Diagnosis of Uterine Leiomyosarcoma and Leiomyoma after Pregnancy with Uterine Leiomyoma
Uterine leiomyomas merger pregnancy has often problems throughout the entire pregnancy period, the treatment policy is a common way of thinking about the uterus conservative therapy. However, it is also argued that enucleation should be actively performed for cases of leiomyomas larger than certain size with some clinical symptoms. In May 2017, the patient visited an obstetrics and gynecology clinic with a chief complaint of irregular bleeding. At the time of the visit, the patient was diagnosed with 8.4 x 6.6 cm uterine leiomyomas and recommended surgical treatment. At the time of the outpatient visit, the pregnancy reaction was judged to be positive. The patient was diagnosed with spontaneous pregnancy by the attending physician and requested follow-up for uterine leiomyomas. Due to her breech birth, selective cesarean section was performed in May 2018 (pregnancy 38 weeks and 1 day). No increase in uterine leiomyomas was observed during the duration of pregnancy. Since then, follow-up for uterine leiomyomas has been continued at outpatient visits. At the outpatient visit in January 2020, the size of the uterine leiomyoma was 6 cm large. However, at the outpatient visit on July 8, 2020, the size of the uterine leiomyoma was found to have increased to 10 cm large. After that, at the outpatient visit on July 15, 2020, an MRI imaging test was performed. As a result of MRI imaging, uterine leiomyosarcoma was suspected, and surgical treatment was performed. The patient was diagnosed with uterine leiomyomas, uterine leiomyomas with Bizarre-like nuclear deformities, and uterine leiomyosarcoma by surgical pathological diagnosis using excised tissue. Currently, follow-up observations regarding tumor recurrence and metastasis are being conducted by outpatient visits every three months.
Introduction
Uterine mesenchymal smooth muscle tumors can be broadly classified into benign uterine mesenchymal smooth muscle tumors with a clinically benign course and uterine leiomyosarcoma with a malignant course. Most benign uterine mesenchymal smooth muscle tumors are uterine leiomyomas, some uterine mesenchymal smooth muscle tumors have a special pathological name, e.g. mitotically active leiomyoma, cellular leiomyoma, leiomyoma with bizarre nuclei, myxoid leiomyoma, epithelioid leiomyoma, malignant trophoblastic tumours, endometrial stromal sarcoma [1]. Although uterine smooth muscle tumors with a special name suggest malignant cell morphology and arrangement or growth rate, the clinical course of these tumors is good [1]. Therefore, independent names have been given to each of these uterine smooth muscle tumors.
In other words, such uterine mesenchymal smooth muscle tumor is a tumor that is required to distinguish from basically malignant tumor, uterine leiomyosarcoma. A clinically benign course is expected only after sufficient differentiation between the two tumors has been made. In addition, in clinical practice, the incidence of these specially named uterine mesenchymal smooth muscle tumors is low, so the full picture of its biological characteristics has not yet been revealed. In particular, cellular leiomyoma, epithelioid smooth muscle tumor, symplastic smooth muscle tumor, leiomyosarcoma with bizarre nuclei, etc. have many problems in distinguishing from uterine leiomyosarcoma [2, 3]. Therefore, it is difficult to establish malignant diagnostic criteria for uterine mesenchymal smooth muscle tumors [1, 4].
Uterine leiomyomas are benign mesenchymal gynecological tumors that increase after the 30s; recently, there is a tendency that the higher the age of the women who wish to become pregnant. Therefore, the effect of uterine leiomyomas on pregnancy and childbirth has become a problem. The frequency of pregnancies with uterine leiomyomas ranges from 2.6% to 3.9% [3]. In the case of pregnancy with uterine leiomyomas, uterine leiomyomas may increase and cause pain during pregnancy. Inpatient treatment may be required in some cases. In addition, perinatal complications such as preterm birth, fetal stunting, fetal position abnormalities, placental abruption and placental abruption tend to increase. In addition, during childbirth, uterine leiomyomas impede the progress of labor; as a result, there is a high probability that a Caesarean section (CS) will have to be performed. This time our clinical team report uterine mesenchymal tumors with mixture of leiomyoma, leiomyoma with Bizarre nuclei and uterine leiomyosarcoma, which were diagnosed in a woman who had a tumor that was thought to be uterine leiomyoma during pregnancy on follow-up at 2 years and 6 months after delivery by Caesarean section.
Case Presentation
On May 13, 2017, a patient visited an obstetrics and gynecology clinic with a main complaint of genital bleeding.
Uterine leiomyomas (84 x 66 mm) were found on pelvic examination and ultrasound imaging. On May 26, 2017, the patient was advised to undergo surgical treatment. Patient visited the Department of Obstetrics and Gynecology at the Kyoto Medical Center with a referral from the doctor in charge. Since the menstruation of the patients was observed two weeks later on April 13, 2017, the possibility of pregnancy was considered. At the outpatient visit on May 26, 2017, a pregnancy test was performed and the patient was positive for Human chorionic gonadotropin (hCG). The patient wanted to give birth. Ultrasound imaging revealed a gestational sac (GS) of 47 mm and fetal heart movement (FHM). From the last menstrual period (LMP) and GS, it was judged to be pregnant (9 weeks 6 days) (Figure 1).
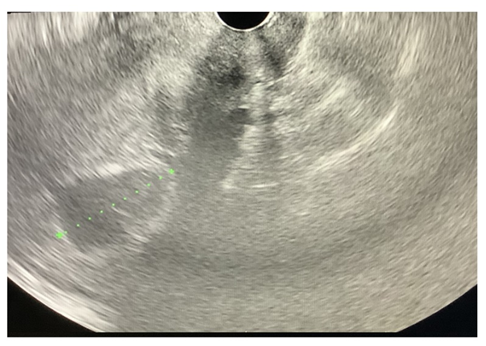
Ultrasound imaging revealed a gestational sac (GS) of 47 mm and fetal heart movement (FHM). From the last menstrual period (LMP) and GS, it was judged to be pregnant (9 weeks 6 days).
Expected date of confinement (EDC) is estimated to be January 18, 2018. Transabdominal ultrasound revealed a 10 cm-sized uterine leiomyoma near the posterior wall of the median, and GS was pushed to the right ventral side. As a result, a tendency of fetal growth restriction (FGR) was considered. Due to pregnancy reasons, no Magnetic Resonance Imaging (MRI) imaging was performed to obtain detailed medical information for uterine mesenchymal tumors. At the outpatient visit on August 26, 2017, transabdominal ultrasound imaging confirmed that the placenta was attached directly above the uterine leiomyoma (Figure 2).
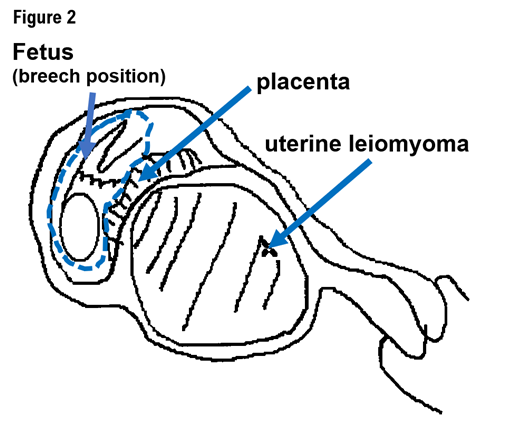
The transabdominal ultrasound imaging confirmed that the placenta was attached directly above the uterine leiomyoma. Fetal morphology screening revealed no major malformations. Because the fetus is in the breech position (breech) and the patient requested permanent sterilization.
The size of the leiomyoma was 10 cm, and no increase was observed. August 26, 2017, the possibility of physiological uterine contractions and water rupture was considered due to large uterine leiomyomas. In order to prevent imminent miscarriage and premature birth, treatment with oral tocolytic agent ritodorine hydrochloride 3T/3x was started.
At the outpatient clinic on December 27, 2017, transabdominal ultrasound imaging confirmed that the fetal movement was good and the amniotic fluid cavity was maintained. Transabdominal ultrasound confirmed that uterine leiomyomas 8.5 cm in size did not grow. It was confirmed that the placenta was attached just above the uterine leiomyomas and that it was not placenta previa. Umbilical cord ptosis was not observed. Fetal morphology screening revealed no major malformations. Because the fetus is in the breech position (breech) and the patient requested permanent sterilization. At the preoperative conference held on December 27, 2017, it was decided that on January 5, 2018 (pregnancy 38 weeks and 1 day); selective cesarean section and surgical treatment for bilateral salpingectomy would be performed.
On January 5, 2018 (pregnancy 38 weeks and 1 day), selective cesarean section and bilateral salpingectomy were performed as scheduled. The newborn weighed 2406 g, [Apgar index 8/9, Umbilical cord arterial blood gas test value (UmA)-pH 7.385, base excess (BE) -1]. The newborn was admitted to pediatrics as a low birth weight infant. On January 09, 2018, a gynecological liquefied sample cytology (LBC) method was performed. The attending physician informed the patient that the medical staff would follow medically for uterine leiomyomas if there were no subjective symptoms. Specifically, medical follow-up for uterine leiomyomas every 6 months and annual cancer screening will be performed. In addition, the patient requested the doctor in charge to treat uterine leiomyomas if subjective symptoms were strongly observed. On January 21, 2018, Negative for intraepithelial lesion or malignancy was diagnosed based on the results of cytodiagnosis using LBC of the vaginal neck. No cells with obvious dysplasia or suspected malignancy were found. On February 07, 2018, the patient’s postpartum course was good, and his vital signs were stable. Life restrictions on patients have been lifted. On July 03, 2019, a small amount of white vaginal discharge was observed, but no cervical erosion was observed. Transvaginal ultrasound imaging showed no increase in uterine leiomyomas (59 x 52 mm) present on the posterior wall of the uterine anteflexion/ endometrial hyperplasia phase. No abnormalities in the bilateral appendages (ovaries) and ascites were observed.
On January 08, 2020, a small amount of white vaginal discharge was observed, but no cervical erosion was observed. Transvaginal ultrasound imaging showed no apparent increase in uterine leiomyomas (61 x 50 mm) present on the posterior wall of the uterine anteflexion / endometrial hyperplasia phase. No abnormalities were found in the bilateral appendages (ovaries) and ascites. Cytology using LBC of the vaginal neck was performed. On January 22, 2020, Negative for intraepithelial lesion or malignancy was diagnosed based on the results of cytodiagnosis using LBC in the vaginal neck. No cells with obvious dysplasia or suspected malignancy were found. However, since the cytological specimen did not contain cervical glandular epithelium and transitional cell cells, it was recommended that LBC cytology using vaginal cervical be performed again within 12 months.
On July 08, 2020, the patient complained of subjective symptoms of tumor growth. The patient’s menstrual cycle is not stable. A small amount of white vaginal discharge was observed, but no cervical erosion was observed. Transvaginal ultrasound imaging showed thin uterine anteflexion and endometrium. An increase in uterine leiomyomas (100 x 71 mm) was observed compared to the January 2020 examination. On July 22, 2020, MRI imaging revealed a new tumor in addition to the previously observed uterine leiomyomas. MRI T1 and T2 imaging showed a marked low signal at T2W1 and a mild high signal at T1W1 on the caudal side of the tumor. After contrast, a markedly poorly contrasted tumor was shown compared to the surrounding muscularis. On the head side of the tumor, T2W1 showed mild hyperintensity and marked diffusion limitation. After imaging, the cranial side of the tumor was shown as a lobulated region showing a non-uniform enhancing effect, including a dorsal defective area. MRI T1 and T2 imaging showed a partial area of suspected necrosis, suggesting uterine leiomyosarcoma, a malignant tumor associated with uterine leiomyomas. There are no findings suggestive of apparent cancer infiltration into surrounding organs. Clear lymph node swelling was not observed in the imaging range. Our clinical team highlighted the importance of discussion with patients regarding the risk of occult malignancy in a fibroid uterus.
The attending physician informed the patient that total hysterectomy and bilateral adnexectomy were desirable as future treatment strategies. On August 03, 2020, Computed tomography (CT) image examination of the entire trunk contrast revealed two tumors touching the top and bottom and occupying the left wall of the uterus. The lower tumor was associated with marginal calcification. CT imaging of the whole trunk revealed a mass in the left lobe of the thyroid gland and a nodule suspected to be inflammatory in the lower lobe of the right lung.
On August 13, 2020, a simple hysterectomy and bilateral accessory resection were performed with a midline incision in the lower abdomen. The attending physician informed the patient that patient would be followed up every three months after the surgical treatment. In addition, the doctor in charge instructed the patient to come to the hospital immediately if the patient had subjective symptoms such as pain. On August 18, 2020, fine needle aspiration biopsy (FNA) was performed on a tumor in the left lobe of the thyroid gland that was found on CT imaging of the entire trunk. From the FNA test results, no findings suspected of being malformed or malignant were found. Follow-up is being performed on the left lobe mass of the thyroid gland.
On August 28, 2020, at the Gynecological Pathology Conference, pathological images showed uterine smooth muscle with severe cell atypia and lobular proliferative morphology (Figure 3).
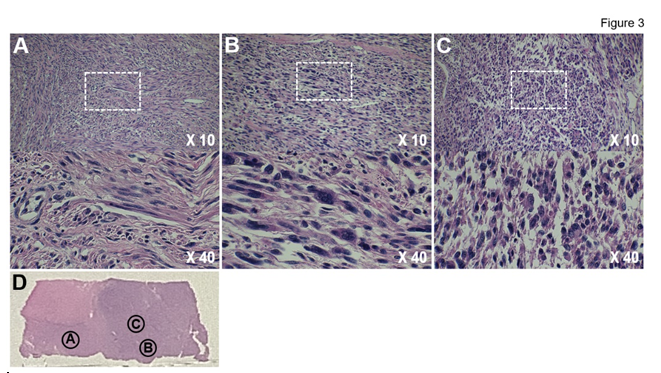
Pathological images show uterine smooth muscle tumors with severe cell atypia and lobular proliferative morphology. The margin of the tumor was pushing and the boundary was clear. Coagulative necrosis was evident and pathological images showed a mixture of A) Uterine leiomyoma B) Uterine leiomyoma cells with bizarre-like nuclear deformities and C) Uterine leiomyosarcoma in uterine tumor section. (D) Picture of whole tissue section.
The margin of the tumor is pushing, and the boundary is clear. No coagulative necrosis was found in the tumor. Pathological images showed a mixture of (A) uterine leiomyoma, (B) uterine leiomyoma cells with Bizarre- like nuclear deformities, and (C) uterine leiomyosarcoma (Figure 3).
Discussion
The incidence of uterine leiomyosarcoma is uncommon, registering 0.64/100 000 women annually. It accounts for approximately 1.3% of all uterine malignancies. The first treatment for uterine leiomyosarcoma is only surgical treatment, but there are serious problems with the risk of postoperative-residual leiomyosarcoma and the risk of frequent recurrence. Therefore, uterine leiomyosarcomas are usually highly malignant neoplasms with an overall poor prognosis. Most commonly, Uterine leiomyosarcoma presents after childbearing age. Occurrence during childbearing age is not common and uterine leiomyosarcomas during pregnancy is even rarer in medical literature.
The development of medical technology is remarkable, but since uterine mesenchymal tumors have the variety of morphologies, the full picture of their biological characteristics has not been clarified. Furthermore, there is no medical or biological evidence that a benign tumor, uterine leiomyoma, transforms into a malignant tumor, uterine leiomyosarcoma. However, many of the uterine leiomyosarcoma, are concurrent with uterine leiomyomas. Like gestational trophoblastic disease, mitotically active leiomyomas are usually found in women of reproductive age and associate with secretory endometrium, pregnancy, and drugs (progestogens and tamoxifen) [5, 6]. In particular, pregnancy with uterine leiomyomas has many problems, but it is also necessary to consider actively performing uterine enucleation [7].
Conclusion
Pregnancy with uterine leiomyomas has many problems. E.g. imminent premature birth, placental abruption, throughout the entire gestation period, and the treatment policy is a common way of thinking about the uterus conservative therapy. There is no medical evidence that uterine leiomyomas transform into malignant mesenchymal tumor, i.e. uterine leiomyosarcoma. However, some argue that enucleation should be actively performed in patients with myomas larger than a certain size and some clinical symptoms. For pregnancies with uterine leiomyoma, regular postnatal follow-up after caesarean section is necessary to capture morphological changes in the tumor.
Author Contributions
TH and KS performed diagnostic pathological studies, coordinated the project, created the study, and wrote the manuscript. IK carefully reviewed the manuscript and commented on the aspects of clinical medicine. IK shared information on clinical medicine and oversaw the entirety of the study.
Footnote
The material (manuscript and figure) is original research. It has not been previously published and has not been submitted for publication elsewhere while under consideration.
Disclosure of Potential Conflicts of Interest
The authors declare no potential conflicts of interest.
Data Availability and Consent to Publish
This manuscript is an editorial and does not contain research data.
Therefore, there is no research data or information to be published or opened.
Research Funding
This clinical research was performed with the support of the following research funding: Japan Society for the Promotion of Science for TH (grant No. 19K09840), START- program Japan Science and Technology Agency (JST) for TH (grant No. STSC20001), and National Hospital Organization Multicenter clinical study for TH (grant No. 2019- Cancer in general-02).
Acknowledgment
We thank all the medical staffs and co-medical staffs for their contribution to the medical research at National Hospital Organization Kyoto Medical Center. We appreciate Crimson Interactive Japan Co., Ltd., for revising and polishing our manuscript.
References
-
Kempson RL, Hendrickson MR (1988) Pure mesenchymal neoplasms of the uterine corpus: Selected problems. Semin Diagn Pathol 5(2): 172-198.
-
Zaloudek, Hendrickson, Soslow (2011) Bluestein’s Pathology of the Female Genital Tract. 6th(Edn.), Springer, New York, 3: 453-578.
-
Hayashi T, Yaegashi N, Tonegawa S, Konishi I (2021) Potential biomarkers associated with malignancy in uterine mesenchymal tumors. European Journal of Gynaecological Oncology 42(5): 824-828.
-
Suwandinata FS, Gruessner SE, Omwandho CO, Tinneberg HR (2008) Pregnancy-preserving myomectomy: Preliminary report on a new surgical technique. Eur J Contracept Reprod Health Care. 13(3): 323-326.
-
WHO (2020) Uterine leiomyosarcoma Female Genital Tumours, WHO Classification of Tumours, 5th (Edn.), Classification of Tumours Editorial Board. World Health Organization 4: 272-276.
-
Jagtap SV, Aher V, Gadhiya S, Jagtap SS (2017) Gestational Trophoblastic Disease- Clinicopathological Study at Tertiary Care Hospital. J Clin Diagn Res 11(8): EC27- EC30.
-
Amant F, Van Calsteren K, Halaska MJ, Beijnen J, Lagae L, et al. (2009) Gynecologic cancers during pregnancy: guidelines of an international consensus meeting. Int J Gynecol Cancer 19: 1-12.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet