Pediatric Desmoid-Type Fibromatosis Following Tonsillectomy
Desmoid-type fibromatosis (DTF) is a benign but locally aggressive neoplasm arising from musculoaponeurotic tissues. It could cause significant functional impairments such as dyspnea, dysphagia or other morbidities when it occurs in the head and neck region. Head and neck DTFs are sometimes found in children and cause diagnostic and therapeutic challenge. Here we present a case of 6-year-old male with recurrent airway obstruction 4 years after tonsillectomy to elucidate that prior surgery or trauma may lead to DTF which has been rarely reported previously.
Introduction
Desmoid-type fibromatosis (DTF) is a locally aggressive but non-metastasizing myofibroblast neoplasm with infiltrative nature for local invasion and recurrence [1]. Head and neck DTF represent 12% to 15% of all extra- abdominal desmoid tumors in adults and are sometimes observed in children with an estimated incidence of between 22% and 35% of all extra-abdominal desmoid tumors [2]. Additionally, these tumors have also been demonstrated to be more aggressive in children with higher recurrence rates [3, 4]. They can be associated with significant functional and cosmetic morbidities, attributed to the complicated anatomy of the head and neck region. The majority of head and neck DTF are located in mandible and submandibular area, and less frequently involve the neck, oral cavity, paranasal sinuses, orbital and parapharyngeal space [2]. The etiology of desmoid fibromatosis in childhood is multifactorial and not completely understood. Pregnancy, oral contraceptives and tamoxifen have been associated with the development and evolution of DTF in adults [5, 6]. However, the exact role of hormonal influence is not clear. Additionally, DTF is rarely reported to occur at sites of previous trauma [7]. There is only one case report existed in the literature of DTF following tonsillectomy [8]. It is possible that tonsillectomy potentially implicates the etiology, however, no hypotheses have been made about how physical trauma induces myofibroblast proliferation and DTF formation. We describe an unusual case of DTF in the oropharynx following tonsillectomy that resulted in oropharyngeal stenosis.
A 6-year-old male with medical history of obstructive sleep apnea and tonsillectomy 4 years ago presented with recurrent obstructive sleep apnea symptoms, increased work of breathing and a change in the quality of his voice. The patient’s family history and physical exam were unremarkable. Laboratory tests were with normal limits. Flexible fiberoptic laryngoscopy revealed an exophytic mass from right tonsil occupying the entire posterior oropharynx. Computed tomography scan with contrast showed a large circumscribed mass measuring 3.3 x 4.8 x
4.5 cm centered within the right palatine tonsillar region involving the mucosal space demonstrating mass effect upon the parapharyngeal fat and right carotid artery (Figure 1). Subsequently, the patient was taken to the operating room for debulking of right oropharyngeal mass, and tracheotomy due to worsening airway obstruction.
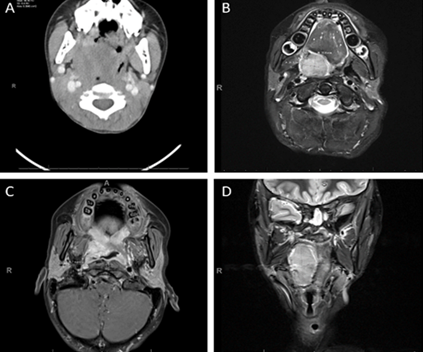
Figure 1: Before debulking, axial CT image of circumscribed mass within the right palatine tonsillar region (A). After debulking, magnetic resonance imaging (MRI) of the mass (B-D). Transverse T2-weighted image (B) and coronal T2-weighted image (C) show the size of the mass, Transverse T1-weighted image shows extension into the right parapharyngeal space, and into the right glossotonsillar sulcus without local infiltration (D).
Pathologic examination of the debulked mass Figure 2 showed broad fascicles of bland-looking spindle cells arranged in uniform direction (“purposeful”) with elongated parallel blood vessels. The spindle cells had myofibroblastic appearance with low nuclear to cytoplasmic ratio and uniformly bland, ovoid nuclei with indistinct nucleoli. By immunostains, the spindle cells are positive for Beta-catenin (nuclear) and SMA with negative stains for cytokeratin AE1/ AE3, DESMIN, S100, CD34, ALK, MyoD1 and MGEN. A Mib-1 stain shows the proliferative rate of approximately 1%. The findings are consistent with desmoid-type fibromatosis.
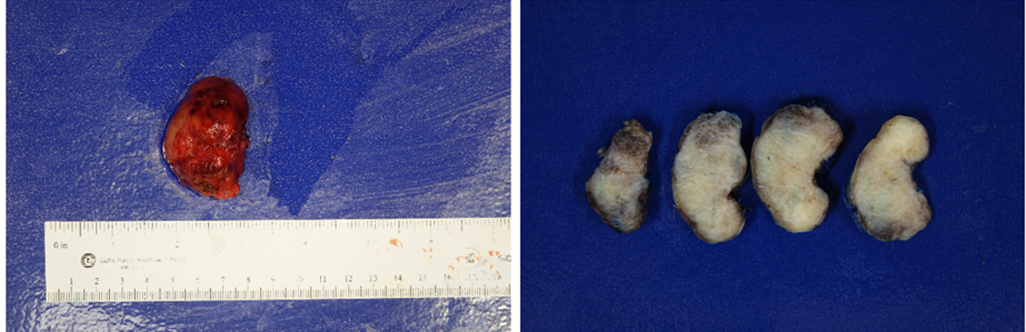
Ten days after debulking, MRI showed a residual solid mass centered in the right palatine tonsil (Figure 1). After confirming the diagnosis, right tonsil mass Figure 3 excision was implemented without complications. The patient recovered well with no sign of recurrence during close follow-up for 34 months.
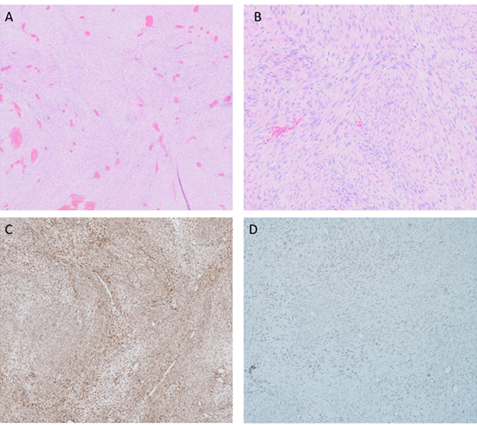
Spindle cell proliferations with bland nuclear features with small and compressed intralesional blood vessels (A&B). The neoplastic cells demonstrated nuclear positivity for beta-catenin and weak positivity for SMA (C&D). (H&E, A, x20; B, x100; β-catenin, C, x20; SMA, D, x20). Figure 2: Histology. Desmoid-type fibromatosis.
Discussion
Desmoid-type fibromatosis also known as aggressive fibromatosis or desmoid tumor, is a rare, locally infiltrative mesenchymal neoplasm with a propensity of local recurrence. DFT may be sporadic or familial in nature. The molecular study has provided an insight in the pathogenesis of both the familial and sporadic DTF. β-catenin is an important molecule with multiple cellular functions including cell adhesion, gene transcription and cell proliferation which is regulated by the adenomatous polyposis coli (APC) gene and the Wnt /β-catenin pathway [9, 10]. The majority of sporadic DTF harbor somatic mutations in exon 3 of the _CTNNB1_gen. It has been reported that T41A and S45F are the most common mutation. While the T41A mutation is significantly more common in abdominal DTF, extra-abdominal DTFs more frequently harbor the S45P alteration [1, 11].
The histologic differential diagnosis of DTF and other monomorphic spindle cell tumors can be difficult given the morphological overlap between these lesions. The histopathologic features such as long, sweeping fascicles of myofibroblasts without substantial cytological atypia and infiltrative growth are essential to diagnose DTF. Nuclear beta-catenin expression (characteristic CTNNB1) is helpful in challenging cases. CTNNB1 mutation analysis may be helpful in small biopsy specimens, when diagnostic morphological features are not readily apparent, and/ or when beta-catenin immunostaining is equivocal or challenging to interpret [1].
Currently, no evidence-based management guidelines are available for children with DTF in the head and neck. Although “wait and see” conservative strategy is proposed by different studies, complete surgical resection with negative margins is the goal of primary treatment because of the high local recurrence rate [12, 13]. However, it is not advocated to achieve negative margin with heavy functional impairment which may not prevent recurrence and may lead to overwhelming socioeconomic burden and psychologic stress to the patient and family members [14]. In our case, the first surgery is to resolve patient’s imminent breath difficulty, confirm diagnosis and prepare for the second surgery which completely resects the tumor without breath and swallow dysfunction.
Conclusion
We reported a rare case of pediatric DTF in the head and neck region following tonsillectomy, suggesting that physical trauma induced myofibroblast proliferation might be an unusual etiology of DTF.
References
-
Fritchie KJ, Van de Rijn M (2020) Desmoid fibromatosis. Soft tissue and bone tumours, WHO classification of tumours series. In: 5th (Edn.), France, 5: 93-95.
-
Risoud M, Mortuaire G, Leroy X, Leblond P, Fayoux P (2017) Desmoid Tumours of the Head and Neck in Children: Review of Management. Eur Ann Otorhinolaryngol Head Neck Dis 134(3): 155-160.
-
Ballo MT , Zagars GK, Pollack A , Pisters PW , Pollack RA (1999) Desmoid Tumor: Prognostic Factors and Outcome After Surgery, Radiation Therapy, or Combined Surgery and Radiation Therapy. J Clin Oncol 17(1): 158- 167.
-
Rutenberg MS, Indelicato DJ, Knapik JA, Lagmay JP, Morris C, et al. (2011) External-Beam Radiotherapy for Pediatric and Young Adult Desmoid Tumors. Pediatr Blood Cancer 57(3): 435-442.
-
Otero S, Moskovic EC, Strauss DC, Benson C, Miah AB, et al. (2015) Desmoid-Type Fibromatosis. Clin Radiol 70(9): 1038-1045.
-
Sharma A, Ngan By,Sandor GKB, Campisi P, Forte V (2008) Pediatric Aggressive Fibromatosis of the Head and Neck: a 20-Year Retrospective Review. J Pediatr Surg 43(9): 1596-1604.
-
Collins BJ, Fischer AC, Tufaro AP (2005) Desmoid Tumors Of The Head and Neck: a Review. Ann Plast Surg 54(1): 103-108.
-
Chang B, Ha JF, Zopf D (2018) Treatment of Extensive Post Tonsillectomy Oropharyngeal Stenosis Secondary to Fibromatosis. Int J Pediatr Otorhinolaryngol 107: 107- 109.
-
MacDonald BT, Tamai K, He X (2009) Wnt/Beta-Catenin Signaling: Components, Mechanisms, and Diseases. Dev Cell 17(1): 9-26.
-
Trufero JM, Bernad IP, Ramon IT, Cubero JH, Cid RP (2017) Desmoid-Type Fibromatosis: Who, When, and How to Treat. Curr Treat Options Oncol 18(5): 29.
-
Trautmann M, Rehkamper J, Gevensleben H, Becker J, Wardelmann E, et al. (2020) Novel Pathogenic Alterations in Pediatric and Adult Desmoid-Type Fibromatosis - a Systematic Analysis of 204 Cases. Sci Rep 10(1): 3368.
-
Kasper B, Baumgarten C, Bonvalot S, Haas R, Haller F, et al. (2015) Management of Sporadic Desmoid-Type Fibromatosis: a European Consensus Approach Based on Patients’ and Professionals’ Expertise - a Sarcoma Patients Euronet and European Organisation for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma Group Initiative. Eur J Cancer 51(2): 127-136.
-
Salas S, Dufresne A, Bui B, Blay JY, Terrier P, et al. (2011) Prognostic Factors Influencing Progression-Free Survival Determined from a Series of Sporadic Desmoid Tumors: a Wait-and-See Policy According to Tumor Presentation. J Clin Oncol 29(26): 3553-3558.
-
Paul A, Blouin MJ, Colin VM, Galmiche L , Coulomb A, et al. (2019) Desmoid-Type Fibromatosis of the Head and Neck in Children: a Changing Situation. Int J Pediatr Otorhinolaryngol 123: 33-37.
- Genomic Landscape of Aggressive Penile Squamous Cell Carcinoma including TERT-p and NOTCH1 Mutations – An Institutional Experience
- Establishment of Baseline Haematological Values for Canine Population in North-Central Nigeria: A Cross-Sectional Study in the Federal Capital Territory
- Biochemical Assessment of Uroliths Extracted in Patients with Urolithiasis in a Tertiary Health Institution
- Update on Gastrointestinal Pecomas: Molecular Pathogenesis and Risk Stratification
- A Comparative Study of Serum C-reactive Protein Level Between Pre-eclampsia and Normal Pregnancy in Tertiary Level Hospital
- From Deformity to Alignment: Clinical Outcomes of the Schnepp Osteotomy in Hallux Valgus in 47 Feet