Mucoepidermoid Carcinoma of Parotid
Mucoepidermoid carcinoma (MEC) is the most common malignant salivary gland tumour comprising approximately 30% of all salivary gland malignancies. It has slight predilection for females in their third to seventh decade of life. Most common site for occurrence in 50% cases is parotid amongst the major salivary glands and palate in minor salivary glands. These lesions usually present as painless swelling associated with discomfort and pressure. WHO describes MEC as a “malignant glandular epithelial neoplasm characterized by mucous, intermediate and epidermoid cells, with columnar, clear cell and oncocytoid features.
Short Communication
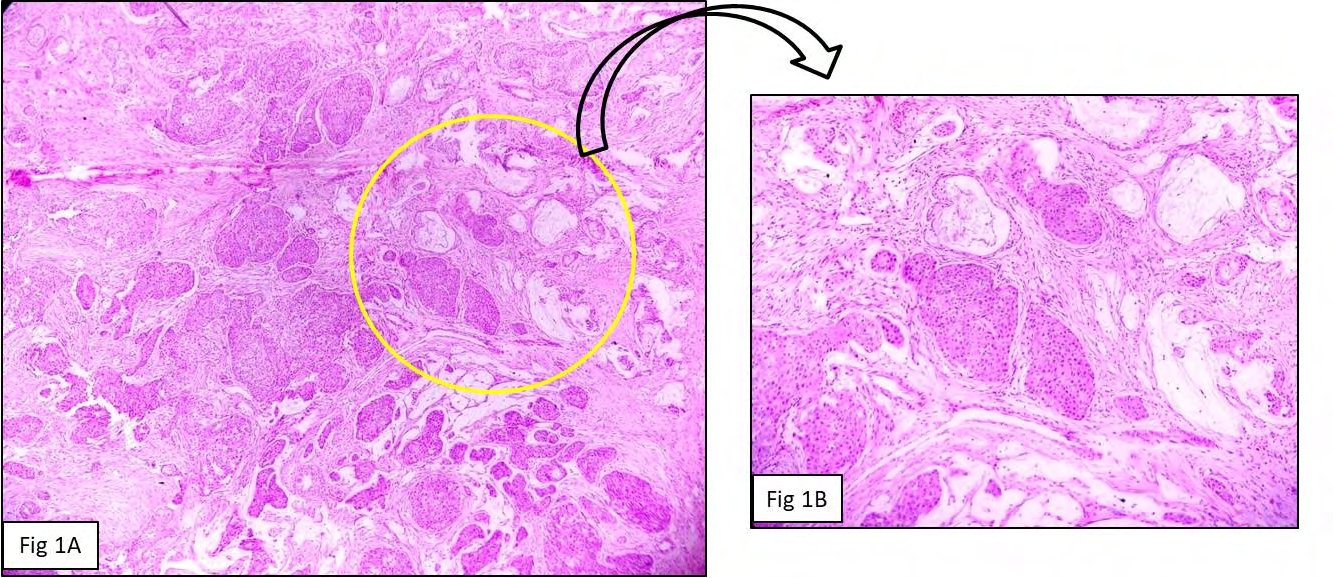
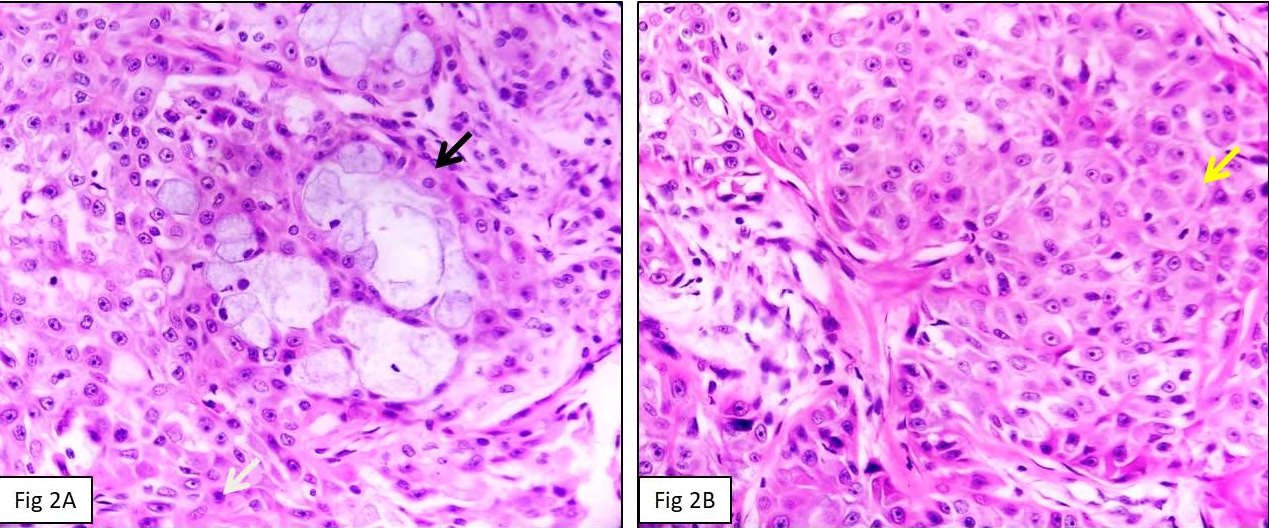
Mucoepidermoid carcinoma (MEC) is the most common malignant salivary gland tumour comprising approximately 30% of all salivary gland malignancies. It has slight predilection for females in their third to seventh decade of life. Most common site for occurrence in 50% cases is parotid amongst the major salivary glands and palate in minor salivary glands. These lesions usually present as painless swelling associated with discomfort and pressure. WHO describes MEC as a “malignant glandular epithelial neoplasm characterized by mucous, intermediate and epidermoid cells, with columnar, clear cell and oncocytoid features”. The proportion of different cell types and their architectural configuration (including cyst formation) varies in and between tumours. They can have multicystic to solid component, the proportion of which plays an important role in deciding the grade of tumour. The cystic spaces are lined by mucous cells which are large, with pale foamy cytoplasm and peripherally displaced nuclei, constituting less than 10% of the tumour. Intermediate type cells are found admixed with epidermoid cells or mucous cells. The intermediate cells range from small basal cells with scanty basophilic cytoplasm to larger and more oval cells with more abundant pale eosinophilic cytoplasm that appears to merge into epidermoid or mucous cells. Clear, columnar and/or oncocytic cell populations may be present and occasionally are prominent [1, 2, 3].
MEC is frequently associated with a t (11; 19) (q14- 21; p12-13) translocation that creates a CRTC1-MAML2 fusion gene. The CRTC1/3-MAML2 fusion is highly specific for MEC. The t (11;19) translocation is occasionally the sole cytogenetic alteration in MEC salivary gland tumors and is also detected in non-salivary gland MEC–like tumors throughout the body, suggesting that the acquired CRTC1- MAML2 fusion is an early core event in MEC pathogenesis.
Many histopathological grading systems have been proposed to grade MEC but none is universally accepted. The Armed Forces Institute of Pathology (AFIP) grading system is a quantitative system [4, 5].
Criteria used are as follows:
- Intracystic component less than 20%- 2
- Neural invasion – 2
- Necrosis – 3
- 4 or more mitoses – 3
- Anaplasia -4 Grade
References
-
Devaraju R, Gantala R, Aitha H, Gotoor SG (2014) Mucoepidermoid carcinoma. BMJ Case Rep.
-
Boahene DKO, Olsen KD, Lewis JE, Pinheiro AD, Pankratz VS, et al. (2004) Mucoepidermoid Carcinoma of the Parotid Gland: The Mayo Clinic Experience. Arch Otolaryngol Head Neck Surg 130(7): 849-856.
-
Diwakar JK, Agarwal A, Garg C, Giri KY, Dandriyal R, et al. (2019) A Rare Case of Mucoepidermoid Carcinoma of Parotid with Mandibular Metastasis. Ann Maxillofac Surg 9(1): 205-207.
-
Thompson LDR, Wenig BM, Muller S, Nelson B (2016) Mucoepidermoid Carcinoma. 2nd (Edn.), Diagnostic Pathology, Head and Neck, Elsevier, pp: 508-517.
-
Seethala RR (2009) An update on grading of salivary gland carcinomas. Head Neck Pathol 3(1): 69-77.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet