Some Ideas on How Decision-Making Process on Multiple Causal Interrelations can be understood in General Medicine: "The Auction of Fish"
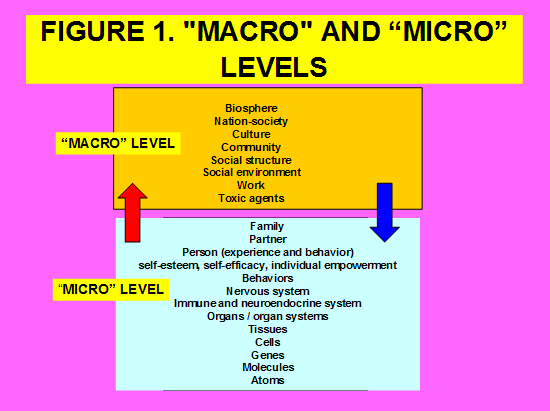
General practitioner (GP) knows the presence of multicausal epidemiological agents at several levels, from the micro level (subatomic particles, atoms, molecules, cells, tissues, organs / organ systems, the nervous system, and the person -experience and behavior) to the macro level (agents that belong to the social structure, structural factors and social and political activities, the social environment, the agents related to work, the toxic agents of the environment, social groups, etc.) and that interventions at the highest possible level will be the most effective (family, community, social structures). Thus, the GP, in each consultation, with each patient, in each health problem that is presented to him, during the interview with the patient, must decide at what level he performs his biopsychosocial intervention. There is a complex mental process or doctor-patient dialogue of understanding and decision-making about the agents of the multi causal that interrelate between the micro and the macro levels. In this article, some ideas are presented on how this process can be understood, and certain constructions are proposed for its practical application. The example or metaphor of the auction convention of the fish market is used to guide the theoretical and pragmatic considerations of the process of interaction of the different heterogeneous causal agents at different levels (macromicro): goods are exchanged under the peculiar protocol of auction of descending offer. The "auction" stops in the price (level and causal agent) that the GP has decided that in that case, in that problem, in that situation, it will be possibly accessible to therapeutic intervention. It can be think a "computerized fish auction protocol" that helps to make and implement decisions in a network of multi-causal agents at macro-micro levels.
Introduction
Epidemiology aims to describe and explain the dynamics of population health, identify the elements that comprise it and understand the forces that govern it, in addition to promoting health, preventing and controlling diseases through knowledge of their causes, in order to intervene in the course of their natural development to modify them [1, 2, 3].
We have been witnessing for some time a change in the concept of epidemiological causality. This change in the way of understanding causality goes from the physiological causality to a circular or ecological or biopsychosocial (BPS) and multiple causality [4]
The cause is not a unidirectional action from the external to the internal or from the internal to the external, but an interaction of the same, that necessarily provokes an effect. Nevertheless we have to assume that it is presented in every integral system as a relationship between the cause and effect which constantly change place or, in the light of the universal connection of the phenomena, cause and effect pass to each other and are transformed into universal connections and interactions. Obviating these interactions contradicts the concrete character of the truth and implies drawing conclusions outside the law of the universal connection of phenomena, which constitutes the result and the manifestation of the universal interaction of all objects, processes and phenomena [5].
However, these models have difficulty in practice to overcome the limitations of the classic or linear causal model, based on an analytical causality, fragmented into isolated parts, which fails to overcome the problem of the dichotomy neither between the individual and the population or social, nor with respect to the hierarchy between macro, meso and micro levels [6, 7].
Since the concept of causality, centered on patients and illnesses, extends to the health-disease process at the population level, this concept at the individual level becomes insufficient to understand the participation of a causality that encompasses, not only the individual or the groups of individuals, but wants to address population health problems [8, 9].
Classical epidemiology, focused on the study of the population from the individual and based on the principles of linear causality, managed to study health Turabian JL. Some Ideas on How Decision-Making Process on Multiple Causal Interrelations can be understood in General Medicine: "The Auction of Fish". Epidemol Int J 2019, 3(2): 000125.
problems considering the individual as part of a population. Because of the development achieved, it dismembered the population in its parts (individuals), and adopted the statistical concept of population as the sum of the parts (individuals), and from this perspective, the causal theory of risk factors assumed the social as one more risk factor. In spite of all the above, the truth is that there is no known causal model capable of linking the causal relationships that occur between the micro (at the individual level) and the macro (at the social level); causality, understood as such, seems to be impossible to be apprehended with the knowledge and tools provided by statistics and the calculation of probabilities. So, there is an expansion of the sociological perspective; the social sciences began to fill the space of understanding of the social [10, 11, 12].
The concept of multi causal agent relationships across the spectrum of hierarchical levels, from micro levels to macro levels in medicine can be compared with the concept of the multi-functional landscape in ecology. Conceptually, self-organization, non-equilibrium, dynamic evolution and hierarchy have been identified as providing an important theoretical grounding for multi-dimensional and integrative landscape studies from a functional perspective. The coupling of horizontal and vertical processes integrates the multi- causality [13].
This analysis of multi causal agents across the spectrum of hierarchical levels can be applied to the level of general medical care. It must be remembered that individual illness depends on relationships and in turn it produces consequences in the social, cultural, economic, environmental and political where it takes place. Therefore, the clinical activity of the general practitioner (GP) should always have a relational dimension even if you work with patients, who at first glance seem to be "alone". The patients are in relational contexts (families, social groups, neighbourhoods) and immersed in social networks that suppose resources, influences and connections [14].
The context includes the pathology, disease, the person and the environment. Each person is part of multiple and interconnected systems, including family, ethnic group, colleagues, social contacts, work, school environment and religion. There is no environment (context) independent of the organism (actor, protagonist, subject, person, "the self"). The multiple connections give rise to sequences of causes in which actors, organisms, etc., both create the systems in which Copyright© Turabian JL.
they are as they are transformed by them. Consequently, mutual causal relationships occur: circular causality; ecological causality [15]. So, analyses of the predictive power of socioeconomic indicators on health run the risk of being fruitless, if interrelations between various indicators are neglected [16].
judgment, it is necessary to use a multi systemic model (Figure 1) that integrates the different areas of the patient's disease and allows the appropriate selection of the path where the treatment could go. A physician with biomedical vision will concentrate on the lowest possible levels of the systemic organization (cells, organs), while a physician with a BPS approach will focus on the highest possible levels of the systemic organization (family, community, social structures...).
The hospital medical specialist sees the disease; the GP sees it, but in its context. To make a clinical
Health is gained and lost in the unstable equilibrium between man and the rapidly changing environment that surrounds him. The individual should not be seen as an isolated element, but in its relations with certain aspects of society: the chain of context-individual interactions, which can be analyzed at its "macro" level (through sociological, epidemiological, economic, historical, or political analysis) in its integration into larger social contexts, and also discovering and analyzing the conditions of micro group functioning (through social psychology, epidemiology, etc.).
That is, the GP to obtain better results should make therapeutic intervention decisions at the highest macro levels that can. We understand by "micro levels", in the consultation of GP, the individual consultation and the relational community of the patient (family, actors and the very close context), and we understand "macro levels" as the part of the geographical community with groups and also community institutions, environmental, social and cultural level [17].
In this scenario, in which GP knows the presence of multi causal epidemiological agents at various levels (from the micro to the macro level), and that interventions at the highest possible macro level will be the most effective, in each consultation with each patient, in each health problem that is presented to him, according to the diverse characteristics that are found, during the interview with the patient, he must decide at what level he performs his BPS intervention. For example, the GP has to realize that decisions at the micro level, as in the prescription of a drug to individual patients, involve systemic changes in a broader system [18].
So, there is a complex mental process of comprehension and decision-making about the multi causal agents that interrelate between the micro and macro levels. This process arises during the dialogue with the patient, and GP must carry out it in a few minutes. This epidemiological process of decision making has important specific characteristics. However, it has not been reflected or conceptualized.
In this article, some ideas are presented on how this process can be understood, and certain constructs are proposed for its practical application. The example or metaphor of the convention of the auction of the fish market is used in the article to guide the theoretical and pragmatic considerations of the competitive process of the different heterogeneous causal agents at different levels (macro-micro).
These epidemiological concepts can often be difficult to explain and understand. In article, these concepts are explained through a metaphor: "the auction of fish." Metaphors enable us to understand something that is unknown in terms of its familiarity. For this reason, they are used frequently in all sciences that adopted common words to name complex realities. The metaphors are analogue devices, used to illuminate reality. Metaphors can simplify expert knowledge, not by ignoring or reducing the complexity, but by providing a point of entry for its comprehension. They are a means of generating ideas, promoting creativity, and constructing concepts and theories. Thinking based on metaphors and comparisons is a way of transforming a concept into something that is so suggestive, interesting, and surprising, that it reaches people more easily [19, 20, 21].
Discussion
The characteristic of family medicine/general medicine is the understanding of the patient and his illness based not only on symptoms and signs, but on the psychological and social factors that relate the patient to his context: that is, with a certain level "macro" [22].
But, The GPs have great difficulty in discovering, using and ultimately intervening on the macro levels, in such a way that this information which is needed to contextualise the information on the pathophysiology and technology, many times is not operative. The "macro" levels, from the individual up (Figure 1) are imagined but not accessible in their entirety [15].
Level "macro"
The GP must know the impact on health caused by structural causes. Many people we call "sick" are because they are poor, because they live in houses with poor conditions, eat poor quality food, work if they do, in depressing jobs, or exist on the margins of survival. That is, there are macro factors. The GP intervention or treatment should include, in addition to actions at the micro levels, actions aimed at structural changes at the macro level that facilitate health. The tasks related to interactions with individuals, at "micro" level, are fundamental in general medicine, but GPs also need to clearly understand their role regarding structural levels: the broad context in which individuals make health decisions. People have limitations in dealing with their personal problems in a way that allows them to control the structural transformations that often lie behind their individual lives [23].
Level "Micro"
It is evident that there is no way to solve social problems from the GP consultation. The GP can not create jobs, mediate a child's school performance, reorder relationships, etc. The external problems (bad housing conditions, loneliness, uprooting, economic difficulties, lack of green areas...), we do not see them as health problems, but as political issues. Thus, stress is diagnosed as irritable bowel, headache or low back pain. Drug addiction or sexual violence is psychiatric diseases. To cure cholera or AIDS or malaria, huge economic resources are used to manufacture a vaccine, when the promotion measures would avoid it. "We control" hypercholesterolemia based on detecting and treating pharmacologically for life millions of previously healthy people who are now sick dependent on the health system. Etc.
From the consultation of the GP cannot solve social problems, but however, can reorient the practice of general medicine towards an ecological or BPS task. It defines the role of the GP to take charge of social problems from the consultation: from to medicalize social relations to socially contextualize medical practice. It is not that the GPs from the consultation, should solve social problems, or that they can or should take into account social problems (a too vague sentence), but that social problems are part of the consultation [23].
So, until what macro level should the GP try to relate the causal network of its patient to achieve the best results in health? How are the causal relationships offered from the micro to the macro levels at the GP consultation?
The factors and multi causal relationships of the "macro" levels (beyond subatomic particles, atoms, molecules, cells, tissues, organs / organ systems, the nervous system, and the person -experience and behavior) are presented to the GP, in each case In each interview with each patient, as if it were a "fish auction", a descending offer auction: From the highest macro levels hierarchically: agents belonging to the social structure, the structural factors and social and political activities, the social environment, agents related to the work, the toxic agents of the environment, social groups, contacts between patients, home care, telecare, foster care, sheltered apartments, temporary residences, homes, day centers and hospitals, NGOs, volunteering, etc., and after, the mental process reaching down to the family ..., and towards the lowest micro levels as intrapersonal aspects such as development of self-esteem, self-efficacy, individual "empowerment", etc., behaviors, nervous system, immune and neuroendocrine system, organs / organ systems, pathophysiological changes, tissues, cells, etc.
A "Fish Auction"
Twice a day in many fishing villages, in Spain and also, around the world, fishermen's fleet catches are sold in the fish market following a long tradition. The fish market is simply where the goods are exchanged under the peculiar protocol of auction of descending offer.
In fish auctions the process is the reverse of the rest of the auctions: you start with the highest price and it goes down... It is a process of "going backwards". It is an auction with price decreasing, that is, the price is initially high but begins to drop quickly and dramatically, until a buyer stops it, making the purchase. Auction begins at the highest price and drops until a bid is made [24].
A bidding round starts when a lot is presented for auction, and ends when it is adjudicated. The lot is presented -by ostentation- by the auctioneer and its FIGURE 2. THE "FISH AUCTION"
| “MA | CRO” LEVEL |
|---|
Biosphere Nation-society
Culture Community Social structure Social environment The "auction" stops in the level and causal agent that the GP has decided, in that case, it will be possibly accessible to therapeutic intervention Work Toxic agents Family Partner Person (experience and behavior) self-esteem, self-efficacy, individual empowerment Behaviors Nervous system Immune and neuroendocrine system Organs / organ systems Tissues Cells Genes Molecules “MICRO” LEVEL Atoms logged information displayed in the display boards: type of good, number of boxes, weight, last paid price, seller's name. When the auctioneer gives the command to start, the bidding clock starts a fast descending pace until a buyer gives a "mine" command that fixes the clock at that instant's apparent selling price.
In the same way, the GP is faced with assessing multiple agents or multi-causal systems in each particular case. The GP mentally uses the process of the "fish auction", either to solve some problems derived from the complexity of the interactions between multiple agents or causes of different levels, or more prosaically, to make acceptable or possible some real applications of decisions in multi causal systems.
"The starting price is high": the GP is alert to the highest causal factors (macro level) of the causal chain in that problem and in that patient, and "quickly this price begins to fall." The GP performs a quick task mental going from the highest macro levels down... and when "he see an interesting price, he mentally press the buy button." The "auction" stops in the price (level of causality) that the GP has decided, in that case, in that problem, in that situation, it will be possibly accessible to therapeutic intervention. If the GP "does not click on the buy button", the "price" continues to fall (that is, the levels of epidemiological causality continue to decrease mentally ...). But it is not convenient to wait too long, because the lower your "price" (your level) the less efficient the GP BPS intervention will be (Figure 2).
Multi causal agents are “exchanged” under the peculiar protocol of auction of descending offer Figure 2: The “Fish Auction” In addition, other social actors can anticipate to the GP and "keep the box of fish he wanted": other social actors have a powerful influence on the problem in that patient and in those circumstances, and when the GP
wants to intervene, their treatment may be useless, or there will be no compliance, or there will be important psycho-social interactions that will cushion or confuse the results... for not "having paid a little more in the auction!" (Because of the GP not having been sufficiently attentive, and having seen intervention possibilities at levels highest of the epidemiological causality network). On the other hand, "the prices depend on how the fishing went, if there is abundance or scarcity, etc." That is, not all cases, nor all health problems, not all associated circumstances, moments, etc. they are the same, and consequently a certain level of intervention will be decided at times and at other times a different level will be decided, according to the possibilities. Therefore, it is a matter of "BPS clinical eye": experience and assessment of the circumstances, to know "what to buy and when is the best time to press the button and keep the fish." Despite its apparent simplicity, the auction is a sophisticated coordination mechanism for the competitive fixation of "prices", in which the interrelations between the multi-causal factors from the macro and micro levels, as if they were intermediaries in the auction that facilitate agreements between buyers and sellers through a highly structured interaction protocol, facilitate GP understanding, the choice of higher level causal factors to perform the intervention and at the lowest possible price (with the least possible difficulties), through a process or mental protocol of discarding inaccessible levels or with a difficult manage by doctor and patient, in each case. Therefore, it is suggested to develop an "electronic auction house" in the general medical history, from which the GP and the patient can "buy" accessible or feasible levels of intervention on certain multi causal agents.
The participants of this "fish auction" are, on the one hand the "sellers": the different macro and micro levels (social structure, structural factors and social and political activities, person, nervous system, organs / organ systems, tissues, cells, organels, molecules, atoms, subatomic particles), and on the other hand the "buyers", who are the doctor and the patient. "Sellers" and "buyers" could interact with "the auction house" through an interface or computer program (software), in which they can assess opportunities and feasibilities [24, 25].
The goods in the auction are the multi-causal agents (Social environment, work, toxic agents, family…, experience, behavior, development of self-esteem, self- efficacy, individual empowerment, behaviors, psychology, immune and neuroendocrine system, pathophysiological changes, genes, etc.). To facilitate recognition of this broader set of causal relations, it can be defined as a potential cause “… any factor, whether event, characteristic, or other definable entity, so long as it brings about change for better or worse in a health condition”, or simply “… something that makes a difference.” That is, this notion of causal or multi causal agent is used to refer to an entity that acts with a purpose or performs an effect, within a social context [12, 26]. Table 1 shows characteristics and properties of causal agents [24].
| Properties | |
|---|---|
| A. Causal agent can be seen as a system | 1. It has a degree of autonomy to determine its behavior2. Interact with humans and other agents3. He perceives the environment and reacts to itAnd, 4. Exhibits goal-directed behavior |
| B. Causal agents exhibit four basic properties | 1. Autonomy: Agents act without human intervention2. Sociability: Agents interact with other agents3- Reactivity: Causal agents can perceive the "world" and react to it4. Situationism: Causal agents may exhibit some objective or behavior oriented |
Table 2: Characteristics and Properties of Causal Agents.
"Buyers" (GP and patient) can certainly have difficulties in evaluating “products”, but an alternative to facilitate this evaluation is to show trade with "products" (causal agents) whose description is standardized in such a way as to allow, to the GP and the patient, all the clarification and differentiation that is needed. The different bidding conventions could be realistic, and they would be implemented and electronically, in an electronic implementation of this "fish auction", as a complement to the electronic medical record [27]. In short, the situations that would occur in the software really would not be so different from those of the electronic auction of a fishing village.
During the doctor-patient dialogue, all the causal interactions of the different macro and micro levels could be assessed. The hierarchical levels and their different multi causal agents can be considered as
2 shows the conditions of this process of doctor-patient dialogue.
| Conditions | Definition | ||
|---|---|---|---|
| 1. Multiplicity | There must be two or more participants (doctor, patient and / or the various causal agents of the hierarchy of levels in each particular case). These "participants" of the biopsychosocial environment exchange the effects that the cause and the intervention produce on the receiver; that is, they exchange reactions or consequences of what each agent says or produces, and the possibilities of intervention | ||
| 2- Sociability | These exchanges of the effects that the cause and the intervention produce in the receiver are subject to a common interaction based on a protocol. The decisions of the participants may change due to dialogical exchange |
Table 3: An Example of the Mental or Computed Process of the Fish Auction.
The protocol, through the notion of "causal agent governor," could ensure that some causal restrictions are understood and correctly applied by the doctor and patient. So, with these two elements (1. levels or institutions mediated by reactions or consequences of causal agents, and 2. governing elements of multi causal agents, a fairly general notion of "causal responsibility", at different macro and micro levels, could be computationally realizable, and it could be formally visualized, for GP and patient, during consultation, showing a sequence "top-down" as in the fish auction, to make a decision [24]. Table 3 and Figure 3 present a typical example of a clinical case where the GP can "stop the auction" at several levels.
| Possible Levels Where | |||
|---|---|---|---|
| Possible Interventions | |||
| General Practitioner (Gp) | |||
| Example | Multi Casual Agents | And Foreseeable | |
| Could Stop "The Auction Of | |||
| Results | |||
| Fish" | |||
| A 42-year-old woman, a kitchen assistant in a hospital, consults her GP for presenting cervical pain and insomnia for months. The course of the interview reveals that the patient suffers from work-related stress and "work harassment" by the supervisor of their work. The patient asks GP for a prescription of a hypnotic, a non- steroidal anti- inflammatory, and sick leave | A. The GP stops "the auction" (from high level to low levels) upon reaching the level of "labour environment and organizational resources." At this level the causative agent would be "psychosocial work environment, psychosocial and organizational factors, particularly high emotional demands, low work-time control and exposure to workplace violence." This causes burnout, stress, and its associated somatic symptoms, such as cervical pain and insomnia and anxiety | A. At this level the causative agent would be "psychosocial work environment, psychosocial and organizational factors, particularly high emotional demands, low work-time control and exposure to workplace violence." This causes burnout, stress, and its associated somatic symptoms, such as Cervical pain and insomnia and anxiety | A. At this level, the intervention could be directed towards labour structures (Labour Inspectorate, Trade Unions...), or towards judicial structures (complaint to the judge, consultation with a labor lawyer ...). By targeting the highest possible hierarchical level of causes, the results of the intervention will be the best possible |
| B. If the GP allows the "auction going to lower more levels", it could stop it at the individual, organ or cell level | B. At this level the causative agent would be factors of personality, difficulty in controlling stress, lack of assertiveness, and / or alteration of cerebral neurotransmitters that provoke anxiety and depression | B. At this causal level, the intervention would include psychological treatment (for example, cognitive-behavioral), psychoactive drugs and non-steroidal anti- inflammatories, as well as cervical RX or consultation with traumatology. The |
Table 4: An Example of the Mental or Computed Process of the Fish Auction.
results would be relatively poor and would include important levels of iatrogenia, health costs and the possibility of a "biological structuring" of the problem and dependence on the health system that can not solve the multi- causal agent alone Table 3: An Example of the Mental or Computed Process of the Fish Auction.
THE "FISH AUCTION"
Community Social environment
| “MACRO | ” LEVEL |
|---|
Table 5: An Example of the Mental or Computed Process of the Fish Auction.
Work
THE EXAMPLE OF TABLE 3
“Psychosocial work environment, psychosocial and organizational factors, particularly high emotional demands, low work-time control and exposure to workplace violence" The GP stops "the auction" Family Person (experience and behavior) Self-esteem, self-efficacy, individual empowerment Behaviors Nervous system Organs / organ systems
| “MICRO | ” LEVEL |
|---|
Cells
The multiple causal agents are shown under the peculiar down- auction bidding protocol Figure 3: An Example of the Process of the "Fish Auction".
Decision making ("the level at which the GP-patient stops the auction") is difficult to achieve, even when the institutions are static. But, it could be seen, with a "fish auction protocol", that intentional formal properties, as well as, those inherent in a given implementation, in a network of multi-causal agents at macro-micro levels, can be understood, and so the protocol is able to effectively try to suggest negotiation lines or points of decision making. Agents in a multi agent system can engage in dialogue. They usually do. But the dialogues they are usually involved in will generally involve actions, and not only propositions, or arguments [24].
The role of the GP is that of agent of change or development, and its interventions are social actions that include interactions between actors in contexts. The role of GP is to help patients-contexts increase their self-esteem and confidence in their own ideas and skills: this is the essence of their therapeutic experience.
The GP is a link in the communication chain, facilitating maximum use of patient-context resources. The performance of the GP should tend to facilitate the "informed choice of the citizen-adult patient", that is, facilitate the development of their ability to choose among a set of alternatives of their competence, but making this provision of information relevant to the patient at macro levels (groups / community), through processes of personal and collective reflection, between different multi causal agents, that allow the conscious and rational taking of complex decisions. The metaphor of the fish auction gives a hint of applicability in which to test simple interactions among possibly complex causal agents [24].
Health outcomes are better in clinical services where patients have more information and therefore a greater sense of control and participation in decisions, compared to traditional ones with little information. In addition, this participation of patients in the decisions of their treatments can mean economic savings. There is evidence that, for certain medical procedures, patients tend to avoid risks and prefer a conservative attitude. The key criterion in decision making in the field of multi causal epidemiological interrelations in the consultation is to support the development of patient autonomy in its context. It is to emphasize the ability of the patient to make decisions about their own health, in their life project, taking into account the significant actors, their points of view / needs, their relationships, their resources, and their environments [23, 29].
We know that the determinants of the disease are BPS; however we are happy to move at the lower micro levels, such as prescribing drugs. We do not usually pay much attention to the macro levels, nor consequently do we help patients for managing their environments in a more effective way. We associate healing with medical treatment at the biological level. Patients improve their health as their lives take on more meaning, and their recovery mechanisms are not inhibited by depression and helplessness; when they learn to solve problems in a critical and reflective way. That is, the higher the intervention in the hierarchical ladder of the macro- micro levels [17, 23].
The corporeity of the multi causal epidemiological agents at micro and macro levels is established through the "nexuses". Working from an epidemiological and BPS perspective supposes to consider the phenomena of health and disease as collective phenomena, emerging from the interrelationship game of economic, educational, political, religious subsystems, etc., that is created in the community. These emerging phenomena can manifest themselves in different ways in the individual, group-family, institutional, community areas [30, 31]. The meaning is not where you start but where it ends. The control and consistency of the process are not where you start, but where it ends. What price can be paid at the auction of fish?
Conclusion
The concept of multi-causal agent across the spectrum of hierarchical levels, from micro levels to macro levels in medicine, includes elements such as self-organization, non-equilibrium, dynamic evolution, hierarchy and the coupling of horizontal and vertical processes. The analysis of the individual includes not only its location as a biographical and physiopathological entity within various interpersonal and biological media, but also the location of those media within the social structures of which they are a part. The life of an individual cannot be properly understood without reference to the institutions within which his biography is developed. There is a complex mental process or doctor-patient dialogue of understanding and decision-making about the multi causal agents that interrelate between the micro and the macro levels.
In this article some ideas are presented on how this process can be understood, and certain constructs are proposed for its practical application. The example of the fish market auction convention is used in the article to guide the theoretical and pragmatic considerations, and a computational version of the fish market could be constructed and used as an aid to decision making for intervention regarding causal agents heterogeneous at different levels (macro-micro).
Thus, one can think of the possible development of simulation models in the interactions of multi causal agents, throughout the hierarchical spectrum from the micro levels to the macro levels, as aids for decision making in general medicine during the consultation, in a way that favours the possibility of more effective and feasible BPS interventions. The model of the "fish auction" would be a possibility, which takes the natural way of processing the information, to make GP decisions.
References
-
Rodriguez Lopez JF, Rodriguez Gonzalez B (2014) Epidemiology: change of paradigms. Medicentro Electron 18(3): 93-99.
-
Lilienfeld AM, Lilienfeld DE (1986) Fundamentos de epidemiologia. Mexico: Addison-Wesley Iberoamericana.
-
Barker DJP, Rose G (1984) Epidemiology in medical practice. Churchill Livingstone, Newyork.
-
Turabian JL (2019) Biopsychosocial Causality in General Medicine: Knot, Ball, and Tangle. Epidemiology International Journal 3(1): 1-9.
-
Tangle Epidemol Int J 3(1): 000121.
-
Sagatovsky VN, Antipov IG (1966) About the correlation between the concepts "cause", "condition", "etiology" and "pathogenesis”. Vestu Akad Med Nauk 21(1): 34-40.
-
Medina Alcoz L (2009) Towards a new general theory of causality in contractual (and extracontractual) civil liability: The doctrine of the loss of opportunities. Rev Resp Civ Seguro (128): 31-74.
-
WHO (2019) Immunization Safety: Training Module. Introduction.
-
Porta M (2006) Constructive conversations about health: policy and values. _In:_ Marinker M (Ed.), Public Health. 2nd(Edn), Oxford: Radcliffe Publishing, pp: 41-50.
-
Grupo de Investigacion de Causalidad (2012) Mecanismo causal. Chile: Universidad de Santiago de Chile.
-
Bacallao Gallestey JC (2012) Modern approaches to bias and causation in epidemiological research. Revista Cubana de Salud Publica 38(5).
-
Morabia A, Porta M (2008) Causality and Epidemiology. Invest Cienc (382): 63-71.
-
Kaufman JS, Poole C (2000) Looking back on "causal thinking in the health sciences". Annu Rev Public Health 21: 101-119.
-
Luo Y, Lu Y, Fu B, Harris P, Wu L, et al. (2019) When multi-functional landscape meets Critical Zone science: advancing multi-disciplinary research for sustainable human well-being. Natl Sci Rev 6(2): 349-358.
-
TurabianJL (2019) Relational Treatment. Chronicle of Medicine and Surgery 3(2): 334-338.
-
Whitfield J (2001) Fish fertilize trees. Wild salmon and trees have a mutually beneficial relationship. Nature.
-
Lahelma E, Martikainen P, Laaksonen M, Aittomaki A (2004) Pathways between socioeconomic determinants of health. J Epidemiol Community Health 58(4): 327-332.
-
Turabian JL, Perez Franco B (2008) Individual health care with community orientation - contextualized care: The figure is the background. Revista Clinica Electronica en Atencion Primaria.
-
Turabian JL (2018) Ecological Implications of Decisions in the Individual Patient: Concentric Health Circles. Chronicle of Medicine and Surgery 2(2): 104-109.
-
Turabian JL, Perez Franco B (2016) Metaphors of the Family Doctor to Learn Family Medicine. New York: Nova Publishers.
-
Casasanto D, de Bruin A (2019) Metaphors we learn by: Directed motor action improves word learning. Cognition 182: 177-183.
-
Colman W (2009) Theory as metaphor: clinical knowledge and its communication. J Anal Psychol 54(2): 199-215.
-
Turabian Fernandez JL, Perez Franco B (2006) The Doctor With Three Heads. Aten Primaria 38(10): 529-588.
-
Turabian JL, Perez Franco B (2001) Actividades Comunitarias en Medicina de Familia y Atencion Primaria. [Community Activities in Family Medicine and Primary Care]. Madrid: Diaz de Santos.
-
Noriega Blanco Vigil PC (1997) Agent Mediated Auctions: The Fishmarket Metaphor. Tesi Doctoral, Universitat Autonoma de Barcelona Facultat de Ciencies.
-
Pearl J (2010) An introduction to causal inference. Int J Biostat 6(2): Article 7.
-
Petersen ML, van der Laan MJ (2014) Causal models and learning from data: integrating causal modeling and statistical estimation. Epidemiology 25(3): 418- 426.
-
Turabian JL (2018) General Medicine-Based Quality Electronic Clinical Record. J Qual Healthcare Eco 1(1): 000106.
-
Lagnado DA, Gerstenberg T, Zultan R (2013) Causal responsibility and counterfactuals. Cogn Sci; 37(6): 1036-1073.
-
Turabian JL (1992) Apuntes, esquemas y ejemplos de participacion comunitaria en la salud. [Notes, schemes and examples of community participation in health]. Madrid: Diaz de Santos.
-
Turabian JL , Perez Franco B (1998) Cual es el sentido de la educacion para la salud y las actividades «comunitarias» en atencion primaria?. Aten Primaria 22(10): 662-666.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria