Pediatric Sinonasal Ewing Sarcoma
Ewing sarcoma is a malignant tumor usually involving long bones of the extremities. Extraskeletal Ewing sarcoma is less common, involving paravertebral region, chest wall, soft tissue of lower extremities and rarely head and neck region. Ewing sarcoma from the sinonasal cavity is extremely rare. Here we present a sinonasal Ewing sarcoma centered at left anterior ethmoidal air cells from an eleven-year-old girl with EWSR1 rearrangement on FISH and EWSR1::FLI1 gene fusion on next generation sequencing test.
Abbreviations
FISH: Fluorescence In Situ Hybridization; PCR: Polymerase Chain Reaction.
Introduction
Ewing sarcoma is the second most common malignant bone tumor of adolescents and children, usually involving long bones of the extremities. Extraskeletal Ewing sarcoma is less common involving paravertebral region, chest wall, soft tissue of lower extremities and rarely head and neck region and usually affect older patients [1]. The symptoms of extraskeletal Ewing sarcoma includes pain at site of involvement and/or constitutional symptoms. Even though cases of extraskeletal Ewing sarcoma is not uncommon, Ewing sarcoma from the sinonasal cavity is extremely rare and only around 10 cases have been reported [2]. Here we report a rare case of sinonasal Ewing sarcoma with EWSR1 rearrangement in FISH and EWSR1::FLI1 gene fusion in next- generation sequencing.
An 11-year-old female presented with two-three weeks of worsening left proptosis with intermittent blurry vision, no bleeding, headache or nasal drainage. MRI showed a solid mass centered in the left anterior ethmoidal air cells, obstructing the left middle meatus/osteomeatal unit, extending into the left orbital medial extraconal space, bulging towards the left anterior cranial fossa floor possibly within a supraorbital ethmoid air cell, and extending into the medial left orbit results in effacement of the fat planes between the mass and the medial rectus, inferior rectus and superior oblique muscle bellies. No metastasis is identified.
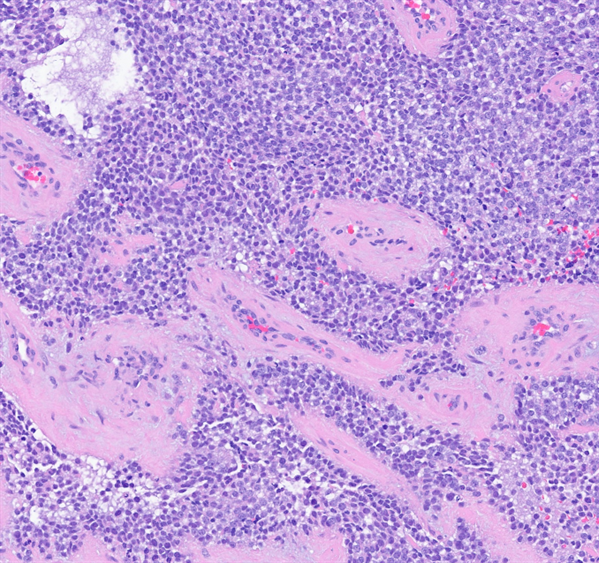
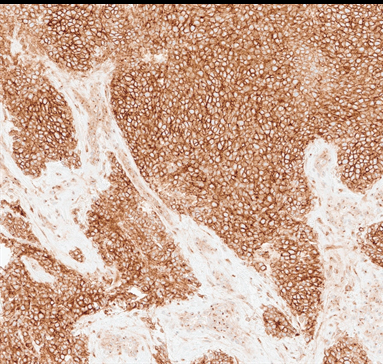
Pathology examination revealed fragments of mucosal tissue intermixed with tiny bony elements. Histologically, sheets of small round blue cells with clear to eosinophilic cytoplasm are present with extensive geographic necrosis and thickened vessels (Figure 1). Tumor cells are positive for immunohistochemical stains of NKX2.2 and CD99 (Figure 2), and negative for pan-cytokeratin, desmin, myogenin, myoD1, CD45, chromogranin A, synaptophysin, CD56, and PHOX2B. INI-1 shows retained nuclear staining.
Formalin-Fixed Paraffin-Embedded slides were submitted for FISH and next-generation sequencing test. For FISH, a dual color assay using the break apart translocation probe EWSR1 was performed to look for a rearrangement of the EWSR1 locus at 22q12. For next-generation sequencing, nucleic acid was isolated and target enrichment of the regions of interest was performed by a hybridization-based methodology using long biotinylated oligonucleotide probes followed by polymerase chain reaction (PCR) and sequencing on Illumina instruments. An in-house bioinformatics pipeline was applied for read alignment, variant and fusion calling and annotation, and comprehensive variant filtering. FISH showed positive for EWSR1 rearrangement. Next- generation sequencing illustrated a fusion between exon 7 of the EWSR1 gene and exon 6 of the FLI1 gene, the most common fusion in Ewing sarcoma.
Discussion
James Ewing described Ewing sarcoma as a rare and aggressive tumor in 1921 [3], a small round cell tumor commonly involving patients in early childhood and adolescence [4]. Ewing sarcoma most commonly occurs in long bones of the extremities. Extraskeletal Ewing sarcoma is less common and involves paravertebral region, chest wall, soft tissue of lower extremities and rarely head and neck region. Extraskeletal involvement in head and neck region is very rare, only 1% to 4% of all Ewing sarcoma [5, 6, 7, 8]. Patients with sinonasal Ewing sarcoma often present with enlarging mass, nasal obstruction, and/or constitutional symptoms such as fever, anemia, or leukocytosis.
Ewing sarcoma is histologically composed of sheets of densely packed cells with round nuclei, fine chromatin and inconspicuous nucleoli, and scant cytoplasm with possible clear appearance by intracytoplasmic glycogen components. PAS stain highlights intracytoplasmic glycogen. Thickened vessels are frequently observed. Immunohistochemical stains usually show tumor cells with positivity of CD99, NKX2.2, and negativity of Desmin, Myogenin, MyoD1, CD45, and PHOX2B. The differential diagnosis includes several other small round blue cells tumors arising in sinonasal tract, such as rhabdomyosarcoma, olfactory neuroblastoma, poorly differentiated carcinomas, and lymphoma [9]. Sinonasal Ewing sarcoma is rare, and it is very important to put it in the differential diagnosis for sinonasal mass, and histologic and immunohistochemical examination could reveal the features of Ewing sarcoma, usually with CD99 and NXK2.2 positivity. FISH study and next-generation sequencing would reveal EWSR1or FUS gene rearrangement and EWSR 1 fusion with various partners, commonly FLI1 or ERG [2]. In this case, FISH demonstrated EWSR 1 gene rearrangement at chromosome 22q12, and next-generation sequencing showed EWSR1::FLI1 gene fusion.
Treatment plan for extraskeletal Ewing sarcoma usually includes a multidisciplinary approach with surgery followed by adjuvant radiotherapy and chemotherapy [10]. This patient received surgery, chemotherapy and radiotherapy with good clinical response. Several factors affect the prognosis, such as patient’s age and presence of distant metastasis [4]. Patients without metastases would expect rate of survival around 55%, and patients younger than 15 would likely have a better outcome. There is no distal metastasis in this patient, and she is less than 15 years old, so the patient would possibly have good prognosis.
Conclusions
A rare case of sinonasal Ewing sarcoma is reported with EWSR1 rearrangement in FISH and EWSR1::FLI1 gene fusion in next-generation sequencing. The differential diagnosis includes small round blue cells tumors arising in sinonasal tract, including rhabdomyosarcoma, olfactory neuroblastoma, poorly differentiated carcinomas, and lymphoma. Treatment usually includes a multidisciplinary approach with surgery followed by adjuvant radiotherapy and chemotherapy, and this patient had good clinical response after the treatment. Patient’s age and presence of distant metastasis affect the prognosis, and this patient has good prognosis since she is less than 15 years old with the absence of distal metastasis.
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Negru ME, Sponghini AP, Rondonotti D, Platini F, Giavarram, et al. (2015) Primary Ewing’s sarcoma of the sinonasal tract, eroding the ethmoid and sphenoid sinus with intracranial extension: A rare case report. Mol Clin Oncol 3(4): 807-810.
-
Lin JK, Liang J (2018) Sinonasal Ewing Sarcoma: A Case Report and Literature Review. Perm J 22: 17-086.
-
Yeshvanth S, Ninan K, Bhandary S, Lakshinarayana KP, Shetty J, et al. (2012) Rare case of extraskeletal Ewings sarcoma of the sinonasal tract. J Cancer Res Ther 8(1): 142-144.
-
Howarth K, Khodaei I, Karkanevatos A, Clarke R (2004) A sinonasal primary Ewing’s sarcoma. Int J Pediatr Otorhinolaryngol 68(2): 221-224.
-
Balamuth NJ, Womer RB (2010) Ewing’s sarcoma. Lancet Oncol 11(2): 184-192.
-
Almomen A, Aldandan A, Alazzeh G, Alkhatib A (2019) Ewing’s Sarcoma of the Sinonasal Tract: A Report of Two Challenging Cases. Indian J Otolaryngol Head Neck Surg 71(Suppl 3): 1849-1853.
-
Amri MF, Abdullah A, Azmi MI, Mohd Zaki F, Md Pauzi SH (2021) Primary sinonasal Ewing sarcoma: A case report. Malays J Pathol 43(2): 319-325.
-
Worthy J, Ganguli MP, Kile MR, Satei AM, Mills ND (2023) A Rare Case of Sinonasal Ewing Sarcoma With Radiologic- Pathologic Correlation. Cureus 15(8): e43708.
-
Hafezi S, Seethala RR, Stelow EB, Mills SE, Leong IT, et al. (2010) Ewing’s family of tumors of the sinonasal tract and maxillary bone. Head Neck Pathol 5(1): 8-16.
-
Souheil J, Skander K, Sawssen D, Sana M, Delia Y, et al. (2016) Ewing sarcomas of the sino-nasal tract and maxillary bone. Egypt J Ear Nose Throat Allied Sci 17(3): 147-153.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet