Talon Cusp, Tooth Transposition, Taurodontism-Occurrence of “T Anomalies” Together in a Non-Syndromic Child-A Rarest Case Report
Presenting of rare and unusual dental anomalies is always essential to enhance the richness of existing dental literature pertaining to these anomalies. Developmental dental anomalies starting from the alphabet ‘T’ such as Talon cusp, Transposition and Taurodontism are the uncommon dental phenomenon’s which are reported individually. However, occurrence of all these anomalies together is not reported so far. Therefore, the purpose of the present article is to report occurrences of all these dental anomalies together in detail in a 9-year-old, normal, healthy Indian male patient.
Introduction
‘Talon cusp’ also called as Eagle’s talon as mentioned by Mellor and Ripa is an anomaly of the tooth shape and is characterized by ‘a cusp-like projection seen in palatal or labial surface of an anterior teeth which extends at least half the distance from the cemento-enamel junction to the incisal edge [1]. Although this anomaly has been reported more frequently in permanent maxillary anterior teeth, its occurrence in permanent mandibular anterior teeth is a rarity [2]. Literature shows mandibular talon cusps are more common in males than females with a ratio of 7:3 [3]. A systematic review on mandibular talon cusps revealed that a total of only 35 articles with 43 patients were reported with mandibular talon cusps across the globe among those one was prevalence study and remaining were only case reports. In that, forty cases (93%) are documented in permanent dentition and rest three cases (7%) are reported in the primary dentition [2].
Tooth transposition is a disturbance of tooth eruption and is defined as ‘interchange in the position of two permanent adjacent teeth within the same quadrant. [4] It is the most difficult dental anomaly to treat in the dental clinic as it represents a unique and severe condition of ectopic eruption. The reported incidence of transposition is low ranging from 0.2% to 0.38% in the general population, most commonly encountered in females, with majority being found in the maxilla (76%) [4]. This clinical condition may occur either unilateral or bilateral, but unilateral occurrence is the most common. The commonly involved teeth by transposition phenomenon are the maxillary canines and first premolars. In deciduous dentition transposition is not reported so far.
Taurodontism is an uncommon dental anomaly of morpho-anatomical changes in the tooth shape characterized by ‘teeth with enlarged and elongated pulp chambers and apical displacement of the bifurcation or trifurcation of the roots.’ The term taurodontism is taken from the Latin word ‘tauros’ meaning bull and Greek term ‘odus’ which means tooth or bull tooth [5]. This anomaly is characterized by an enlarged apically displaced pulp chamber, a proportionately shortened root, and an enlarged pulp chamber in the affected dentition and apically displaced furcation areas [6]. The bifurcation may be only a few millimetres above the apices of the roots. Moreover, the teeth do not show the usual constriction at the cemento-enamel junction observed in molars with a normal pulp chamber. Taurodontism is most frequently reported in permanent mandibular molars either unilaterally or bilaterally and in any combination of teeth or quadrants [6].
Extensive review of dental literature revealed individual reports on the above dental anomalies [7, 8].
From author’s best of best current knowledge, reports on occurrence of all these anomalies together in a single, normal patient is not reported so far. Therefore, the purpose of this article is to show the occurrence of ‘T’ anomalies such as Talon cusp, Tooth Transposition, and Taurodontism in a 9-year-old healthy, non-syndromic Indian male patient. One more interesting point regarding this case is related to tooth transposition. Previous published reports showed occurrence of tooth transposition in erupted teeth into the oral cavity. In this case, the transposition phenomenon was noticed in the intra-osseous stage involving erupting teeth buds which are not reported till date.
Case Report
A 9-year-old male patient reported to a private dental clinic complaining of delay in eruption of new set of teeth in the lower front region. On physical examination, patient appeared healthy, moderately built, well-nourished and did not exhibit any signs and symptoms of any syndromic features or systemic and metabolic disorders. On intraoral examination, patient was found with mixed dentition, oral hygiene was good and few deciduous teeth were mobile. On further examination, talon cusp was noticed in relation to the permanent mandibular left lateral incisor. To confirm the presence of other permanent teeth buds, an orthopantomograph radiograph was advised. On examination of the Orthopantomograph, presence of talon cusp was confirmed as it appeared a ‘V’ shaped radiopaque structure extending from cemento-enamel junction of lateral incisor to the 1 mm below the incisal edge (Figure 1). On careful examination of the radiograph, the permanent maxillary right canine tooth bud was located in between first and second premolars tooth buds. The first premolar was located in the canine position. The root development was not completed in these three teeth. On the contralateral side, the positions of canines and premolars tooth buds were correct. Radiograph also showed the presence of taurodontism in the permanent maxillary and mandibular first molars (Figure 1 & Table 1). Finally based on clinical features, radiographic findings and literature search the case was diagnosed as non-syndromic, congenital, idiopathic occurrence of tooth transposition, taurodontism and talon cusp was made. The detailed description of all these anomalies is elaborated in Table 2. Patient did not experience any discomfort from the talon cusp present in the mandibular lateral incisor. Therefore patient did not require any particular treatment and parents were informed about the presence of these anomalies, educated to maintain good oral hygiene and kept under observation.
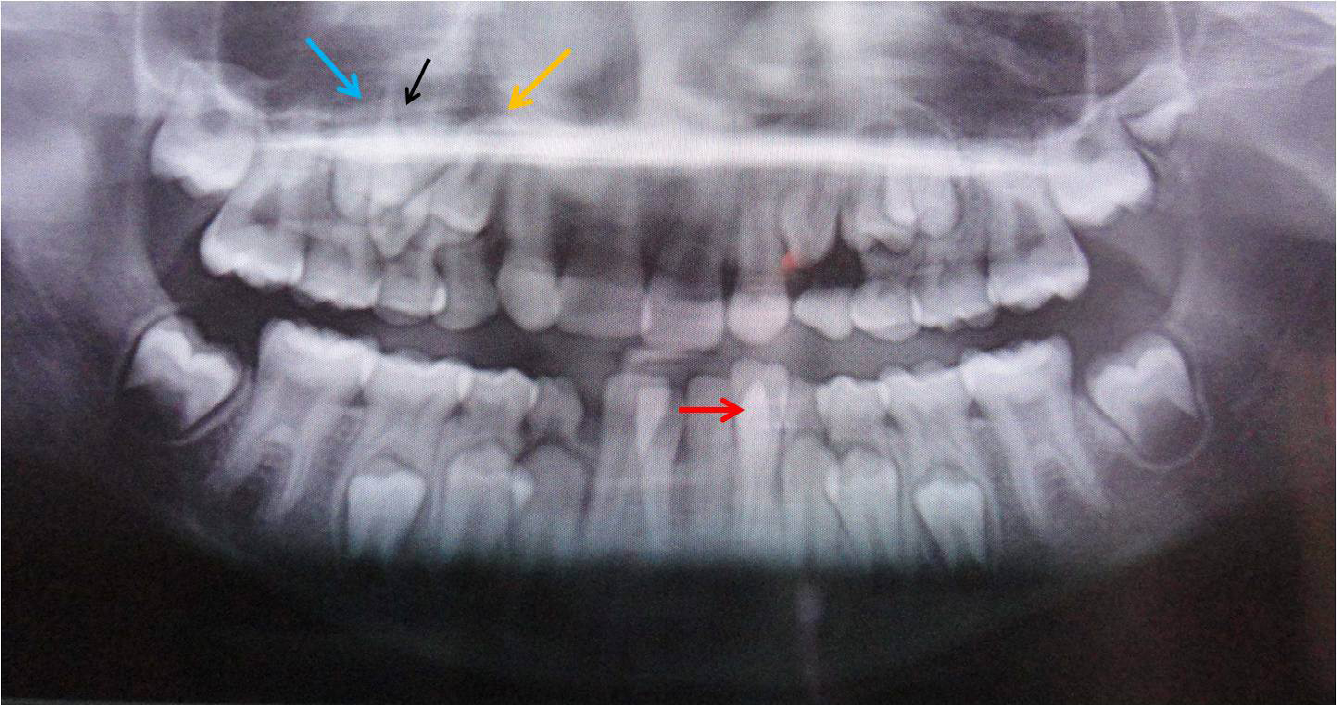
Figure 1: Orthopantomograph Showing Talon Cusp (Red Arrow) in Permanent Mandibular Left Lateral Incisor, Tooth Transposition in Relation to Permanent Maxillary Right Canine (Black Arrow) with Right First Premolar (Yellow Arrow) and Taurodontism in Permanent Maxillary and Mandibular First Molars. Maxillary Right Canine Tooth Bud (Black Arrow) is Located between First (Yellow Arrow) and Second Premolars (Blue Arrow).
| Patient age | Gender | Chief complaint | History of dental trauma | Clinical features | Radiographic features |
|---|---|---|---|---|---|
| 9 years | Male | Delay in eruption of new set of teeth in the upper front region | Absent | Mixed dentition stage Presence of talon cusp in relation to permanent mandibular left lateral incisor. | Presence of talon cusp (appeared as ‘V’shaped radiopaque structure extending from cement-enamel junction of mandibular left lateral incisor towards incisal edge. Transposition of permanent maxillary right canine and first premolar. Presence of taurodontism in permanent maxillary and mandibular first molars. |
Table 1: Details of Patient’s Demographic Profile.
| Talon cusp | Tooth Transposition | Taurodontism | |
|---|---|---|---|
| Location | Mandible | Maxilla | Both maxilla and mandible |
| Laterality | Unilateral | Unilateral | Bilateral |
| Side affected | Left | Right | Both right and left side |
| Teeth involved | Permanent mandibular left lateral incisor | Permanent maxillary right canine and first premolar | Permanent maxillary and mandibular first molars |
| Type/Classification | Type I talon | Mx.C.P1 Complete type | Mesotaurodont |
| Classification Proposed author and year | Hattab, et al. [7] | Peck S, et al. [4] | Shaw [8] |
| Associated clinical problem | |||
| Treatment provided | None, only Observation | None, only Observation | None, only Observation |
Table 2: Details of ‘T’ Anomalies-Talon Cusp, Tooth Transposition, Taurodontism in a Child.
Discussion
Talon cusps most commonly affect permanent maxillary lateral incisors. Occurrence of talon cusp in mandibular anterior teeth is rare and a resent research article revealed that most of the mandibular talon cusps were reported from Asia, with 90% cases was documented from India [2]. Pertaining to mandibular arch, its occurrence is quiet low. In a systematic review [2], it is stated that eight cases (19%) were found in archeological skulls and remaining are only case reports. Among the reported cases, lingual talons are more frequently documented in mandible than labial talon cusps in permanent dentition. About 30% (12 cases) were found on labial surface, 68% (27 cases) were found on lingual surface and only one case (2%) noticed on both surfaces. In mandibular talon cusps, majority occurred unilateral and seven cases, (17.5%) exhibited bilateral presentation [2]. Among total of 43 cases, 36 cases were noticed on central incisors, three were on lateral incisors and two cases reported in canines. In mandible, comparatively left side incisors are more affected than right side. The most common dental anomaly reported with mandibular talon cusp was the double tooth [2]. The author of this paper previously investigated 21 cases of talon cups in Indian population [3]. In this study, author found two cases of talon cusps occurring in mandibular central incisors [3]. In the present case, the talon cusp was found in permanent mandibular lateral incisor and was on left side (unilateral occurrence) and other anomalies found were canine-first premolar transposition and taurodontism involving all permanent molars which is not reported so far.
Various classification systems have been proposed by different authors Mallineni SK [2, 3] along with conventional classification given by Hattab, et al. [7] (Table 3). Based on this classification, the talon cusp was categorised as type I (True) talon in the present case because both clinically and radiographically it was confirmed by presence of a prominent ‘V’ shaped structure appeared on lingual surface extending from cemento-enamel junction towards the incisal edge. Various treatment modalities are described by different clinicians based on the prominence and clinical problem associated with talon cusp, such as fissure sealing, composite resin restoration, gradual reduction of bulk of the cusp with application of topical fluoride to reduce sensitivity and stimulate reparative dentin formation for pulp protection and total reduction of whole cusp followed by pulpotomy or root canal treatment [2, 3, 7]. In the present case, no treatment was carried out as the talon cusp was not causing any problem.
| Talon Cusp type | Description |
|---|---|
| Type I – True Talon | Refers to a morphologically well-delineated additional cusp that prominently projects from the palatal surface of a primary or permanent anterior tooth and extends at least half the distance from the cement- enamel junction to the incisal edge. |
| Type II – Semi talon | Refers to an additional cusp of 1 mm or more, but extending less than half the distance from the cement- enamel junction to the incisal edge. It may blend with the palatal surface or stand away from the rest of the crown. |
| Type III – Trace talon | Refers to an enlarged or prominent cingulam in any of its variants (conical, bifid, or tubercle-like) originating from the cervical third of the crown. |
Table 3: Classification of Talon Cusp - Given by Hattab, et al. [7].
Tooth transposition is an interesting dental phenomenon and has been described by Peck et al as ‘positional interchange of two adjacent teeth particularly of the roots or the development or eruption of a tooth in a position occupied normally by a non-adjacent tooth [4]. Peck, et al. [4] classified tooth transpositions into five types based on the particular tooth transposed. The detailed description of this classification is presented in Table 4. Tooth transposition can also be categorized as ‘complete’ or ‘true’ and ‘incomplete’ or ‘pseudo’ transposition. In complete transposition, the crowns and the roots of the affected teeth exchange places in the dental arch. In the condition of incomplete transposition, the crowns are transposed, but the roots remain in their normal positions. In the present case, the transposition found was complete type because both crown and root of canine was transposed with crown and root of first premolar. Although root development was not completed in both teeth, but the whole teeth buds were in complete transposed position based on radiographic examination. The specialty of this case compared to other previously published reports is that, transposition process was of intra-osseous nature involving erupting teeth buds within the alveolar bone.
| Types | Description | Notation system |
|---|---|---|
| 1 | Maxillary Canine – First premolar transposition | (Mx.C.P1) |
| 2 | Maxillary Canine – Lateral incisor transposition | (Mx.C.I2) |
| 3 | Maxillary Canine – First molar transposition | (Mx.C.M1) |
| 4 | Maxillary Lateral incisor – Central incisor transposition | (Mx.I2.I1) |
| 5 | Maxillary Canine – Central incisor transposition | (Mx.C.I1) |
Table 4: Classification of Tooth Transposition - Given by Peck, et al. [4].
The prevalence studies reported in different ethnic groups such as Turkish (0.27-0.33%), Saudi Arabia (0.13%), Germany (0.09%), India (0.41%), Greece (0.13-0.65%) and Nigeria (0.14-0.38%) stated that tooth transposition might be considered a rare phenomenon because of low frequency in occurrence [9, 10, 11]. In the present case, transposition was found in the maxilla, and even literature shows predilection for maxilla compared to mandible [12]. The reason for this is due to the high bone density of the mandible prevents the phenomenon of tooth transposition and hence lesser prevalence in the mandible. There is contradictory finding regarding increased occurrence of transposition in right or left side [9, 12]. In the present case, transposition occurred on the right side showing unilateral presentation which is more frequently reported in the maxilla. Literature shows canine tooth is the most commonly affected in transposition cases with either lateral incisor or first premolar [4, 9, 13].
The hypothesis behind this nature of occurrence is related to the longest period of development and longest path of eruption of canines [12]. In addition to this, maxillary canine- first premolar transposition is the most commonly reported transposition with a prevalence of 0.13-0.51% among other five classifications given by Peck and Peck [4]. Even in this case reported here, canine-first premolar transposition (Mx.C.P1) was found.
The exact etiology behind the phenomenon of transposition is still not clear. However, various theories have been proposed like migration of a tooth bud during eruption, heredity, the presence of retained primary teeth, interchange of developing teeth and mechanical interferences. Sometimes, bone pathologies such as cyst formation and odontomas may cause displacement and transposition of the tooth. Even, history of trauma to the primary teeth suggested as possible etiologic factor in transposition cases [4, 9, 13]. However in the present case, none of these factors were evident and it may be due to the interchange of tooth buds due to genetic influence. There is no definite treatment for complete transposition cases except of orthodontic movement of transposed teeth to their original position. But this type of treatment modality is very challenging and associated with many complications. Therefore in the present case as teeth were still in eruptive stage no treatment was considered and patient was kept under observation till their complete eruption into the oral cavity.
Taurodontism occur majority of time as an isolated anomaly; however some syndromes have been reported in association with taurodontism such as Down’s syndrome, hypophosphatasia, and Klinefelter syndrome [14, 15, 16]. Taurodontism is also associated with microdontia, amelogenesis imperfecta and dens invaginatus [8, 17]. But in the present case, taurodontism was evident in all permanent first molars along with presence of tooth transposition and talon cusp. This concurrent occurrence of three anomalies is not reported so far thereby considering this case as an uncommon interesting case. Even primary mandibular both right and left second molars too exhibited taurodontism (mesotaurodont type) on radiographic examination. But as the root resorption was started in mesial roots, it was quite difficult to appreciate the morphology of molars and to conclude with final diagnosis.
Diagnosis of taurodontism is possible only on radiographic examination, as the crown morphology of the tooth appear clinically normal [5, 15, 18]. Taurodontism is classified by different authors based on numerous criteria [17, 18]. The first classification system was given by Shaw in 1928 [8], based on the relative amount of apical displacement of the pulp chamber floor which is elaborated in Table 5. In addition to this, Keene in 1966 gave ‘Taurodont Index’ based on the relative height of the pulp chamber to the length of the longest root and different index values for each hypo, meso and hypertaurodont tooth is given [17]. However, the most widely used classification is given by Shifman, et al. [18] based on the anatomical landmarks of the taurodont tooth. In the case described here, taurodontism was categorized as ‘mesotaurodont’ based on Shaw classification [8]. The etiology behind occurrence of all these individual conditions is entirely different as mentioned in the literature. The possible etiology for occurrence these anomalies together described in this case report is might be due to genetic influence or idiopathic in nature.
| Types | Description |
|---|---|
| Hypotaurodont | Moderate enlargement of the pulp chamber at the expense of the roots |
| Mesotaurodont | Quite large pulp and short roots but still separate |
| Hypertaurodont | Pulp chamber nearly reaches the apex giving prismatic or cylindrical forms and then breaks up into 2 or 4 channels. |
Taurodontism not only affects permanent molars but also reported in primary molars [6]. From author’s archive, prevalence study has been reported in primary mandibular first molars in Indian children and reported with a prevalence of 4% [6]. The presence of taurodontism has various clinical implications during clinical practice including endodontics, orthodontics, prosthodontics and periodontics. It poses difficulties during endodontic treatments, reduces the root canal surface area available for post anchorage and complicates orthodontic treatment due to increased tendency to root resorption [5, 15, 18].
Different obturation techniques should be followed during endodontic management of teeth affected with taurodontism. Therefore, it is highly essential for all clinicians to have in depth knowledge about taurodontism and management of such teeth in clinical practice.
Talon cusp exhibits in varied form and shapes. The present author previously published unusual occurrence of talon cusps in Indian ethnic groups [19, 20]. One is occurrence of type I true talon cusp in lingual aspect of mesiodens having three lobes. In this case, Nagaveni NB [19] explained both the clinical and radiographic appearance of this different anomaly. Another case is the presence of talon cups in permanent mandibular central incisor. The central incisor was macrodontic and itself having other anomalies like short root anomaly and dens invaginatus along with talon cusp [20].
Occurrence of all these anomalies did not give rise to any clinical problems as they were clinically normal and not affected by any dental pathology. Preventive measures should be regularly followed in these teeth to avoid any complications. In case of taurodontic molars pit and fissure sealants and fluoride application should be carried out to avoid occurrence of dental caries in the future as the root canal treatment is challenging in these teeth. In case of mandibular lateral incisor with talon cusp, oral prophylactic measures help to prevent occurrence of dental caries and its consequences in the future. Tooth transposition will not lead to any clinical problem except for tooth appearance in this case.
Conclusion
Therefore, finally to conclude author would like to suggest that from previous research and from the above case presentation it is clear that, majority of rare anomalies are reported from Indian context. This paper should be a platform for other researchers to explore and report more and more cases or prevalence studies pertaining to these three anomalies in order to formulate more appropriate classification systems and to draw proper guidelines in management of these types of cases during clinical practice.
References
-
Mellor JK, Ripa LW (1970) Talon cusp: a clinically significant anomaly. Oral Surg Oral Med Oral Pathol 29(2): 225-228.
-
Mallineni SK, Panampally GK, Chen Y, Tian T (2014) Mandibular talon cusps: A Systematic review and data analysis. J Clin Exp Dent 6(4): 408-413.
-
Nagaveni NB, Umashankara KV (2014) A clinical and radiographic retrospective analysis of talon cusps in ethnic Indian children. Journal of Cranio-Maxillary Diseases 3(2): 79-84.
-
Peck S, Peck L (1995) Classification of maxillary tooth transpositions: Am J Orthod Dentofacial Orthop 107(5): 505-517.
-
Witkop CJ (1976) Clinical aspects of dental anomalies. Int Dent J 26(4): 378-390.
-
Nagaveni NB, Radhika NB (2012) Prevalence of taurodontism in primary mandibular first molars of ethnic Indian children. Gen Dent 60(5): 335-340.
-
Hattab FN, Yassin OM, Al-Nimri KS (1996) Talon cusp in permanent dentition associated with other dental anomalies: Review of literature and reports of seven cases. ASDC J Dent Child 63(5): 368-376.
-
Shaw JC (1928) Taurodont teeth in South African races. J Anat 62(Pt 4): 476-498.
-
Onyeaso CO, Onyeaso AO (2006) Occlusal/dental anomalies found in a random sample of Nigerian school children. Oral Health Prev Dent 4(3): 181-186.
-
Kavadia-Tsatala S, Sidiropoulou S, Kaklamanos EG, Chatziyanni A (2003) Tooth transpositions associated with dental anomalies and treatment management in a sample of orthodontic patients. J Clin Pediatr Dent 28(1): 19-25.
-
Umweni AA, Ojo MA (1997) The frequency of tooth transposition in Nigerians, it’s possible aetiologic factors and clinical implications. J Dent Assoc S Afr 52(9): 551- 554.
-
Nakane Matsumoto MA, Sasso Stuani MB (2018) Tooth transposition: a multidisciplinary approach. Dental Press J Orthod 23(1): 97-107.
-
Seth P, Halasagundi VS, Tegginamani AS, Singh AK (2019) Dental transposition of Mx.C.I2 and associated with supernumerary teeth. Indian J Oral Health Res 5(2): 54-55.
-
Houpt MI, Kenny FM, Listgarten M (1970) Hypophosphatasia: Case reports. ASDC J Dent Child 37(2): 126-137.
-
Joseph M (2008) Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefelter syndrome: A review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 105(5): 670-677.
-
Jaspers MT (1981) Taurodontism in the Down syndrome. Oral Surg Oral Med Oral Pathol 51(6): 632-636.
-
Keene HJ (1966) A morphologic and biometric study of taurodontism in a contemporary population. Am J Phys Anthropol 25: 208-9.
-
Shifman A, Chanannel I (1978) Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dent Oral Epidemiol 6(4): 200-203.
-
Nagaveni NB, Umashankara KV, Sreedevi, Reddy BP, Radhika NB, et al. (2010) Muli-lobed mesiodens with a palatal talon cusp –A Rare case report. Braz Dent J 21(4): 375-378.
-
Nagaveni NB, Umashankara KV, Vidhyullatha BG, Sreedevi, Radhika NB (2011) Permanent mandibular incisor with multiple anomalies – Report of a rare clinical case. Braz Dent J 22(4): 346-350.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet