Immunohistological Spectrum of Diffuse Crescentic Glomerlonephritis, a Single Center Study in Bangladesh
Background: Diffuse Crescentic glomerulonephritis (CrGN) is defined as presence of crescents in >50% of glomeruli sampled for renal biopsy. This is a critical diagnosis with clinical implications that ideally is communicated to the referring physician immediately. There is limited data on the etiology, clinical and histopathological spectrum of CrGN in Bangladeshi population. Aim: This study aims to identify the aetiology, clinico-pathological features and immunohistological patterns of crescentic glomerulonephritis in Bangladeshi population. Materials and Methods: All the crescentic glomerulonephritis diagnosed histologically at Armed Forces Institute of Pathology, Dhaka irrespective of age and sex are included in the study. The study duration was from January 2017 to December 2018. The renal biopsy samples were undergone H&E, PAS, Masson trichrome and Methanamine silver staining. For each case direct immunofluoresnece study was carried out for IgG, IgM, IgA, C3, C1q, Kappa and Lambda. Depending on clinical, biochemical, serological, histological and immunofluorescence evaluation crescentic glomerulonephritis was classified. Results: During stipulated period 43 crescentic glomerulonephritis were diagnosed which comprises 3.5% out of total 1229 non transplant renal core biopsy patients. Mean age was 30.32+ 17.41 the largest age group (15/43) being paediatric age group (<16 yrs). The male female ratio was 0.72. The most common presentation was generalized body swelling (46.51%) followed by gross haematuria (27.9%). On urine examination 38 (88.37%) patients had haematuria and 28 (65.12%), patients had massive proteinuria (>3.0 Gm/24 hrs). The mean serum creatinine level was 5.9±4.47 mg/dl (1.3 to 18.85 mg/dl). ANA was positive in 5 cases and among those 04 were anti dsDNA positive and labeled as systemic lupus erythematosus (SLE). Among all immune complex mediated crescentic glomerulonephritis (IC-CGN) was 22 (51.16%), Pauci-immune crescentic glomerulonephritis (PI-CGN) was 17 (39.53%), anti-glomerular basement membrane disease (anti GBM disease) was 03 (6.97%) and 01(4%) could not be classified due to lack of DIF findings. Average age of IC-CrGN is 27.86 yrs, PI-CrGN is 31.29 yrs and anti GBM disease is 36.67 yrs. Serum creatinine level during admission was in average, 4.10 mg/dl in IC-CrGN, 5.66 mg/dl in PI-CrGN and 11.46 mg/dl in anti GBM disease. Among the PI-CGN, 9 (53%) were ANCA positive and 08 (47%) were ANCA negative. Among ANCA positive PI-CGN, one had associated ANA positivity. One IC-CrGN case found with associated with ANCA positivity. Among 22 IC-CGN, 05 (23%) were crescentic IgA, 04 (18%) were crescentic lupus nephritis, 04 (18%) were C3 glomerulopathy, 09 (41%) were post infectious glomerulonephritis with diffuse crescent formation. The glomerular crescents formation was (79.4%±14.13) in PI-CGN while it was (67.62%±13.98) among IC-CGN cases and (79.89%±17.7) in anti GBM glomerulonephritis. Among ICCGN, 7 (31.81%) cases needed dialysis on admission, while 9 (52.94%) PI-CGN cases and all (100%) anti GBM cases were managed during admission by dialysis. Conclusion: Diffuse CrGN is not very rare in our population which warrants early notification to the clinician for its aggressive prognostic significance. IC-CrGN accounts for commonest immunohistological pattern of CrGN in our cohort followed by PI-CrGN and anti GBM diseases.
Introduction
Diffuse crescentic glomerulonephritis (CrGN) is defined as presence of crescents in >50% of glomeruli sampled for renal biopsy. This is a critical diagnosis with clinical implications that ideally is communicated to the referring physician immediately [1]. Extracapillary proliferation within a glomerulus, either partially or completely filling up the Bowman’s space defines a crescent. It is composed of proliferating parietal epithelial cells, podocytes, macrophages, and fibroblasts [2]. The process is initiated by entry of fibrin and other proteins from glomerular capillaries rupturing the basement membrane [3].
Typically, a patient with CrGN presents with nephritic syndrome and rapid deterioration of renal function. This clinical syndrome is referred to as “rapidly progressive glomerulonephritis” (RPGN) or rapidly progressive renal failure and is often considered synonymous with histological evidence of CrGN [1]. Pathology and immunopathology of CrGN comprises three major categories, 1) Anti glomerular basement membrane disease (anti GBM disease), 2) Immune complex crescentic glomerulonephritis (IC-CrGN) and 3) Pauci- immune crescentic glomerulonephritis (PI-CrGN) [4]. Serological testing in a suspected case of RPGN includes screening for relevant antibodies including but limited to anti-GBM, ANCA and anti-DNA antibodies [5].
There is limited data on the etiology, clinical and histopathological spectrum of CrGN in Bangladeshi population. This study aims to identify the aetiology, clinico-pathological features and immunohistological patterns of CrGN in Bangladeshi population.
Materials and Methods
A retrospective descriptive study is carried out at Armed Forces Institute of Pathology, Dhaka, Bangladesh, with the histopathologically diagnosed cases of diffuse CrGN during the period from January 2017 to December 2018. Diffuse CrGN is defined as presence of proliferation of parietal cells forming two or more cell layers filling the bowman’s space in more than 50% glomeruli in the renal biopsy. Detailed clinical and biochemical evaluation was done for these patients. Clinical details included age, gender, presenting complaints, presence of hypertension. Biochemical parameters, including serum creatinine at diagnosis, urine routine examination, including 24-hour urinary protein level were recorded from hospital record sheet. Serological investigations for anti-nuclear antibody (ANA), anti-double stranded DNA (dsDNA), anti- neutrophil cytoplasmic antibody (ANCA) and serum complement levels (C3 &C4) were also recorded.
Histopathological Examination
The renal biopsy samples were undergone H&E, PAS, Masson trichrome and Methanamine silver staining. Histologically all the three components were observed including glomeruli, tubules and interstitium. Biopsies carrying at least 5 glomeruli excluding obsolete glomeruli were considered as adequate. Crescents present in >50% glomeruli excluding the obsolete glomeruli were included in the study. The crescents were categorized into cellular and fibrocellular/fibrous. For each case direct immunofluoresnece study was carried out for IgG, IgM, IgA, C3, C1q, Kappa and Lambda. The immune complex- mediated GN (IC-CrGN) refers to the presence of immune complex deposits in the glomeruli visible by immunofluorescence study (granular deposits). Pauci- immune GN (PI-CrGN) has relative absence of deposits visible by IF. Anti-GBM disease is characterized by linear immunoglobulin (Ig) G staining along glomerular basement membrane. Anti GBM disease is further confirmed by detection of serum anti GBM antibody.
Statistical Method
The study being descriptive in nature, frequencies were calculated and no other statistical methods were employed.
Results
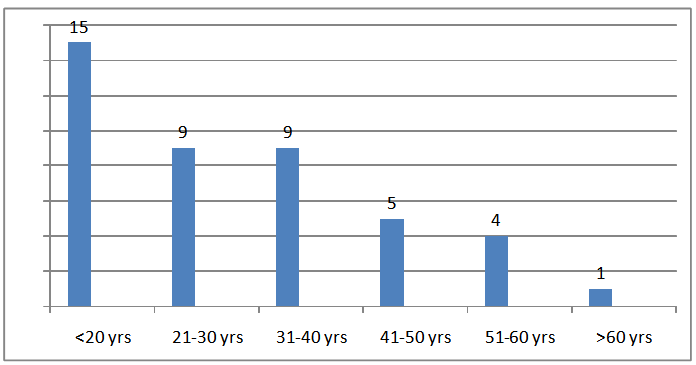
During stipulated period 43 CrGN were diagnosed which comprises 3.5% out of total 1229 non transplant renal core biopsy patients. Mean age was 30.32 the largest age group (15/43) being paediatric age group (<16 yrs). The male female ratio was 0.72 (Figure 1).
