflammation and nail deformities with pitting were noted (Figure 1D). No joint symptoms were observed. The combination preparation was applied periungually, with limited efficacy.
• August, Year X+1: Following a coronavirus disease 2019 infection, all skin eruptions worsened. Both AD-like and PSO-like eruptions occurred on the trunk, face, and neck. Topical delgocitinib and excimer light irradiation provided limited improvement.
• December, Year X+1: Generalized eruptions persisted. Irritated erythematous lesions with epidermal desquamation and fissures appeared on the palmar and plantar surfaces, causing pain while walking (Figure 3).
These lesions responded poorly to local therapy.
• Oral cyclosporine (CYA) (100 mg) was initiated, resulting in marked improvement in all lesions. However, symptoms worsened upon dose reduction; therefore, CYA treatment was continued for 3 months.
• March, Year X+2: CYA was discontinued, and upadacitinib (15 mg) was initiated. Subsequently, the eruptions showed sustained improvement. A mild elevation of liver enzymes was noted 2 months after upadacitinib was initiated; this elevation nearly resolved after 6 months.
• May, Year X+3: While continuing upadacitinib, the patient exhibited occasional mild erythema on the extremities, forehead, and periauricular areas, which improved with topical steroids. There was no skin eruption on the palmar-plantar lesions.
Pathological findings
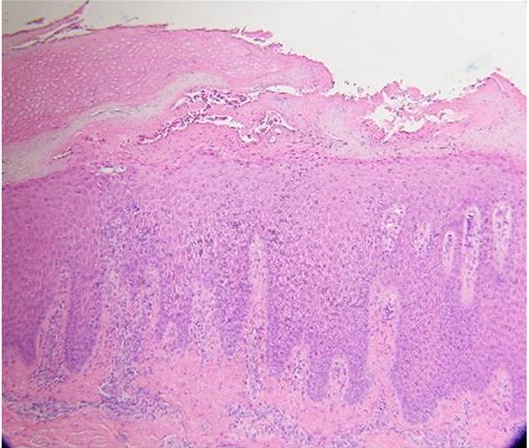
Histopathology showed regular elongation of the rete ridges, spongiosis, and parakeratosis, findings consistent with psoriasis. However, neutrophil infiltration into the stratum corneum and vascular proliferation in the dermal papillae were absent (Figure 2). These eruptions were considered “PSO-like.”

Discussion
The author reported a case in which psoriatic symptoms developed after treatment was initiated for atopic dermatitis.
Psoriasis is primarily mediated by T-helper (Th) 17 immune responses, whereas AD is predominantly Th2- mediated. Both are distinct diseases, but overlapping cases occur, suggesting they may represent opposite ends of a spectrum of T-cell–mediated inflammatory diseases [1]. Moreover, intrinsic, Th17-dominant phenotypes may exist in AD [2]. In this case, IgE level was moderately elevated at the first visit, but the absence of xerosis suggested that this is a phenotype different from that of typical AD. The clinical course of this case suggests that the immune environment of intrinsic AD shifted to the opposite direction. On the other hand, since the eruption worsened after coronavirus disease 2019 infection, it is considered that the infection triggered an increase in disease activity.
Cytokine-targeted therapies may shift immune responses across the disease spectrum. Therefore, upadacitinib, a Janus kinase (JAK) inhibitor, was selected in this case.
In PSO, interleukin (IL)-17 and IL-23 inhibitors achieve disease control in approximately 90% of patients [3]. By contrast, AD involves multiple immune axes, requiring individualized therapeutic strategies.
This case illustrates the immunological diversity of AD. Its clinical course also highlights a therapeutic option for AD patients with diverse immunological backgrounds. At the time of writing, the patient has maintained disease control for more than 1 year after JAK inhibitor therapy. Continued observation is necessary to ensure long-term efficacy.
Conflict of Interest
The author declares no conflicts of interest.
Ethics Statement
I got consent from the person concerned.
References
-
Yassky EG, Krueger JG (2017) Atopic dermatitis and psoriasis: two different immune diseases or one spectrum. Current Opinion in Immunology 48 (2017): 68-73.
-
Tokura Y (2010) Extrinsic and intrinsic types of atopic dermatitis. Journal of Dermatological Science 58: 1-7.
-
Schabitz A, Eyerich K, Stark NG (2021) So close, and yet so far away: The dichotomy of the specific immune response and inflammation in psoriasis and atopic dermatitis. Journal of Internal Medicine 290: 27-39.
- Epithelioid Granuloma; 3cases with Different Clinical Features
- Advancing Representation in Dermatology Clinical Trials: Ethical, Scientific, and Regulatory Imperatives for Inclusion Across all Fitzpatrick Skin Types
- Innovation Lifting Eyeshadow: A Synthesis of Makeup and Optical Illusion
- Distinguishing Superficial Actinic Porokeratosis from Actinic Keratosis with UVF Dermoscopy: A Case Report
- High Mobility Group Box 1 (HMGB1) in Cutaneous Inflammation: An Immune Modulator Bridging Cellular Stress, Ferroptosis and Danger Signaling
- Knowledge, Attitude, and Practices towards Leprosy among Nurses around Semarang, Indonesia