From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet
Background: Hallux valgus is a common deformity that causes pain over the medial prominence of the first metatarsal head and increases forefoot width, complicating shoe fitting. Although conservative measures like hygiene and footwear adjustments are considered, surgical treatment remains the primary option. Since Hueter's first surgery in 1871, over 150 techniques have been developed. Our study aims to evaluate the outcomes of the Schnepp technique in treating severe hallux valgus associated with a significant distal metatarsal articular angle (DMAA). Methods: A retrospective review was conducted on 32 patients (47 feet) treated for severe hallux valgus with elevated DMAA between April 2014 and June 2019, all of whom completed follow-up. The patients underwent Schnepp osteotomy (a distal medial closing osteotomy and a basal open wedge osteotomy) combined with soft tissue release. The cohort included 4 males (6 feet) and 28 females (41 feet), aged 22 to 56 years (mean 41.5 years). Preoperative evaluations showed an average Maryland metatarsophalangeal joint score of the American Orthopaedic Foot & Ankle Society (AOFAS) of 53.3 ± 6.7 and a Visual Analogue Scale (VAS) pain score of 6.0 ± 2.0. Outcomes were assessed by comparing preoperative and postoperative AOFAS and VAS scores, hallux valgus angle (HVA), first-second intermetatarsal angle (1-2IMA), DMAA, and first metatarsal length (FML). Results: All incisions healed primarily, and follow-up lasted 21 to 24 months, with an average of 22.7 months. Two feet experienced complications, including one case of hallux stiffness and necrosis of the first metatarsal head. One year postoperatively, the AOFAS score improved to 89.3 ± 6.4. Of the 47 feet, 38 were rated as excellent, 7 as good, and 2 as poor, yielding a 95.6% satisfaction rate. The VAS score significantly decreased to 1.6 ± 2.1. Radiographic reviews at three months confirmed complete bone healing at the osteotomy sites. At six months and one year postoperatively, significant improvements were observed in HVA, 1-2IMA, and DMAA compared to preoperative values. However, no statistically significant change in FML was noted one-year post-surgery. Conclusion: The Schnepp osteotomy is highly effective in improving clinical symptoms and radiographic parameters in patients with severe hallux valgus and elevated DMAA, with a low complication rate.
Abbreviations
DMAA: Distal Metatarsal Articular Angle; HVA: Hallux Valgus Angle; FML: First Metatarsal Length; VAS: Visual Analogue Scale; AOFAS: American Orthopaedic Foot & Ankle Society.
Introduction
Hallux valgus is a deformity of the first metatarsophalangeal joint, commonly characterized by lateral deviation of the great toe and medial displacement of the first metatarsal [1]. Severe hallux valgus is a three- dimensional, multi-planar deformity involving not only an abnormal hallux valgus angle (HVA) and first-second intermetatarsal angle (1-2 IMA) but often an increased distal metatarsal articular angle (DMAA). When associated with a significant DMAA, a single osteotomy technique may not always provide sufficient correction for such complex deformities [2].
Between April 2014 and June 2019, we performed Schnepp osteotomy, combining distal medial closing osteotomy and basal open wedge osteotomy of the first metatarsal, on 36 cases (56 feet) of severe hallux valgus with increased DMAA. Among these, 32 patients (47 feet) had complete follow-up data. This study retrospectively reviewed the clinical records of these 32 patients to evaluate the effectiveness of Schnepp osteotomy in correcting such deformities.
Material and Methods
This study was a retrospective review of a consecutive series of patients who underwent hallux valgus correction by a single foot surgeon, between April 2014 and June 2019. The procedure performed was the Schnepp osteotomy, which combines a distal medial closing osteotomy and a basal open wedge osteotomy of the first metatarsal.
Inclusion criteria for patients were severe hallux valgus (HVA > 30° or 1-2IMA > 15°) with an increased DMAA (DMAA ≥ 20°). Exclusion criteria included patients with degenerative arthritis of the first metatarsophalangeal joint, rheumatoid arthritis, diabetes, a history of forefoot surgery, or patients lost to follow-up.
Among the patients, 4 were male (6 feet) and 28 were female (41 feet), with ages ranging from 22 to 56 years (mean age: 41.5 years). The primary clinical symptoms included bunion formation and pain, which affected walking. No significant osteoarthritis was present in the first metatarsophalangeal joint on X-rays. Additionally, 9 feet presented with hammer toe deformity, and 8 feet showed plantar callus formation. Preoperatively, the average AOFAS score was 53.3 ± 6.7, and the Visual Analogue Scale (VAS) pain score was 6.0 ± 2.0.
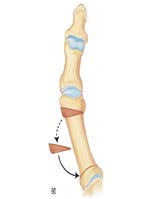
All patients provided consent to undergo the surgical procedure. Surgeries were performed using consistent operative techniques, including McBride’s procedure and lateral soft tissue release. A medial incision was made along the first metatarsophalangeal joint, extending from the proximal phalanx toward the first metatarsal. The medial bony prominence was removed, and the bunion excised. An adductor tendon and sesamoid ligament release were also performed. After completing the soft tissue procedures, the Schnepp osteotomy was carried out [3] (Figure 1): • Distal Medial Subtraction Osteotomy: A distal osteotomy was performed approximately 1 cm proximal to the articular surface of the first metatarsal head. The osteotomy was made perpendicular to the metatarsal axis, with a wedge-shaped cut on the distal side of the osteotomy line, about 5 mm from the osteotomy. The wedge was removed, and the osteotomy was compressed medially to close the wedge and correct the deformity.
• Proximal Open Wedge Osteotomy: A basal open wedge osteotomy was performed at the base of the first metatarsal. The distal fragment from the distal osteotomy was grafted into the proximal osteotomy, and fixation was achieved using Herbert screws.
After completing the osteotomies, absorbable sutures were used to pull the medial joint capsule dorsally and proximally, reducing the dislocated sesamoid bone and tightening the joint capsule. The incision was then closed routinely.
X-rays were taken four weeks postoperatively to confirm osteotomy healing, after which patients were allowed to bear weight in forefoot off-loading shoes. Clinical outcomes were assessed pre- and postoperatively using the AOFAS score [4] and VAS score.
All analyses were performed using SPSS version 21. Quantitative variables are presented as mean ± standard deviation. Pre- and postoperative comparisons were made using the paired Student’s t-test. A p-value of < 0.05 was considered statistically significant.
Weight-bearing X-rays of the feet in anteroposterior and lateral views were obtained to measure HVA, 1-2IMA, DMAA, and FML. • HVA: The angle between the axes of the metatarsal and proximal phalanx. • 1-2IMA: The angle between the axes of the first and second metatarsals. • DMAA: The angle between the axis of the first metatarsal and a line perpendicular to the distal articular surface. • FML: The distance from the intersection of the first metatarsal head with its axis to the intersection of the first metatarsal base with its axis.
Results
All surgical incisions healed without complications, and all patients were followed for 21 to 24 months, with an average follow-up period of 22.7 months. We have noted that two feet experienced postoperative complications: one case of hallux stiffness and one case of avascular necrosis of the first metatarsal head, which required secondary surgery for metatarsophalangeal joint fusion due to persistent pain.
At one year post-surgery, the average AOFAS score for the metatarsophalangeal joint was 89.3 ± 6.4 (p=0,017), demonstrating a statistically significant improvement compared to the preoperative score. Outcomes were excellent in 38 feet, good in 7, and poor in 2, yielding an overall satisfaction rate of 94.9%. The VAS score significantly decreased to 1.6 ± 2.1 (p=0,023).
Radiographic follow-up at 3 months confirmed complete bone union at the osteotomy sites. Comparisons of the hallux valgus angle (HVA), first-second intermetatarsal angle (1-2IMA), and distal metatarsal articular angle (DMAA) between the preoperative period and the 6-month and 2-year postoperative assessments revealed statistically significant improvements. No significant differences were noted between the 6-month and 1-year postoperative measurements. Additionally, there was no statistically significant change in first metatarsal length (FML) at 2 years post-surgery compared to preoperative measurements.
Radiographic results revealed significant improvements in various angles at 2 years follow up. The M1P1 angle decreased from a preoperative average of 29.8° to 7,6° (p=0,016), indicating marked correction in alignment.
Similarly, the M1M2 angle showed a reduction from 14.8° preoperatively to 11,2° at 2 years follow up (p=0,02), reflecting improvement in intermetatarsal alignment.
The DMAA angle, crucial for evaluating lateral deviation, improved substantially from a preoperative average of 25.8° to 8° at 2 years follow up (p=0,018). In addition, the DMAA2 angle shifted from 11° preoperatively to -5.6° (0,031), indicating correction in the distal metatarsal angle.
Lastly, the M1M5 angle decreased from an average of 34.2° preoperatively to 26.2° at 2 years follow up (p=0,035), reflecting improved balance across the forefoot. (Figure 2).
Discussion
Hallux valgus is a common deformity, especially in women, involving valgus deviation of the big toe and varus of the first metatarsal, creating excessive angulation of the first ray [5]. This deformity causes pain over the medial prominence of the first metatarsal head and increases forefoot width, complicating shoe fitting. Although conservative measures like hygiene and footwear adjustments are considered, surgical treatment remains primary. Since Hueter’s first surgery in 1871, over 150 techniques have emerged [6].
The first metatarsal osteotomy is key to correction, addressing metatarsus varus and potentially correcting length and DMAA. Schnepp’s bipolar osteotomy (distal subtraction, proximal addition) offers strong correction for moderate to severe cases, particularly when metatarsus varus and a high DMAA angle are involved.
The DMAA is primarily used to assess the degree of outward deviation of the first metatarsal head joint surface, with a normal value being less than 10° [7]. It is currently believed that DMAA reflects the alignment of the first metatarsophalangeal joint and is a critical factor in preventing recurrence of deformities after hallux valgus surgery [8].
This study presents the Schnepp technique, its advantages in hallux valgus treatment, two-year functional and radiological outcomes, and guidance for optimizing this osteotomy technique.
The distal subtraction osteotomy involves creating a wedge-shaped cut near the proximal part of the first metatarsal head joint surface while keeping the lateral cortex intact. The hallux is then realigned by closing the osteotomy site, correcting the DMAA and producing an inward tilt of the metatarsal head. Because the osteotomy is performed at the metaphyseal region of the first metatarsal, it promotes good bone healing [9].
A proximal opening wedge osteotomy, performed 1 cm distal to the tarsometatarsal joint, allows for effective correction of the metatarsus varus deformity. In our series, the two-plane osteotomy corrected both the DMAA and the 1-2 intermetatarsal angle (1-2IMA), while also allowing for slight lowering of the metatarsal head, reducing the occurrence of transfer metatarsalgia. Additionally, we replanted the wedge bone removed during the subtraction osteotomy into the proximal open wedge site, which helped preserve the first metatarsal length (FML) and further reduced the risk of transfer metatarsalgia (Figure 3).
Our functional results reveal a 95.6% satisfaction rate among patients. The AOFAS score, widely used for objective assessment, averaged 89.3 ± 6.4 postoperatively in our series, which is consistent with literature standards. Comparing functional outcomes across different techniques, particularly through AOFAS scores, our results with the Schnepp technique show superior outcomes for patients with significant metatarsus varus or DMAA.
Radiologically, the preoperative M1P1 angle in our study averaged 29.8°, achieving a postoperative average of 7.6°, with all values below 15°, underscoring the Schnepp osteotomy’s reliability for correcting severe hallux valgus. The M1M2 angle showed a 3.6° reduction, ending with a postoperative mean of 11.2°, comparable to other series. Our preoperative DMAA was notably high (25.8°) due to the advanced stage of our cases; however, we observed an impressive correction to 8°, indicating a superior outcome relative to other methods (Table 1).
Overall, our findings in functional and radiologic improvements affirm the Schnepp osteotomy as an effective treatment for severe hallux valgus, with better outcomes compared to other surgical techniques reported in the literature.
In our series of 47 feet, two complications (4.3%) were observed: a single case of hallux rigidus, likely due to preexisting metatarsophalangeal arthritis, and one instance of avascular necrosis of the metatarsal head attributable to excessive soft-tissue dissection. To prevent these, we advocate a limited capsular release that spares the medial collateral fibers, coupled with an early, structured protocol of passive and active mobilization. Compared with the Scarf osteotomy , which carries an overall complication rate of approximately 5.1% [10] (including avascular necrosis, non-union, malunion, infection, and complex regional pain syndrome) , and the Chevron technique, which shows similar complication rates but potential under correction of severe intermetatarsal angles [11], our bipolar Schnepp approach achieves equivalent or superior correction of hallux valgus, intermetatarsal, and distal metatarsal articular angles while maintaining a slightly lower complication profile. Proximal techniques (e.g., Ludloff, Mau) may correct larger deformities but demonstrate higher rates of non-union and vascular compromise [12].
Limitations
We recognize several constraints in our work. Because we relied on chart reviews, as a retrospective study, rather than a prospective protocol, selection and information biases cannot be controles. Our modest cohort size (47 feet) may also limit the ability to detect subtler effects and may reduce the generalizability of our findings to broader patient populations. Lastly, all surgeries were performed by a single surgeon, which could introduce operator-dependent bias.
Conclusion
The bipolar Schnepp osteotomy technique (distal subtraction, proximal addition) offers effective correction for moderate to severe hallux valgus, especially in cases of significant metatarsus varus and a high DMAA angle. This method is notable for its low complication rate and high patient satisfaction. Key advantages include the ability to adjust metatarsal length, plantar displacement, and DMAA while effectively correcting the M1M2 angle without causing metatarsal shortening or metatarsophalangeal joint stiffness.
| Etude | Technique | HVA (◦) | 1-2IMA (◦) | DMAA (◦) | |||
|---|---|---|---|---|---|---|---|
| Pre-op | Post-op 2 ans | Pre-op | Post-op 2 ans | Pre-op | Post-op 2 ans | ||
| Crevoisier (2001) [13] | SCARF | 32 | 17 | 16 | 10 | 13 | 10 |
| Freslon (2005) [14] | SCARF | 31.2 | 17.5 | 12.1 | 7.5 | 13.3 | 11.1 |
| Jardé (1996) [15] | Parties molles +/- P1 | 33.3 | 24.5 | 14.2 | 12 | NP | NP |
| Veri (2001) [16] | Ostéotomie proximal | 37 | 13 | 16 | 6 | NP | NP |
| Shneider (2004) [17] | chevron | 27.6 | 14 | 13.8 | 8.7 | NP | NP |
| Bauer T (2010) [18] | Ostéotomie percutanée Riverdin-isham distal | 30 | 15 | 14 | 11 | 15 | 7 |
| Notre étude | Schneep | 29.8 | 7.6 | 14.8 | 11.2 | 25.8 | 8 |
Table 1: Overview of results: change between preoperative and postoperative values.

References
-
Smith SE, Landorf KB, Butterworth PA, Menz HB (2012) Scarf versus chevron osteotomy for the correction of 1-2 intermetatarsal angle in hallux valgus: a systematic review and meta-analysis. J Foot Ankle Surg 51(4): 437- 444.
-
Schuh R, Willegger M, Holinka J, Ristl R, Windhager R, et al. (2013) Angular correction and complications of proximal first metatarsal osteotomies for hallux valgus deformity. Int Orthop 37(9): 1771-1780.
-
Schnepp J, Carret JP, Courcelles P, Revel JJ, Texier A, et al. (1983) Treatment of hallux valgus with irreducible metatarsus varus of the 1st metatarsus. Bipolar metatarsal osteotomy. Rev Chir Orthop Reparatrice Appar Mot 69(Suppl 2): 113-115.
-
Kitaoka HB, Alexander IJ, Adelaar RS, et al. (1994) Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 15(7): 349-353.
-
Nix S, Smith M, Vicenzino B (2010) Prevalence of hallux valgus in the general population: a systematic review and meta-analysis. J Foot Ankle Res 3: 21.
-
Weil L (2000) Scarf osteotomy for correction of hallux valgus. Historical perspective, surgical technique, and results. Foot Ankle Clin 5: 559-580.
-
Park CH, Cho J, JaeMoon J, Lee WC (2016) Can Double Osteotomy Be a Solution for Adult Hallux Valgus Deformity with an Increased Distal Metatarsal Articular Angle. The Journal of Foot & Ankle Surgery 55(1): 188- 192.
-
Al-Nammari SS, Christofi T, Clark C (2015) Double First Metatarsal and Akin Osteotomy for Severe Hallux Valgus. Foot & Ankle International 36(10).
-
Daria Dykyj (1989) Patholgic anatomy of hallux abducto valgus. Clin Podiatr Med Surg 6(1): 1-15.
-
Matthew SR, Tokarski AR, Elliott AD, Borgert AJ, Jacobs MP (2023) The Incidence of Complications Following Scarf Osteotomy for the Treatment of Hallux Valgus: A Systematic Review with Meta-Analysis. The Journal of Foot and Ankle Surgery 62(4): 610-617.
-
Peng YN, Peng YH, Chen CPC (2024) Chevron osteotomy and scarf osteotomy for hallux valgus angle and intermetatarsal angle correction: a systematic review and meta-analysis of randomized controlled trials. J Orthop Surg Res 19: 566.
-
Ettinger S, Spindler FT, Savli M, DAF Scientific Committee, Baumbach SF (2024) Correction potential and outcome of various surgical procedures for hallux valgus surgery: a living systematic review and meta-analysis. Arch Orthop Trauma Surg 144: 4725-4736.
-
Crevoisier X, Mouhsine E, Ortolano V, Udin B, Dutoit M (2001) The Scarf osteotomy for the treatment of hallux valgus deformity: a review of 84 cases. Foot Ankle Int 22: 970-976.
-
Freslon M, Gayet Le, Bouche G, Hamcha H, Nebout J (2005) Scarf osteotomy for the treatment of Hallux Valgus: a review of 123 cases with a mean follow-up of 4.8 years. Rev Chir Orthop 91: 257-266.
-
Jarde O, Trinquier-Lautard Jl, Meire P, Gabrion A, Vives P (1996) Hallux valgus treated by varus osteotomy of the first phalanx associated with adductor plasty. Rev Chir Orthop 82: 541-548.
-
Veri JP, Pirani SP, Claridge R (2001) Crescentic proximal metatarsal osteotomy for moderate to severe hallux valgus: a mean 12.2 year follow-up study. Foot Ankle Int 22: 817-822.
-
Schneider W, Aigner N, Pinggera O, Knahr K (2004) Chevron osteotomy in hallux valgus. Ten-year results of 112 cases. J Bone Joint Surg Br 86(7): 1016-1020.
-
Bauer T, Biau D, Lortat-Jacob A, Hardy P (2010) Percutaneous hallux valgus correction using the Reverdin-Isham osteotomy. Orthop Tram Surg Res 96: 407-416.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- Pediatric Sinonasal Ewing Sarcoma