Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features: Pitfalls of Cytological and Histopathologic Diagnosis
Classical papillary thyroid carcinoma (PTC) is the commonest primary thyroid neoplasm. Besides PTC, significant histological variants that differ from classical PTC in regard to the morphological, cytologic and histologic features are mentioned; among them is follicular variant papillary thyroid carcinoma (FVPTC). The update WHO classification and the update Bethesda system reclassified FVPTC introduced a new entity which is "non-invasive follicular thyroid neoplasm with papillary like nuclear features" (NIFTP) that is characterized by an indolent behavior with encapsulated noninvasive growth features. Recently this entity is considering one of an indeterminate cytological categories (category III-IV-V). Update studies are found a combination of triple diagnostic procedures included sonographical, cytologic and molecular investigations can be suspecting preoperative diagnosis. Methods: A total of 150 selected cases of solitary thyroid nodules (STNs) with preoperative FNAC have an indeterminate follicular patterned cytological lesions with their underlying thyroidectomies that were collected in a 5-year period included in this article. Results: Majority of our cases were females and suffering from neck swelling. Cytollogically all the enrolled cases were lying in the indeterminate categories and histologically they were encapsulated with variable sizes follicles, nuclear features, no vascular invasion, no psammoma bodies, no tumor necrosis or mitosis. Also, there is no any extra-thyroid invasion. Conclusion: The accurate diagnosis of this entity “”NIFTP” carries many congratulations in regard that is “not malignant” category among both update TBSRTC and the final histopathological examination of the excised thyroid tissue.
Introduction
Anatomically, thyroid gland has two lateral lobes connected by a narrow median bridge called isthmus. The normal size of the lobes of the thyroid gland has been described to be 5 cm long, 3 cm wide, and 2 cm thick. In some cases, an additional lobe is present, which is known as the Pyramidal Lobe [1, 2]. Majority of thyroid tumors are predominately follicular cells derived neoplasm. They broadly divided into benign and malignant. Some thyroid tumors are difficult to clearly diagnose as benign or malignant. Therefore, the update publication of World Health Organization (WHO) classification of endocrine neoplasia, listed borderline thyroid lesions such as well-differentiated tumor of uncertain malignant potential (WDT-UMP), follicular tumor of uncertain malignant potential (FT-UMP), as well as reclassified the follicular variant of papillary carcinoma into invasive and encapsulated one and entitled the later as noninvasive follicular thyroid neoplasm with papillary- like nuclear features (NIFTP) [3]. In collaboration with the update WHO, the Endocrine Pathology Society working group (ESP-WG) concluded that the absence of invasion among the encapsulated follicular variant papillary thyroid carcinoma (EFVPTC) was associated with an indolent biologic behavior may be similar to follicular adenomas as well as the patients were treated conservatively with lobectomy without need to radioactive iodine (RAI). They proposed a new diagnostic entity “noninvasive follicular thyroid neoplasm with papillary like nuclear features” (NIFTP). The introduction NIFTP as a non-invasive neoplasm had important implications for the cytological interpretation of STNs as well as significantly impacts the risk of malignancy (ROM) for the diagnostic categories of the update Bethesda System for Reporting Thyroid Cytopathology (TBSRTC). This indolent entity must be has an encapsulated and noninvasive follicles with papillary-like nuclear features (NIFTP). Additionally a recent international multidisciplinary collaborative group agreed about this variant. Finally, this new entity was agreed by American Thyroid Association in their treatment recommendations [4, 5, 6, 7, 8, 9, 10, 11]. By new nomenclature of NIFTP, the term thyroid carcinoma is avoided so, over-diagnosis and overtreatment of tumors with indolent biological behavior and a good prognosis will become clear and carries an excellent congratulation for patients [5].
Cytologically, the NIFTP can be related to any one of the six categories of TBSRTC; however, the majority fall into one of the following categories: 1) atypia of undetermined significance/follicular lesion of undetermined significance (AUS or category III); 2) suspicious for follicular neoplasm/ follicular neoplasm (SFN or category IV); and 3) suspicious for malignancy (SM or category V) [12, 13].
Many researchers mentioned downgrading of NIFTP in the “not malignant “category of TBSRTC has an impact mainly on the indeterminate categories (category III-IV-V), where the risk is expected to be reduced, while the benign (II) and the malignant categories (VI) are less affected [14]. Additionally, update study by Bongiovanni M found the risk of malignancy (ROM) reduced by 7%, 15%, and 2% in relation to the indeterminate category III, IV and V. A study by Nikiforov Y.E reported that NIFTP reduced the risk of malignancy for the TBSRTC diagnostic categories V and VI by 14 and 3% [15, 16].
The accurate diagnosis of NIFTP is tightly linked to histological sections following tumor resection. The diagnostic criteria included a unique features of this new entity was applied on this article [4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18]. In the same manner a combination of triple ways included sonographical, cytologic and molecular tests can be suspecting preoperative diagnosis of NIFTP [19, 20, 21, 22, 23] (Tables 1 & 2); (Figures 1-3) [24, 4, 5, 17, 18, 25].
| Clinical Examination Ultrasonography | Absence of clinically apparent or known metastasis of thyroid origin• |
|---|---|
| Absence of LNM• | |
| Fine-Needle Aspiration | Nodule without the following findings: extrathyroidal extension, microcalcification, taller-than-wide shape, spiculate/microlobulate/ill-defined margin, high suspicion of malignancy Category Ill, IV or V cytology of the Bethesda system |
| Nodule without mutations or with RAS or other RAS-like mutations (e.g., PAX81PPARG rearrangement)’ |
Table 1: Summarized data raised the possibility of thyroid nodule as corresponding to NIFTP [23].
| Tumor (STNs) | Architectures | Psammoma bodies / Necrosis | Papillae / High mitosis | Nuclei |
|---|---|---|---|---|
| Completely encapsulated. Evident interface between tumor and capsule with expansive growth. No vascular or capsular invasion throughout the whole capsule examination. | Micro-follicular Ma- follicular Or mixed follicles | Absent | Absent | Features of PTC. |
Table 2: Recommended diagnostic parameters in relation to NIFTP [4,6,18,17].
![Figure 1: Classification of follicular-patterned thyroid tumors with papillary-like nuclear feature. FVPTC, follicular variant of papillary thyroid carcinoma; iEFVPTC, invasive encapsulated follicular variant of papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary–like nuclear features) [24].](/fulltextimages/9994/fig_1.png)
![Figure 2: A) Margins of the nodule: a NIFTP has definite, expansive margins, usually encircled by a continuous, intact capsule (left). If capsular or vascular invasions are present (middle), or if the capsule is discontinuous or completely absent and the nodule has infiltrative margins towards the surrounding parenchyma (right), then the lesion cannot be diagnosed as NIFTP. B) Architecture of the nodule: a NIFTP as a prevalent microfollicular pattern of growth (up) and no papillae or psammoma bodies are allowed (down). C) Nuclear features: NIFTP have large, clear and irregular nuclei, with frequent grooves and occasional pseudoinclusions. NIFTP nuclei (right) differ significantly from regular nuclei of normal thyrocytes (left), which are small, rounded and dark [10].](/fulltextimages/9994/fig_2.png)
Figure 2: A) Margins of the nodule: a NIFTP has definite, expansive margins, usually encircled by a continuous, intact capsule (left). If capsular or vascular invasions are present (middle), or if the capsule is discontinuous or completely absent and the nodule has infiltrative margins towards the surrounding parenchyma (right), then the lesion cannot be diagnosed as NIFTP. B) Architecture of the nodule: a NIFTP as a prevalent microfollicular pattern of growth (up) and no papillae or psammoma bodies are allowed (down). C) Nuclear features: NIFTP have large, clear and irregular nuclei, with frequent grooves and occasional pseudoinclusions. NIFTP nuclei (right) differ significantly from regular nuclei of normal thyrocytes (left), which are small, rounded and dark [10].
![Figure 3: Summary of histological and cytological features of NIFTP. The figure summarizes the histological (left) and cytological (right) diagnostic features of NIFTP [10].](/fulltextimages/9994/fig_3.png)
Materials and Methods
All the prepared slides were stained with Hematoxylin and Eosin (H&E). The remaining materials used for preparation of paraffin-embedded tissue blocks. Sections with 3 micron thickness were prepared and stained with (H&E). Cytologically, all the cases were reported and categorized according to the update TBSRTC “2017” by 2 experienced pathologists [26] (Table 3). The smears were considered adequate if there are at least five groups of well visualized- follicular cells, each group containing ten or more cells in association with adequate colloid materials [26, 27, 28] so, any inadequate case was not considered as a target and excluded from this study. Cytologically, and according to TBSRTC, this article focused on the categories 3 to 5 “C3, C4 &C5 only” which were considered as an indeterminate lesion and suspicious for malignancy. These cases were considered as positive on cytological examination. All the above categories underwent for surgical intervention ranged from lobectomyto near total thyroidectomy. All the received tissue materials were examined grossly and processed according to standard guidelines and reported by consultant histopathologist. The sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy of FNAC, relative to the final histopathological findings were statistically analyzed using standardized formulas and through SPSS software [19].
During 5-years duration from January; 2017 to January 2022, 150 patients were selecting to participate among this article, all the cases seen in the surgery outpatient clinics; Northern zone’s Hospitals, KSA. The main complain among them is neck swelling. The patients were examined and evaluated clinically and laboratory investigations for T3, T4, and TSH in association with other routine investigations. A strict inclusion criteria is applied among the cases that is stressed on solitary thyroid nodule (STNs) with hypothyroid or euthyroid patients, whereas the exclusion criteria included patients with multiple thyroid nodules as well as abnormal hyperthyroid function tests. A pre-FNAC informed consent was taken from all selected included cases according to an institutional policy and procedure, then all were underwent for thyroid ultrasonography for nodule localization using a high resolution linear array transducer. A 20-24 gauge needle was used for the procedure and at least 2 passes of FNAC was done. The obtained aspirated materials were immediately smeared in labeled slides with the cytology numbers according to the laboratory’s policy and procedure, then placed in Cablin jars with 95% alcohol for fixations (wet preparations), and sent for preparation of staining.
| Diagnostic category | ROM if NIFTP ≠ CA (%) | ROM if NIFTP = CA (%) | Usual management |
|---|---|---|---|
| 1- Nondiagnostic or unsatisfactory (ND/UNS) | 5–10 | 5–10 | Repeat FNA with ultrasound guidance. |
| 2- Benign | 0-3 | 0-3 | Clinical and sonographic follow-up |
| 3- Atypia of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) | 6–18 | ∼10–30 | Repeat FNA, molecular testing, or lobectomy |
| 4- Follicular neoplasm or suspicious for follicular neoplasm (FN/SFN). | 10–40 | 25–40 | Molecular testing |
| Lobectomy | |||
| 5- Suspicious for malignancy (SFM) | 45–60 | 50–75 | Near-total thyroidectomy or surgical lobectomy |
| 6- Malignant | 94–96 | 97–99 | Near-total thyroidectomy or surgical lobectomy |
Table 3: Update TBSRTC including recommended diagnostic categories, implied risk of malignancy, and recommended management Cibas
Results
Clinical Background of NIFTP Studied Cases
As said up we enrolled 150 patients of selected STNs, the diagnosis of NIFTP is chiefly based on recent diagnostic parameters in relation to this new entity (Figures 1-3) (Table 1). Our patients were comprised of 50 cases (33.3%) men and 100 cases (66.7%) women that were included in this study. The female/male (M/f) ratio was 2:1. The patients’ age ranged from 20-70 year, with an average age of 50 (Table 4). Majority of patients were in the age group 31-40 years. Majority of patients were suffering from neck swelling whereas; dysphagia and hoarseness were rare. In regard to the ultrasonographical findings, majority of cases were seen as TRIADs 4 which is suspicious whereas; minority of them was TRIADs 3 which is considered benign (Table 5).
| Age groups | # of cases | Gender | Bethesda Category Type | Frequency | % of categories | |
|---|---|---|---|---|---|---|
| Men | Women | |||||
| 20-30 | 30 | 10 | 20 | C3 | 18 | 12% |
| 31-40 | 53 | 17 | 36 | C4 | 80 | 53.30% |
| 41-50 | 45 | 15 | 27 | C5 | 52 | 34.70% |
| 51-60 | 15 | 5 | 10 | |||
| 61-70 | 7 | 3 | 7 | |||
| Total | 150 | 50 | 103 | 150 | 150 |
Table 4: Distribution of selected included cases according to the clinical variables and TBSRTC (C3-C5).
| Tumor size (cm) | Location / Lobe | Nodules (US) | Cervical LN status (US) | |
|---|---|---|---|---|
| TRIADS 3 | TRIADS 3 | |||
| 1-1.5 | LT Lobe. | 21 (14%) | 129 (86%) | Reactive |
| 1-2 | LT. Lobe | Reactive | ||
| 2-3 | LT. Lobe | Reactive | ||
| 2-4 | LT. Lobe | Suspicious | ||
| 2-5 | RT. Lobe. | Suspicious | ||
| 3-5 | RT. Lobe | Involved | ||
| 5-6 | LT. Lobe | Involved | ||
| 7 | LT. Lobe | Reactive | ||
| C3 AUS / FLUS | C4 FN /SLN | C5 Suspicious of malignancy | Total | |
| 18 | 80 | 52 | 150 |
Table 5: Ultrasongical Findings in relation to the selected included cases.
Cytological Background of Studied Cases
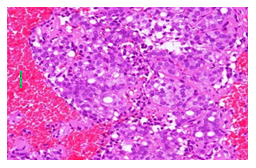
After FNAC done and the aspirates were examined, the results were categorized according to the update Bethesda system that were 18 (12%) cases were C3, 80 (53.3%) cases C4, and 52 (34.7%) cases were C4 (Table 6) (Figures 4-8). In regard to adequacy, any inadequate cases was excluded from this study so, all the 150 cases were FNAC adequate.
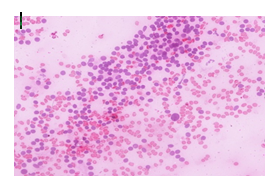
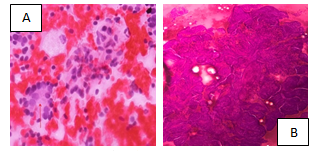
Figure 5a&b: CIV FNAC case showing microfollicles lined by enlarged cells H&E X200.
Surgical Background of Studied Cases
Lobectomy was done on 20 cases (13.3%) whereas; near total thyroidectomy performed on the remaining 130 cases (86.7%) (Table 7).
| Lobectomy | T. thyroidectomy | LN dissection | Total | |
|---|---|---|---|---|
| Not done | Done | |||
| 25 (16.7%) | 125 (83.3%) | 45 (30%) | 105 (70%) | 150 |
Table 6: Extent of surgery included lymph nodes in all studied cases.
Histopathological Background of NIFTP Studied Cases
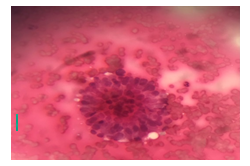
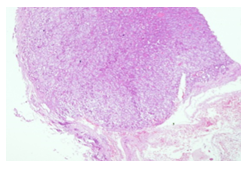
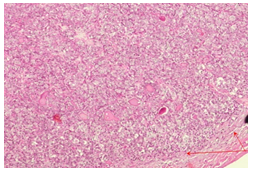
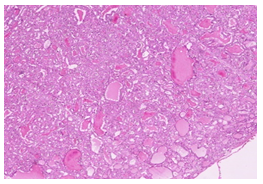
As stated before this new entity of thyroid tumors basically depended on histological examination of the excised tissue material. The histopathological findings of all the surgical received thyroid materials including the relative incidence of malignancy in each of Bethesda category were summarized in (Table 8). Majority of the surgically received thyroidectomies showing complete encapsulation whereas disrupted capsule was observed in 10 cases (6.7%) as well as majority of cases revealing absence of any vascular invasion yet the tumor may be touching the capsule without evident capsular breaking or out extensions. In regard to the architectural pattern of growth micro-follicles where seen in majority of the selected STNs studied cases and mixed follicles were found in 30 cases (20%). All cases showing complete absence of papillae, psammoma bodies, necrosis and mitotic activity (Figures 9-13).
| En. | C / V In | Arch. | Pap. | Nuclei | Pb | No | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pr. | Ab | Pr. | Ab | Mic | Mar | Mx | Pr | Ab | Gr | CL | Inc | Mx | Sb | ||
| 145 | 5 | -- | 150 | 117 | 3 | 30 | --- | 150 | 90 | 20 | 30 | 150 | 10 | --- | 150 |
Table 7: Histopathological Diagnostic Features of all studied cases. En: Encapsulation; C/V In: Capsular/vascular invasion; Arch:
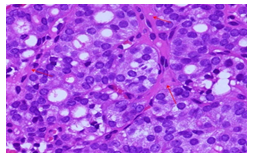
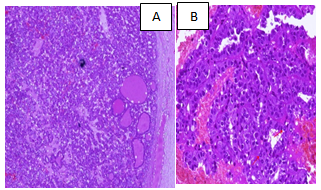
Figure 10 A and B: Mixed follicles with crowded cells, intact capsule and vessels H&E X100.
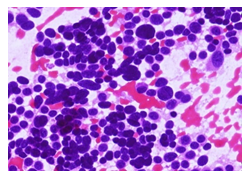
After carful histopathological examination and application of the update diagnostic features in relation to NIFTP of all the enrolled cases, follicular adenoma were seen in 8 cases (5.3%), follicular tumor of uncertain malignant potential (FT-UMP) found in 3 cases (2%) whereas, the remaining cases (92.7%) were noninvasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP) (Table 9) (Figures 14-17).
| Follicular adenoma | NIFTP | FT-UMP |
|---|---|---|
| 8 (5.3%) | 118 (92.7%) | 2 (2%) |
Table 8: Histopathological Diagnosis of all studied cases. NIFTP: Non-invasive follicular neoplasm with thyroid papillary like nu
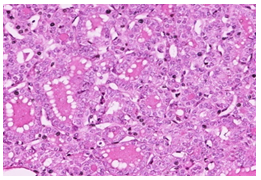
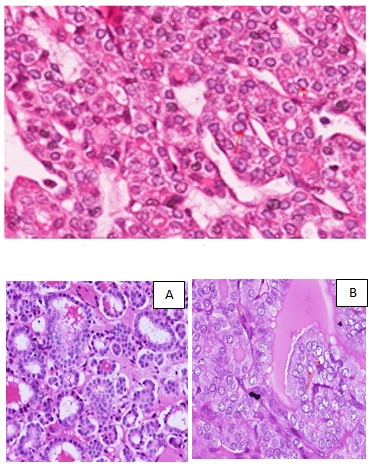
Figure 16 A&B: NIFTP with crowded enlarged cells H&E X400.
Discussion
The follicular variant of papillary thyroid carcinoma (FVPTC) is considering the second most common histological variant of PTC [30]. Before mentioning the entity NIFTP nomenclature, any encapsulated PTC with follicular pattern of growth and has the classic nuclear features and even without invasive features, was considered as malignant tumor with therapy may be as conventional PTC. Now as the nuclear features of PTC are subjective, the diagnostic probability of NIFTP that become resemble follicular adenoma / carcinoma group of tumors (RAS-like) is may be fare away the classic PTC group of tumors (BRAF-like) [5, 31]. Cytologically, the reports of FNAC aspirates of our cases were issued in accordance with the update Bethesda System 2017 [26]. This system provides a good channel for communication between surgeons and pathologists helping the former to choose appropriate therapeutic pathways. It makes the cytology report unambiguous, clear, succinct and clinically relevant. Each category of the TBSRTC has an implied risk of malignancy (ROM) which now is changeable and dependent on the mentioning of NIPTP as player factor in regard to the Bethesda system. The ROM is ranging from
5 to 10% for the CI category up to 96% for the C6 category [26, 27].
Cytological, among the included 150 cases of STNs in this study that were chosen as CIII, CIV, and CV. 18 (12%) cases were the first category, 80 (53.3%) were the second one whereas; the last C5 cases were 52 (34.7%).In the same manner NIFTP cases can be considered in any categories of TBSRTC yet, it is considered in intermediate categories that are CIII, CIV, 1nd CV. In published series it is found among 29.8% of cases of CIII “atypia of undetermined significance/ follicular lesion of undetermined significance (AUS/FLUS)”, 28.0% of cases of CIV “follicular neoplasm (FN)” and 21.2% in cases of CV “suspicious for malignancy (SM)” [32, 33, 34] showed a similar NIFTP cases distribution in among all TBSRTC categories with 34.2% and 30% in CIII, 22.7% and 21% in CIV category and 22.4% and 24% in CV category. In addition to the above a study Strickland K C reported a study done on 164 patients with tumors exhibited papillary- like nuclear features criteria [35]. The FNAC results of the indeterminate categories were 26% for CIII, 20% for CIV, and 19% for CV. Our results are more or less concordance with these observations.
This article is focusing in two items first is the considered indertminate categories of the update TBSRTC CIII, CIV & CV and the second on the histopathological parameters for diagnosing NIFTP.
CIII category “Follicular Lesion of Undetermined Significance/ Atypia of Undetermined Significance (FLUS/AUS)”.
The 2017 TBSRTC FUS/AUS category with auditing and adding the new NIFTP, the ROM is higher than originally estimated one and become closer to 10–30% in consideration that NIFTP is a malignant one, in contrast to the risk of 6–18% if NIFTP is not considered as malignant [36, 37]. As mentioned above in this article 18% of cases (n. 18/150) encompassed CIII category.
CIV category “Follicular Neoplasm or Suspicious for a Follicular Neoplasm”.
The update TBSRTC mentioned a modification for the definition and diagnostic criteria for this category as if there is an increased nuclear size, nuclear contour irregularities, and/ or chromatin clearing without true papillae and intranuclear inclusions, the lesion can be classified as FN/SFN [8]. In our article and according to the update TBRST 2017, NIFTP is considered if the cytology material has predominance of microfollicles and focal or mild nuclear atypia. This is true yet the final diagnosis for NIFTP is accurately issued on the received tissue material. These opinions are concordance with other researchers [26, 27].
CV category “Suspicious for Malignancy”. The incidence of FINTP is raised in relation among FNAC cases of Bethesda category CV so; lobectomy is advised rather than total thyroidectomy [38]. In our study lobectomy was done on 20 cases (13.3%) whereas near total thyroidectomy performed on the remaining 130 cases (86.7%). Mainthia et al., reported a study done on 164 patientsthyroid lobectomy was done in 48% whereas; 52% patients were underwent total thyroidectomy.
Histologically and in concern with incidence of NIFTP it is varying in researches and ranges from 5% to 28% of all thyroid neoplasms after strict applications of its diagnostic parameters [39]. A reclassification of 71% of EFVPTC as NIFTP, the incidence of this entity is about 27% of all included PTC in the study Wong, et al. [40]. Another review linked to consensus diagnosis involving three pathologists, NIFTP observed in 46% of total 60 FVPTC [41]. Additionally, series [42] considered incidence of NIFTP is up to 40%. In the same theme another publication found only 15(13%) /110 of EFVPTC was NIFTP [43]. These results are more of less similar to our results. In the same histological background in regard NIFTP, this new entity must be differentiated histologically rather than cytologically from other thyroid neoplasms as follicular adenoma, EFVPTC, FT-UMP (follicular tumor of uncertain malignant potential), WDT- UMP (well-differentiated tumor with uncertain malignant potential) as well as recently introduced borderline tumor with papillary structure “NEPRAS,”. The above pitfalls can be solved by the application of the diagnostic parameters of NIFTP, the diagnosis will be straightforward [44, 10]. A study by Hirokawa and coworkers 2020 showed that in a Japanese retrospective case series, the peculiar differential diagnosis of NIFTP is follicular adenoma rather than other neoplasms [45]. Finally histological diagnosis of the new entity NIFTP is decreasing the ROMS in the intermediate categories [36, 46, 47, 48]. Researches mentioned reductions among the ROM by the following 8.2% (I2 was 43%) in AUS/FLUS, 8.2% (I2 was 53%) in FN, and 7.3% (I2 was 89%) in SM [49] Similarly, Layfield et al., showed significantly lower ROM in all TBSRTC categories except for the ND category [50]. Bongiovanni et al. showed a reduction in the ROM for CV “SM” category by 14% [51].
In this study the majority of patients were females (66.7%) as well as in their fourth decade of life. These findings are in agreement with a study by Ohba, et al. [52]. In the same theme all cases were selected as STNs that was similar to study by Hirokawa, et al. [53] mentioned STNs were 4–9 times more common in females as compared to males. In regard to gender, this study showed that solitary thyroid nodules and NIFTP cases were commonest in females than males, these observations little pit near to others [44, 45].
Acknowledgments
None
Conflict of interest
The authors declare no conflict of interest.
References
-
Asha S, Dixit D, Shirol VS, Bhimalli S (2013) Study of absence of isthmus of thyroid gland with its developmental and surgical implications in adult human cadavers: a case series. Med Innov 2(1): 50-52.
-
Reddy CK, Panchakshari M (2016) A study of anatomical and morphological variations of the thyroid gland. Sch J Appl Med Sci 4(9): 3510-3513.
-
Ito Y, Hirokawa M, Hayashi T, Kihara M, Onoda N, et al. (2022) Clinical outcomes of follicular tumor of uncertain malignant potential of the thyroid: real-world data. Endocrine Journal advance publication 69(7): 757-761.
-
Lloyd RV, Osamura RY, Klooppel G, Rosai J (2017) WHO classification of tumors of endocrine organs. 4th (Edn.), International Agency for Research on Cancer (IARC), Lyon, France.
-
Nikiforov YE, Seethala RR, Tallini G, Baloch ZW, Basolo F, et al. (2016) Nomenclature revision for encapsulated follicular variant of papillary thyroid carcinoma: a paradigm shift to reduce overtreatment of indolent tumors. JAMA Oncol 2(8): 1023-1029.
-
Bizzarro T, Martini M, Capodimonti S traccia P, Lombardi CP, et al. (2016) The morphologic analysis of non- invasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP) on liquid based cytology: Some insights of their identification. Cancer Cytopathol 124(10): 699-710.
-
Ibrahim A, Fortune KAL, Wu H (2016) Fine needle aspiration cytology of noninvasive follicular thyroid neoplasm with papillary like nuclear features (NIFT), single institutional study with comparison to invasive follicular variant of papillary thyroid carcinoma. Mod Pathol 29: 86-125.
-
Pusztaszeri M, Triponez F, Meyer P, Sadowski SM (2017) Non Invasive follicular thyroid neoplasm with papillary like nuclear features (NIFTP): report of an institutional experience with 86 cases. J Basic Clin Med 6(1): 29-35.
-
Zhao L, Santagata DD, Sadow PM, Faquin WC (2017) Cytological, molecular, and clinical features of noninvasive follicular thyroid neoplasm with papillary-like nuclear features versus invasive forms of follicular variant of papillary thyroid carcinoma. Cancer Cytopathol 125(5): 323-331.
-
Maletta F, Falco EC, Gambella A, Metovic J, Papotti M (2020) Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features: From Echography to Genetic Profile. Tohoku J Exp Med 252(3): 209-218.
-
Haugen BR, Sawka AM, Alexander EK, Bible KC, Caturegli P, et al. (2017) American Thyroid Association Guidelines on the Management of Thyroid Nodules and Differentiated Thyroid Cancer Task Force Review and Recommendation on the Proposed Renaming of Encapsulated Follicular Variant Papillary Thyroid Carcinoma Without Invasion to Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features. Thyroid 27(4): 481-483.
-
Maletta F, Massa F, Torregrossa L, Duregon E, Casadei GP, et al. (2016) Cytological features of noninvasive follicular thyroid neoplasm with papillary-like nuclear features and their correlation with tumor histology. Hum Pathol 54: 134-142.
-
Maletta F, Volante M, Papotti M (2017) Experience on NIFTP cytology, with a mini meta-analysis of the literature. J Basic Clin Med 6(1): 44-50.
-
Linhares SM, Whitfield BW, Lee AF, Gordillo D, Picado O, et al. (2020) Impact of noninvasive follicular thyroid neoplasm with papillary-like nuclear features on revised bethesda system malignancy rates at a single institution. J Surg Res 255: 152-157.
-
Bongiovanni M, Faquin WC, Giovanella L, Durante C, Kopp P, et al. (2019) Impact of non-invasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP) on risk of malignancy in patients undergoing lobectomy/thyroidectomy for suspected malignancy or malignant fine-needle aspiration cytology findings: a systematic review and meta-analysis. Eur J Endocrinol 181(4): 389-396.
-
Nikiforov YE, Baloch ZW, Hodak SP, Giordano TJ, Lloyd RV, et al. (2018) Change in diagnostic criteria for noninvasive follicular thyroid neoplasm with papillary like nuclear features. JAMA Oncol 4(8): 1125-1126.
-
Seethala RR, Baloch ZW, Barletta JA, Khanafshar, Mete O, et al. (2018) Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a review for pathologists. Mod Pathol 31(1): 39-55.
-
Hahn SY, Shin JH, Oh YL, Kim TH, Lim Y, et al. (2017) Role of ultrasound in predicting tumor invasiveness in follicular variant of papillary thyroid carcinoma. Thyroid 27(9): 1177-1184.
-
Yang GCH, Fried KO, Scognamiglio T (2017) Sonographic and cytologic differences of NIFTP from infiltrative or invasive encapsulated follicular variant of papillary thyroid carcinoma: a review of 179 cases. Diagnostic Cytopathology 45(6): 533-541.
-
Rosario PW (2017) Ultrasonography and cytology as predictors of noninvasive follicular thyroid (NIFTP) neoplasm with papillary-like nuclear features: importance of the differential diagnosis with the invasive encapsulated follicular variant of papillary thyroid cancer. Clinical Endocrinology 87(5): 635-636.
-
Bongiovanni M, Giovanella L, Romanelli F, Trimboli P (2018) Cytological diagnoses associated with non- invasive follicular thyroid neoplasms with papillary-like nuclear features, (NIFTP) according to the Bethesda system for reporting thyroid cytopathology: a systematic review and meta-analysis. Thyroid,; 29(2): 222-228.
-
Nikiforov YE (2017) Role of molecular markers in thyroid nodule management: then and now. Endocrine Practice 23(8): 979-988.
-
Rosario PW, Mourao GF (2019) Follow-up of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP). Head and Neck 41(3): 833-834.
-
Kholova I, Haaga E, Ludvik J, Kalfert D, Ludvikova M (2022) Noninvasive Follicular Thyroid Neoplasm with Papillary-like Nuclear Features (NIFTP): Tumor Entity with a Short History. A Review on Challenges in Our Microscopes, Molecular and Ultrasonographic Profile. Diagnostics 12(2): 250.
-
Cibas ES, Ali ZS (2017) The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 27(11): 1341-1346.
-
Ali Syed Z, Cibas ES (2010) The Bethesda system for reporting thyroid cytopathology. In: Ali Syed Z , et al. (Eds.), Springer, pp: 11.
-
Hennawy H, Zaid H, Mujeeb I, Kahlout E, Bedai ESM (2013) Accuracy of Fine Needle Aspiration Cytology of Solitary Thyroid Nodules in Tertiary versus Community Hospital Surg Sci 4: 494-499.
-
Bagga PK, Mahajan NC (2010) Fine needle aspiration cytology of thyroid swellings: How useful and accurate is it? Indian J Cancer 47(4): 437-442.
-
Yu XM, Schneider DF, Leverson G, Chen H, Sippel RS (2013) Follicular variant of papillary thyroid carcinoma is a unique clinical entity: a population-based study of 10,740 cases. Thyroid 23(10): 1263-1268.
-
Tallini G, Tuttle RM, Ghossein RA (2017) The History of the Follicular Variant of Papillary Thyroid Carcinoma. J Clin Endocrinol Metab 102(1): 15-22.
-
Haaga E, Kalfert D, Ludvikova M, Kholova I (2022) Non- Invasive Follicular Thyroid Neoplasm with Papillary- Like Nuclear Features Is Not a Cytological Diagnosis, but It Influences Cytological Diagnosis Outcomes: A Systematic Review and Meta-Analysis. ActaCytol 66(2): 85-105.
-
Ruanpeng D, Cheungpasitporn W, Thongprayoon C, Hennessey JV, Shrestha RT (2019) Systematic Review and Meta-analysis of the Impact of Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features (NIFTP) on Cytological Diagnosis and Thyroid Cancer Prevalence. Endocr Pathol 30(3): 189-200.
-
Bongiovanni M, Giovanella L, Romanelli F, Trimboli P (2019) Cytological Diagnoses Associated with Noninvasive Follicular Thyroid Neoplasms with Papillary-Like Nuclear Features According to the Bethesda System for Reporting Thyroid Cytopathology: A Systematic Review and Meta-Analysis. Thyroid 29(2): 222-228.
-
Mainthia R, Wachtel H, Chen Y, Mort E, Parangi S, Sadow PM, et al. (2018) Evaluating the projected surgical impact of reclassifying noninvasive encapsulated follicular variant of papillary thyroid cancer as noninvasive follicular thyroid neoplasm with papillary- like nuclear features. Surgery 163(1): 60-65.
-
Strickland K C, Brooke E H, Ellen M, Erik K A , Cibas ES, et al. (2015) The impact of noninvasive follicular variant of papillary thyroid carcinoma on rates of malignancy for fine-needle aspiration diagnostic categories. Thyroid 25(9): 987-992.
-
Faquin W C, Lawrence Q W, Amir H A, Syed Z Ali, Bishop JA, et al. (2016) Impact of reclassifying noninvasive follicular variant of papillary thyroid carcinoma on the risk of malignancy in The Bethesda System for Reporting Thyroid Cytopathology. Cancer Cytopathol 124(3): 181- 187.
-
Pusztaszeri M, Diana Rossi E, Auger M, Baloch Z, Bishop J, et al. (2016) The Bethesda system for reporting thyroid cytopathology: proposed modifications and updates for the second edition from an international panel. Acta Cytologica 60(5): 399-405.
-
Krane Jeffrey F, Alexander EK, Cibas ES, Barletta JA (2016) Coming to terms with NIFTP: a provisional approach for cytologists. Cancer Cytopathol 124(11): 767-772.
-
Bychkov A, Jung CK, Liu Z, Kakudo K (2018) Noninvasive Follicular Thyroid Neoplasm with Papillary Like Nuclear Features in Asian Practice: Perspectives for Surgical Pathology and Cytopathology. Endocr Pathol 29 (3): 276-288.
-
Wong KS, Strickland KC, Angell TE, Nehs MA, Alexander EK, et al. (2017) The Flip Side of NIFTP: an Increase in Rates of Unfavorable Histologic Parameters in the Remainder of Papillary Thyroid Carcinomas. Endocr Pathol 28(2): 171-176.
-
Kiernan CM, Weiss VL, Mehrad M, Ely K, Baregamian N, et al. (2018) New terminologynoninvasive follicular neoplasm with papillary-like nuclear features (NIFTP) and its effect on the rate of malignancy at a single institution. Surgery 163(1): 55-59.
-
Agrawal N, Abbott CE, Liu C, Kang S, Tipton L, et al. (2017) Non-invasive follicular tumor with papillary-like nuclear features: not a tempest in a teapot. Endocr Pract 23(4): 451-457.
-
Chung R, Guan H, Ponchiardi C, Cerda S, Marwaha N, et al. (2021) Non-invasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features: Epidemiology and Long-Term Outcomes in a Strictly Defined Cohort. Thyroid 31(1): 68-75.
-
Faquin WC, Wong LQ, Afrogheh AH, Ali SZ, Bishop JA, et al. (2016) Impact of reclassifying noninvasive follicular variant of papillary thyroid carcinoma on the risk of malignancy in The Bethesda System for Reporting Thyroid Cytopathology. Cancer Cytopathol 124(3): 181- 187.
-
Shrestha RT, Ruanpeng D, Hennessey JV (2019) Cytomorphology of Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features and the Impact of New Nomenclature on Molecular Testing. Med Sci 7(2): 15.
-
Baloch ZW, Seethala RR, Faquin WC, Papotti, MG, Basolo F, et al. (2016) Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP): A changing paradigm in thyroid surgical pathology and implications for thyroid cytopathology. Cancer Cytopathol 124(9): 616-620.
-
Lau RP, Paulsen JD, Brandler TC, Liu CZ, Simsir A, et al. (2017) Impact of the Reclassification of “Noninvasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma” to “Noninvasive Follicular Thyroid Neoplasm with Papillary-Like Nuclear Features” on the Bethesda System for Reporting Thyroid Cytopathology: A Large Academic Institution’s Experience. Am J Clin Pathol 149(1): 50-54.
-
Layfield LJ, Baloch ZW, Esebua M, Kannuswamy R, Schmidt RL (2017) Impact of the Reclassification of the Non-Invasive Follicular Variant of Papillary Carcinoma as Benign on the Malignancy Risk of the Bethesda System for Reporting Thyroid Cytopathology: A Meta-Analysis Study. Acta Cytol 61(3): 187-193.
-
Bongiovanni M, Faquin WC, Giovanella L, Durante C, Kopp P, et al. (2019) Impact of non-invasive follicular thyroid neoplasms with papillary-like nuclear features (NIFTP) on risk of malignancy in patients undergoing lobectomy/thyroidectomy for suspected malignancy or malignant fine-needle aspiration cytology findings: A systematic review and meta-analysis. Eur J Endocrinol 181(4): 389-396.
-
Dorairajan N, Jayashree N (1996) Solitary nodule of the thyroid and the role of fine needle aspiration cytology in diagnosis. J Indian Med Assoc 94(2): 50-52, 61.
-
Bouvet M, Feldman JI, Gill GN, Dillmann WH, Nahum AM, et al. (1992) Surgical management of the thyroid nodule: patient selection based on the results of fine‐needle aspiration cytology. Laryngoscope 102(12): 1353-1356.
-
Ohba K, Mitsutake N, Matsuse M, Rogounovitch T, Nishino N, et al. (2019) Encapsulated papillary thyroid tumor with delicate nuclear changes and a kras mutation as a possible novel subtype of borderline tumor. J Pathol Transl Med 53(2): 136-141.
-
Hirokawa M, Higuchi M, Suzuki A, Hayashi T, Kuma S, et al. (2020) Prevalence and diagnostic significance of noninvasive follicular thyroid neoplasm with papillary- like nuclear features among tumors previously diagnosed as follicular adenoma: a single-institutional study in Japan. Endocr J 67(10): 1071-1075.
- Huddled and Preternatural- Atypical Lobular Hyperplasia
- Cytologic Surveillance Versus Immediate Referral to Colposcopy for Women with a Cervical Cytology Diagnosis of ASC-US and LSIL in the Absence of HPV DNA Test
- Callow and Vernal-Hepatoblastoma
- Black Plum Fruit Extract as a Substitute for Haematoxylin in Haematoxylin and Eosin Staining Technique
- Critical Analysis of World Status of Research on the Development of High Yielding Strains of Jatropha Curcas L
- Melissopalynology in Some Regions of Kermanshah Province (West of Iran)