27.9%). On urine examination 38 (88.37%) patients had haematuria and 28 (65.12%), patients had massive proteinuria (>3.0 Gm/24 hrs). The mean serum creatinine level was 5.9 mg/dl (range 1.3 to 18.85 mg/dl) (Table 1). Serum C3 & C4 level was found low in 11/38 and 4/27 cases respectively. ANA was positive in 5 cases and among those 04 were anti dsDNA positive and labeled as systemic lupus erythematosus (SLE). ANCA was positive in 10 cases, negative in 24 cases and was unknown in rest 9 cases.
Characteristics Total (n=43) IC-CrGN (n=22) PI-CrGN (n=17) Anti GBM disease Table 1: Demographic and clinical characteristics of study population.
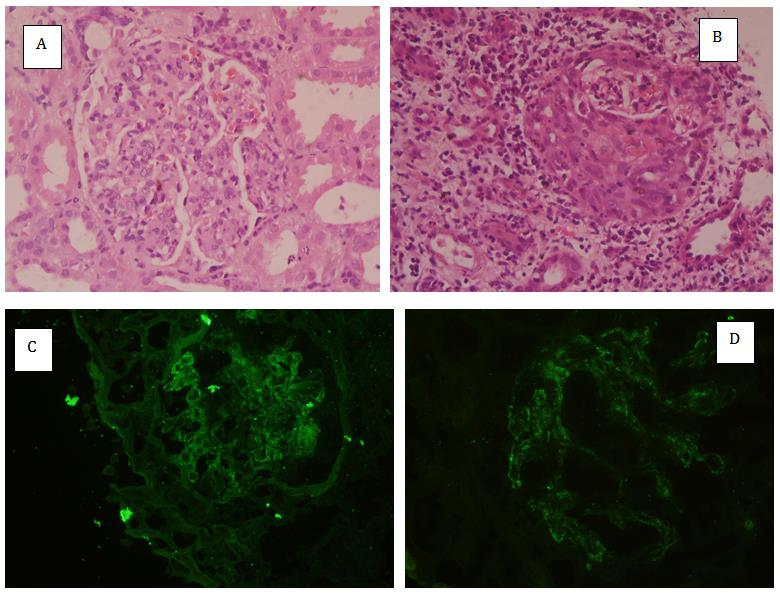
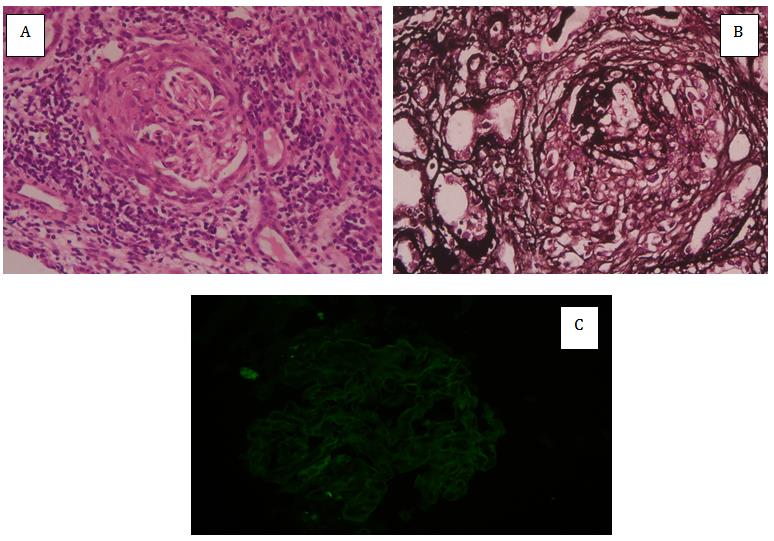
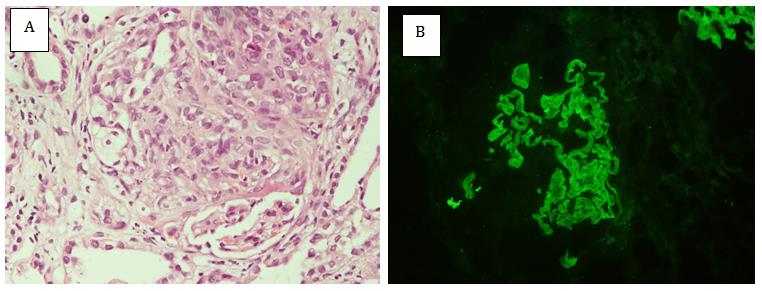
Among the study population IC-CrGN (Figure 2) was 22 (51.16%), PI-CrGN (Figure 3) was 17 (39.53%), anti GBM disease (Figure 4) was 03 (6.97%) and 01 (4%) could not be classified due to lack of DIF findings (Table 2). Among the PI-CGN, 9 (53%) were ANCA positive and 08 (47%) were ANCA negative. Among ANCA positive PI- CrGN one had associated ANA positivity. Among 22 IC- CGN, 05 (23%) were crescentic IgA, 04 (18%) were crescentic lupus nephritis, 04 (18%) were C3 glomerulopathy, 08 (36%) were post infectious glomerulonephritis with diffuse crescent formation. One IC-CrGN case found with associated with ANCA positivity. Mean age of IC-CrGN was 27.86 yrs, PI-CrGN was 31.29 yrs and anti GBM disease was 36.67 yrs. Serum creatinine level during admission was in average, 4.10 mg/dl in IC- CrGN, 5.66 mg/dl in PI-CrGN and 11.46 mg/dl in anti GBM disease. The proportion of glomerular crescent formation was 79.4% in PI-CrGN while it was 67.62% among IC- CrGN cases and 79.89% in anti GBM disease. Interstitial fibrosis and tubular atrophy (IFTA) was found >25% in 8 (36.36%) cases in IC-CrGN, 3 (17.65%) cases in PI-CrGN and 1 (33.33%) case in anti GBM diseases (Table 3). Among IC-CrGN, 7(31.81%) cases needed dialysis on admission, while 9 (52.94%) PI-CrGN cases and 100% anti GBM disease cases were managed during admission by dialysis.
| Immunohistological types | n =43 |
|---|---|
| Pauci-immune GN (PI-CrGN) | 17 (39.53) |
| ANCA positive | 9 |
| ANCA negative | 8 |
| Immune complex mediated GN (IC-CrGN) | 22 (51.16%) |
| Lupus nephritis | 4 |
| IgA nephropathy | 5 |
| C3 glomerulopathy | 4 |
| Post infectious GN | 9 |
| Anti GBM disease | 03 (6.98%) |
| Unclassifiable due to lack of DIF | 1 |
Table 1: Demographic and clinical characteristics of study population.
| Total (n=43) | IC-CrGN (n=22) | PI-CrGN (n=17) | Anti GBM disease (n=3) | Unclassified (n=1) | |
|---|---|---|---|---|---|
| Glomerulus (Nos) | 16±7 | 15±7 | 16±8 | 19±4 | 14 |
| Crescentic glomerulus | 11±5 | 10±4 | 13±7 | 16±5 | 8 |
| Crescent (%) | 73.05±14.8 | 67.62±13.98 | 79.4±14.13 | 79.89±17.7 | 57.14 |
| Endocapillary proliferation | 18 | 14 | 3 | 0 | 1 |
| Normal cellularity | 12 | 0 | 9 | 3 | 0 |
| IFTA (>25%) | 12 | 8 | 3 | 1 | 0 |
| ATI | 21 | 10 | 9 | 2 | 0 |
| Vasculitis | 9 | 2 | 4 | 3 | 0 |
Table 2: Immunohistologic categories of CrGN.
CrGN must be diagnosed promptly and precisely so that appropriate treatment can be initiated as quickly as possible. The best predictor of outcome for all types of CrGN is the severity of renal failure at the time therapy begins. Even several days’ delay in diagnosis and treatment can have a major negative impact on outcome because of the rapidly progressing loss of renal function that typically accompanies CrGN [1]. The incidence of CrGN varies with geographic location and policies of kidney biopsies from 2-10% in different studies [6]. In our study we got 3.5% diffuse CrGN which is closer to study of Nagaraju SP, et al. in Southern India population [7].
In our study the most common pattern of diffuse CrGN was IC-CrGN which accounts for 51.16%, followed by PI- CrGN (39.53%). Rampelli SK, et al. [8] in a recent study at South India (77.5%) and a study from China [9] have also got IC-CGN as the predominant cause of CrGN. While most of the studies from India and USA got PI-CrGN as the commonest pattern of CrGN (60-70%) [1, 10, 11]. Anti GBM diseases accounts for 6.97% of CrGN cases in our study, which is quite closer to study by McAdoo SP, et al. in London (5%) [12], Rampelli SK, et al. (2.5%) [8] and Kumar R, et al. (3%) [11] in India. While anti GBM diseases were found in higher number in study carried out by Nagaraju SP, et al. (24%) in India [7] and Jennette JC (15%) in USA [1]. It is possibly due to geographical, racial variation of study population and some of the studies were of small cohort.
In our study post infectious glomerulonephritis (36%) was the predominant cause of IC-CrGN followed by crescentic IgA nephropathy (23%), crescentic lupus nephritis (18%) and C3 glomerulopathy (18%). It is discordant with other studies like, Rampelli SK, et al. & Kumar R, et al. who got crescentic IgA as the predominant cause of IC-CrGN followed by post infectious The mean age of CrGN was 30.32+ 17.41 yrs in our study, however the largest age group was paediatric age (<16 Yrs) group (34.88%). Gupta R, et al. got closer mean age (27.6+17.1 yrs) with also the paediatric age group (<14 Yrs) as the predominant age group (26.8%) among over all CrGN cases [10]. Ravikumar G, et al. also got paediatric age group (<18 yrs) as the predominant age group (24%) for CrGN [13]. Male: female ration (0.72) of our study population was discordant with some studies, who got mostly male affected by CrGN [7, 16]. In our study female predominance is probably due the large number of IC-CrGN cases. Female predominance was also reported by Gupta R, et al. [10] and Jannette JC [1]. Among three immunohistological classes IC-CrGN patients (27.86 yrs) are comparatively younger and anti GBM disease patients (36.67 yrs) are older in comparison to PI-CrGN (31.29 yrs) in our study. Jannette JC [1] as well as Rampelli, SK et al. [8] also got IC-CrGN as the younger age group (Table 4).
In our study mean serum creatinine level on presentation was 5.9 mg/dl for all CrGN cases. Anti GBM diseases were presented with most severe renal impairment evidenced by very high (avg 11.46 mg/dl) serum creatinine level in comparison to IC-CrGN (avg 4.10 mg/dl) and PI-CrGN (avg 5.66 mg/dl). Choudhury TA, et al. got 5.54+3.66 mg/dl mean creatinine level in their study in North India [16]. Jannette JC also got highest level of serum creatinine on admission in anti GBM disease followed by PI-CrGN and IC-CrGN in University of North Carolina Nephropathology Laboratory similar to our
- study [1]. On histology, proportion of glomeruli displaying crescent was highest in anti GBM disease 79.89% followed by PI-CrGN 79.4% and IC-CrGN 67.62% in our study. Sinha A, et al. got proportion of glomeruli with
- Parameters
- Nagaraju SP, et al.
- Rampelli SK, et al.
- (n=29)
- (n=40)
- (n=43)
- Incidence
- 2.90%
- 5.80%
- 2.65%
- 3.50%
- Mean age
- 42.52+17.27
- 27.6+17.1
- 37.6+16.4
- 30.32+17.41
- M:F
- 1.23
- 0.9
- 0.65
- 0.72
- IC-CrGN
- 28%
- 77.50%
- 28.30%
- 62.70%
- 51.16%
- PI-CrGN
- 41%
- 20%
- 71.70%
- 25.80%
- 39.53%
- Anti GBM disease
- 24%
- 2.50%
- 0
- 11.60%
- 6.98%
Table 3: Comparison between different studies.
Conclusion
Diffuse CrGN is not very rare in our population which warrants early notification to the clinician for its aggressive prognostic significance. IC-CrGN accounts for commonest immunohistological pattern of CrGN in our cohort followed by PI-CrGN. There were also three cases of anti GBM diseases which were diagnosed on characteristic linear immune deposits of glomerular capillary wall which were authenticated by detection of anti GBM antibodies in serum.
This study was performed in the department of histopathology, Armed Forces Institute of Pathology, Dhaka. We acknowledge the support given by all the histo-technicians working in the department.
References
-
Jennette JC (2003) Rapidly progressive crescentic glomerulonephritis. Kidney Int 63(3): 1164-1177.
-
Thorner PS, Ho M, Eremina V, Sado Y, Quaggin S (2008) Podocytes contribute to the formation of glomerular crescents. J Am Soc Nephrol 19(3): 495- 502.
-
Sangle N (2018) Rapidly progressive (crescentic) glomerulonephritis. UM Medicine Pathology.
-
Couser WG (1988) Rapidly progressive glomerulonephritis: classification, pathogenetic mechanisms, and therapy. Am J Kidney Dis 11(6): 449-464.
-
Kambham N (2012) Crescentic Glomerulonephritis: an update on Pauci-immune and Anti-GBM diseases. Adv Anat Pathol 19(2): 111-124.
-
Andrassy K, Kuster S, Waldherr R, Ritz E (1991) Rapidly progressive glomerulonephritis: analysis of prevalence and clinical course. Nephron 59(2): 206- 212.
-
Nagaraju SP, Laxminarayana SLK, Kosuru S, Parthasarathy R, Attur RP, et al. (2017) Clinicopathological characteristics and outcomes of diffuse crescentic glomerulonephritis-a single center experience from Southern India. J Clin Diagn Res 11(9): 21-24.
-
Rampelli SK, Rajesh NG, Srinivas BH, Harichandra Kumar KT, Swaminathan RP, et al. (2016) Clinical spectrum and outcomes of crescentic glomerulonephritis: A single center experience. Indian J Nephrol 26(4): 252-256.
-
Tang Z, Wu Y, Wang Q, Zeng C, Yao X, et al. (2003) Clinical spectrum of diffuse crescentic glomerulonephritis in Chinese patients. Chin Med J (Engl) 116(11): 1737-1740.
-
Gupta R, Singh L, Sharma A, Bagga A, Agarwal SK, et al. (2011) Crescentic glomerulonephritis: a clinical and histomorphological analysis of 46 cases. Indian J Pathol Microbiol 54(3): 497-500.
-
Kumar R, Choudhary RK (2017) Study of etiology and clinical assessment of Crescentic glomerulonephritis. JMSCR 5(7): 25425-25429.
-
McAdoo SP, Tanna A, Randone O, Tam FW, Tarzi RM, et al. (2015) Necrotizing and crescentic glomerulonephritis presenting with preserved renal function in patients with underlying multisystem autoimmune disease: a retrospective case series. Rheumatology 54(6): 1025-1032.
-
Ravikumar G, Rout P (2017) Crescents in renal biopsies and crescentic glomerulonephritis-A 5 year study from South India. Trop J Path Micro 3(2): 174- 180.
-
Savage COS (2001) ANCA-associated renal vasculitis. Kidney Int 60(4): 1614-1627.
-
Dey B, Dange P, Ganesh RN, Parameswaran S, Pilai PPS (2017) Immune complex deposits in anti- neutrophil cytoplasmic antibody associated crescentic glomerulonephritis; a report of two cases. Immunopathol Persa 3(2): 09.
-
Choudhury TA, Singh RG, Usha, Singh S, Singh TB, et al. (2014) Clinicopathologic spectrum of crescentic glomerulonephritis: A hospital-based study. Saudi J Kidney Dis Transpl 25(3): 689-696.
-
Sinha A, Puri K, Hari P, Dinda AK, Bagga A (2013) Etiology and outcome of crescentic glomerulonephritis. Indian Paediatr 50(3): 283-288.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet