Complex and Composite Odontomas-Report of Case Series with Literature Review
One can come across various dental anomalies during clinical practice. The diagnosis and management such anomalies is a great challenge for all clinicians. Odontomas are developmental tumor like anomalies seen incidentally on radiographic examination. Odontomas constitute two types one being compound and the other one complex odontome. Hence the present article attempts to show the occurrence of both complex and compound types of odontomas in Indian patients and also discusses in detail about odontomas.
Introduction
Odontomas are the most common odontogenic tumors, which are composed of dental tissues. These tumors are benign and slow-growing, and they can occur in any region of the jaws [1, 2, 3, 4, 5]. The term “odontoma” was first introduced by Broca in 1866 to describe a tumor-like mass composed of enamel, dentin, and pulp tissue [1]. According to the World Health Organization (WHO), odontomas are classified into two types: compound odontomas and complex odontomas. Compound odontomas consist of multiple small tooth-like structures, while complex odontomas are characterized by a disorganized mass of dental tissues [5]. The purpose of this article is present case series of three cases of different odontomas and also to discuss in detail about their etiology, classification, clinical features, radiographic appearance, clinical presentation, histological features and treatment options.
Description of Case Series
Three patients reported to private dental office seeking treatment for their teeth. On radiographic examination odotomas were observed. Detailed history and radiographic examination was carried out. Based on literature search on odontomas, in two patients a diagnosis of complex odontome was made and in one patient compound odontome was done. The detailed description of patients is elaborated in Table 1.
| Case no. | Age (years)/ Gender | Chief complaint | Clinical finding | Radiographic finding | Diagnosis of odontome (Type of odontome) | Treatment rendered |
|---|---|---|---|---|---|---|
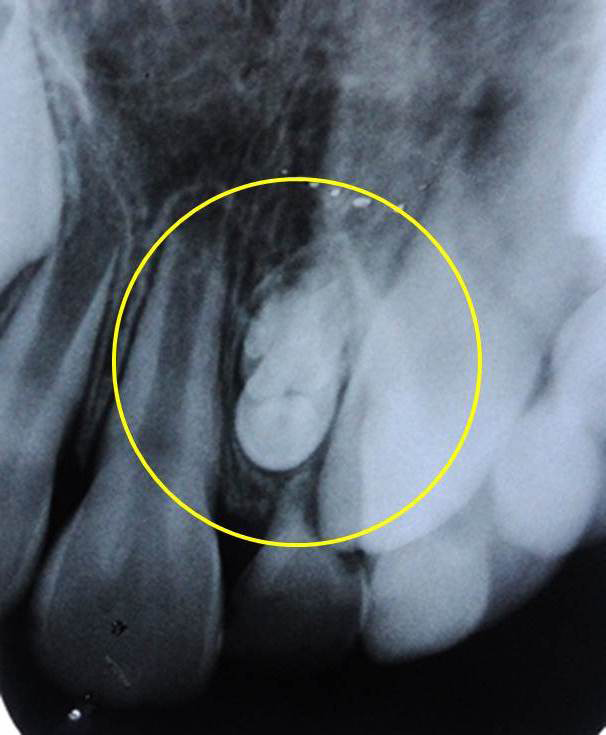
| 1 | 10/F | Delay in eruption of permanent upper front tooth | Retained upper right primary lateral incisor. On left side permanent lateral was erupted | Unerupted right permanent lateral incisor + radiopaque mass seen at the root of primary lateral incisor (Figure. 1) | Complex odontome | Surgical removal of odontome |
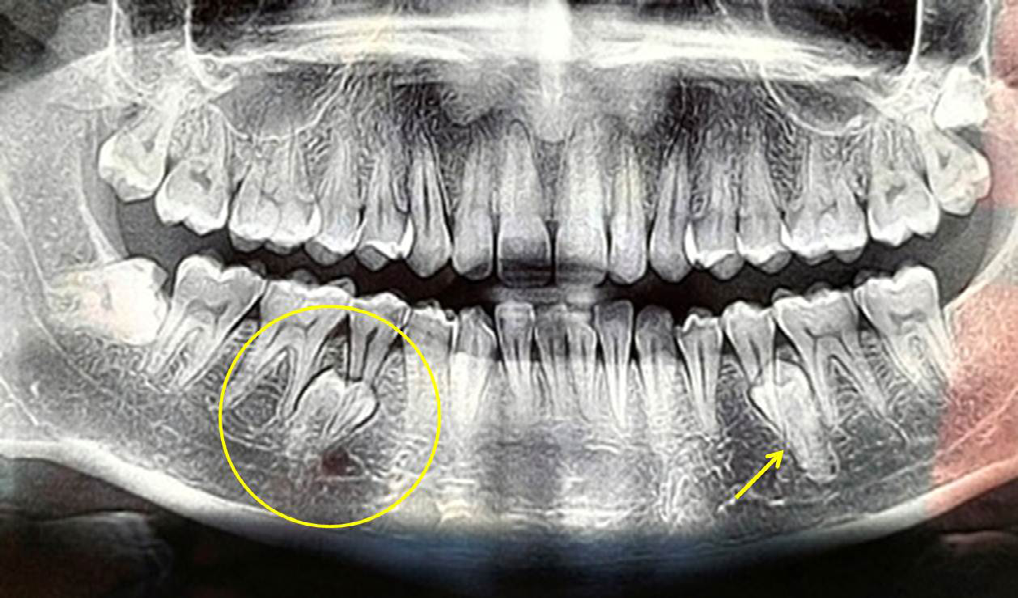
| 2 | 26/M | Pain in right lower back tooth | Impacted right mandibular third molar | Radiographic crown like structure observed at the tip of right second premolar On left side impacted supernumerary second premolar was found (Figure 2) | Compound odontome | No treatment done for odontome as it was asymatomatic |
| 3 | 9/M | Abnormal eruption of upper front tooth | Retained primary left central and lateral incisors | Irregular radiopaque masses found at the root apex of retained primary left central and lateral incisors (Figure 3) | Complex odontome | Extraction of primary central incisor + surgical removal of odontome |
Table 1: Detailed description of cases found with odontomas in Indian patients.
Discussion
Etiology
The etiology of odontomes is not fully understood, but several theories have been proposed to explain their development. One of the most widely accepted theories is the “developmental anomaly” theory, which suggests that odontomes result from disturbances in the development of dental tissues. According to this theory, odontomes occur when the normal process of tooth formation is interrupted, resulting in the formation of abnormal dental tissues. Even in our two cases disturbances in the eruption of permanent teeth was noticed (Figures 1 & 3). In addition to this the theory is supported by the fact that odontomes are often associated with other developmental anomalies, such as impacted teeth, supernumerary teeth, and tooth agenesis [2]. This factor was observed in the second case presented here thereby strongly agreeing with the above assumption. The supernumerary second premolar which was impacted was found along with the compound odontome (Figure 2). Another theory that has been proposed is the “genetic” theory, which suggests that odontomes are inherited in an autosomal dominant manner. Several studies have reported familial cases of odontomes, supporting this theory. However, the exact genetic mechanism underlying the development of odontomes is still unknown [3]. A third theory that has been proposed is the “trauma-induced” theory, which suggests that odontomes result from trauma to the dental tissues. According to this theory, trauma can cause the dental epithelium and/or mesenchyme to proliferate abnormally, resulting in the formation of odontomes. This theory is supported by the fact that odontomes are often found in teeth that have been traumatized [1]. To rule out this factor, history about trauma was elicited in all three patients, which found to be negative. In addition to these theories, several factors have been identified that may increase the risk of developing odontomes. These include radiation exposure, certain medical conditions such as Gardner syndrome, and exposure to certain chemicals such as asbestos [4]. Overall, the etiology of odontomes is complex and multifactorial. Further research is needed to fully understand the underlying mechanisms involved in their development. However, the developmental anomaly theory remains the most widely accepted explanation for the formation of odontomes.

Classification
The World Health Organization (WHO) classifies odontomes into two types, compound and complex odontomes [5]. Compound odontomes are composed of multiple, small, tooth-like structures resembling normal teeth in size and shape. These structures are arranged in a radiating pattern around a central core of dental pulp.
Complex odontomes are composed of an irregular mass of dental tissues and can include structures resembling normal teeth, such as enamel, dentin, and cementum, as well as structures not normally found in teeth, such as bone, cartilage, and fibrous tissue [5]. Based on this classification in first and third case the odontome found was classified into complex odontome and in second case it was diagnosed as a compound odontome.
Clinical Features
It can vary depending on age and gender distribution. Odontomes can occur at any age, but they are most commonly diagnosed in individuals aged 10 to 30 years. There is no gender predilection for odontomes, and they are equally seen in males and females [1, 2, 3, 4, 5, 6]. The clinical features also depends on location. Odontomes can occur in any part of the jaws, but they are more commonly found in the posterior mandible and the anterior maxilla. Compound odontomes are more likely to occur in the anterior maxilla, while complex odontomes are more commonly found in the posterior mandible [1, 7, 8].
In the cases described here, two odontomas occurred in the anterior region of maxilla (Figures 1 & 3) and one in the posterior region of mandible (Figure 2).
Clinical Presentation
Most odontomes are asymptomatic and are discovered incidentally on routine dental radiographs. However, large odontomes can cause facial asymmetry, delayed eruption of teeth, displacement of adjacent teeth or bone expansion. In rare cases, odontomes can cause pain, swelling, and infection [9, 10]. In our all three cases, odontomas were completely asymptomatic and found accidentally on radiographic examination.
Radiographic Features
The radiographic appearance of odontomas varies depending on their type. Odontomes are usually detected on routine radiographic examinations as well-circumscribed radiopaque masses [6]. The radiographic appearance of each type is distinct.
Compound odontomes typically appear as radiopaque masses with a radiolucent rim on intraoral periapical radiographs. They can resemble normal teeth in size, shape, and location, and may even displace adjacent teeth. They often have a lobulated appearance with small radiolucent spaces within the radiopaque mass, giving them a “cluster of grapes” appearance [6, 7, 8]. The small, tooth-like structures within the compound odontome can also be seen as separate entities in the surrounding radiolucent zone. In some cases, compound odontomes can be completely radiopaque, making them difficult to distinguish from other radiopaque structures such as impacted teeth or calculus [6]. Complex odontomes, on the other hand, appear as irregular masses of calcified tissue with a radiopaque or mixed radiopaque- radiolucent appearance. They can vary in size from small nodules to large masses, and are often located in the posterior mandible. They can cause cortical expansion and displacement of adjacent teeth, and may be associated with cystic changes. In some cases, the complex odontome may appear as a diffuse radiopacity without any discernible shape or borders [6].
Histological Features
The histopathological features of compound odontomes are characterized by a mass of miniature teeth, whereas complex odontomes are a disorganized mass of calcified tissue resembling an amorphous conglomerate. Compound odontomes have a central pulp cavity surrounded by enamel, dentin and cementum, while complex odontomes lack a distinct pulp cavity and have a disorganized mass of calcified tissue [7]. Histologically, odontomes can present as mature, immature or dysplastic. Mature odontomes are well-differentiated and composed of normal dental tissues. Immature odontomes are characterized by the presence of irregularly arranged enamel, dentin and cementum, with no clear distinction between them. Dysplastic odontomes are composed of abnormal dental tissues and are associated with impacted teeth, cysts and other odontogenic tumors [7].
Treatment
The treatment of odontomas is generally conservative, and surgical removal is often unnecessary. However, if the odontoma is causing symptoms or interfering with the eruption of adjacent teeth, surgical removal may be indicated. However, the surgical approach may vary depending on the type and location of the odontome [1]. As in our two cases, presence of odontomas hindered the eruption of permanent incisor, surgical removal was carried out. According to a study by Kumar, et al. [8], the majority of odontomes were treated by surgical excision, which was found to be the most effective treatment option. The authors also reported that the prognosis of odontomes was excellent with a low recurrence rate [8]. The odontome was surgically removed using a minimally invasive approach, and the postoperative healing was uneventful. It is stated that the prognosis of odontomes is excellent with a low recurrence rate after surgical excision [9, 10].
Conclusion
Odontomas are unusual developmental dental anomalies that are composed of various dental tissues. These anomalies are commonly found in the jaws and are usually asymptomatic. The diagnosis of odontomas is based on radiographic findings, and treatment is generally conservative. Surgical removal may be indicated in cases of symptomatic or obstructive odontomas.
References
-
Neville BW, Damm DD, Allen CM, Chi AC (2016) Oral and Maxillofacial Pathology. In: 4th (Edn.), St. Louis: Elsevier.
-
Cabov T, Fuchs PN, Julijani A, Ercegovic LC, Marelic S (2021) Odontomas: Pediatric Case Report and Review of the Literature. Acta Clin Croat 60(1): 146-152.
-
Hanemann JA, Oliveira DT, Rados PV, Sant Ana F (2010) Odontogenic Tumors: Analysis of 706 Cases. J Oral Sci 52(4): 581-586.
-
Philipsen HP, Reichart PA (2004) Odontogenic Tumors and Allied Lesions. London: Quintessence Publishing Co Ltd.
-
Shear M, Singh S (2005) Cysts and Odontogenic Tumors. In: Barnes L, Eveson JW, et al. (Eds.) World Health Organization Classification of Tumours. Pathology and Genetics of Head and Neck Tumours. Lyon, France: IARC Press, pp: 306-307.
-
Ali Azhar D, Kota MZ, El-Nagdy S (2013) An Unusual Erupted Complex Compound Odontoma: A Rare Case. Case Rep Dent pp: 106019.
-
Shafer WG, Hine MK, Levy BM (2012) A Textbook of Oral Pathology. In: 6th (Edn.), New Delhi, India, Elsevier.
-
Kumar N, Shrivastava H, Vijay Kumar N, Jadav R (2020) An Unusual Case of Unerupted Composite Complex Odontoma of Eleven-Year-Old Child. Int J Dent Heal Sci 1(05): 0-5.
-
Park JC, Yang JH, Jo SY, Kim BC, Lee J, et al. (2018) Giant Complex Odontoma in the Posterior Mandible: A Case Report and Literature Review. Imaging Sci Dent 48(4): 289-293.
-
An SY, An CH, Choi KS (2012) Odontoma: A Retrospective Study of 73 Cases. Imaging Sci Dent 42(2): 77-81.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet