Sars-Cov-2 Transmission in Family: Study of 18 Families and 51 People without Asymptomatic Secondary Cases in a General Medicine Clinic of Toledo (Spain). Social Factors Lose Importance in Families without Asymptomatic Cases
Background: The presence of asymptomatic secondary cases within the family biases the transmission study, since it is not possible to determine whether these were secondary cases or index cases. Objective: To study the characteristics of the index cases and the contacts in the families that did not have asymptomatic secondary cases. Methodology: An observational and retrospective study of families was conducted from March 15 to December 31, 2020, in which there were at least one primary case or index and one secondary case, and they had no asymptomatic case, in a general medicine office in Toledo (Spain). Results: Eighteen families (50 people) who did not have asymptomatic secondary cases were included, with 18 primary or index cases and 32 cohabitants, of which 26 were secondary cases (with positive PCR) and 6 non-ill (with negative PCR and asymptomatic). The secondary cases only differed statistically significantly from the index cases because they were more frequently female (73% vs. 28%). The healthy cohabitants with respect to the secondary cases in the families were more frequently men (17% vs. 73%), specialized workers (83% vs. 27%), and there was a greater number of people in these families (67% vs. 19% families with => 4 members). None of the characteristics studied in the primary cases was statistically significantly associated with the secondary cases vs. healthy cohabitants. Conclusion: In the context of general medicine in Toledo (Spain), the index cases in families without asymptomatic cases are men who transmit the disease to women, with other men with a higher professional level remaining healthy in the family and living in larger families. With respect to what is known, social factors lose importance in families without asymptomatic cases.
Introduction
Since December 2019, the coronavirus disease 2019 (COVID-19), due to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1, 2], has caused more than 117 million reported cases and more than 2.5 million of deaths to date [3]. COVID-19 is complex, presents variable clinical symptoms and different severity of the disease among patients, although on this spectrum, most of them develop mild symptoms. Several features of SARS-CoV-2 (including high transmissibility, an incubation period with a long-tailed distribution, pre-symptomatic transmission, and the existence of asymptomatic infections which may also contribute to transmission) make accurate detection challenging [4, 5, 6, 7, 8, 9, 10, 11]. Asymptomatic carriers are well documented and have been implicated in COVID-19 transmission. It has been claimed that up to 40% of infections may be asymptomatic [12, 13, 14]. Higher levels of virus can occur in presymptomatic and asymptomatic patients [12, 15]. Because of approximately one in three SARS-CoV-2 infections may be asymptomatic [16] is much more difficult to fight against transmission. Although uncertainty remains about how much they have contributed to the pandemic, mathematical models suggest that 30 to 60 percent of the spread occurs when people have no symptoms [17].
In addition, the duration of the transmissibility of COVIDd-19 and the level of associated contagion has been uncertain [18]. So, the importance of asymptomatic infections in the transmission of SARS-Co-2 has been questioned, highlighting the differences between presymptomatic and asymptomatic patients. But, it seems beyond doubt that these asymptomatic (or initially presymptomatic) infections act as a “silent driver” of the pandemic [19, 20]. On the other hand, it is suspected that home transmission of COVID-19 has contributed to the increase in cases [21, 22]. The cumulative risk to household contacts of an infected person is likely to be substantial during the peak of viral shedding [23, 24]. Most people with COVID-19 receive care at home, which increases the likelihood of exposure for household members. However, less attention has been paid to family members and others who care for people with COVID-19 in the community [25]. However, contact within homes is believed to be responsible for approximately 70% of SARS-CoV-2 transmission when widespread community control measures are in place [26].
On the other hand, homes are ideal settings to assess the transmissibility of a pathogen and the associated determinants of susceptibility and infectivity [27]. But there has been little research that has evaluated the spread of the disease at the family level and the characteristics of primary and secondary cases. Furthermore, the presence of asymptomatic secondary cases confuses the transmission study, since it is only possible to determine the direction of intrafamilial transmission when all cases are symptomatic (and the dates of onset of symptoms are available). Thus, transmission without symptoms poses specific challenges in determining the timing of infections and potential exposures [28, 29]. Consequently, the available clinical-epidemiological data on primary and secondary cases in families are biased as they usually include asymptomatic patients. In this context, a study is presented on the clinical-epidemiological characteristics of primary and secondary cases in families in which there were no asymptomatic cases.
Material and Methods
An observational and retrospective study of 39 families and 132 people, in which there was at least two polymerase chain reaction (PCR) confirmed COVID-19 cases -one primary case or index and one secondary case was conducted March 15 to December 31, 2020, in a general medicine office in Toledo, Spain. The general methodology has already been published [30, 31].
Emplacement
The study was conducted at a general medicine consultation in the Santa Maria de Benquerencia Health Center, Toledo, Spain, was conducted, which has a list of 2,000 patients > 14 years of age (in Spain, general practitioners -GPs- care for people> = 14 years of age, except for exceptions requested by the child’s family and accepted by the GP).
Exclusion of Families with Asymptomatic Cases
From the set of 39 families, those with asymptomatic secondary cases were excluded, defined as family members who, after the appearance of the index case, had positive CRP without the presence of any symptoms.
Diagnosis of COVID-19
The diagnosis was confirmed with PCR oropharyngeal. A confirmed case with active infection was considered to be any person with a clinical picture of sudden onset acute respiratory infection of any severity that occurs, among others, with fever, cough or feeling of shortness of breath. Other symptoms such as odynophagia, anosmia, ageusia, muscle pain, diarrhea, chest pain or headache, among others, were also considered symptoms of suspected SARS- CoV-2 infection according to clinical criteria; and a positive PCR test. People with symptoms compatible with COVID-19
who had already had a PCR-confirmed SARS-CoV-2 infection in the previous 90 days were not considered suspect cases again [32].
Household Contacts
Household contacts were defined as people who shared a residence with the COVID-19 index case. We defined family members as those who had lived with primary cases in a house 4 days before and for more than 24 hours after the primary cases developed illness related to COVID-19. Families with secondary transmission were defined as those where some or all of the family members become infected within one incubation period (2 weeks) of symptom onset of the primary case. The onset date of a confirmed case was defined as the date of the first appearance of self-reported clinical symptoms [33]. Contacts were quarantined shortly after the index case was diagnosed, thereby reducing the risk of transmission (a provision not available in all circumstances).
Incubation Period
The incubation period was determined from confirmed cases that had been exposed only once in transmission chains, whose exposure and onset time were clearly known and in which other factors potentially responsible for their infection were ruled out.
Secondary Attack Rate
Secondary attack rate was defined as the number of new cases divided by the number of people exposed to a primary case. The existence of second or third generation cases was not assessed.
Collected Variables
Data on the index case and close contacts were extracted from the medical records of the general medicine practice. The following variables were collected: age, sex, symptoms, previous contacts, chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and/or can be expected to require a long period of control, observation or treatment ”[34], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD-10 Version: 2019 [35], social-occupancy class (according to the Registrar General’s classification of occupations and social status code) [36, 37], problems in the family context and low income household based on the genogram and in the experience of the GP for their continuity of care and knowledge of the family (genogram is a schematic model of the structure and processes of a family, which included the family structure, life cycle, and family relational patterns. It was understood that “complex” genograms present families with psychosocial problems) [38, 39, 40, 41], and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate ≥ 30 breaths / min; pulse oxygen saturation ≤ 93 % with room air at rest; arterial partial pressure of oxygen/oxygen concentration ≤ 300 mmHg) [33]. To simplify comparison, moderate and severe cases were counted together.
Sample
A convenience sampling was used. The families participating in the study were chosen because they had their members in the same consultation and all medical information was available.
Sample Size
Sample size was calculated for a cohort study, for a Two-sided Significance Level (1-alpha) of 95%, a Power (1-beta,% probability of detection) of 80%, a ratio of secondary / cohabiting cases healthy of 4, a percentage of female secondary cases of 73%, and a percentage of healthy female partners of 17%. These yields a sample size of 28; 21 secondary cases and 7 healthy partners [42].
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test when necessary, (according to the number the expected cell totals) for percentages, and the Student t test for the mean.
Results
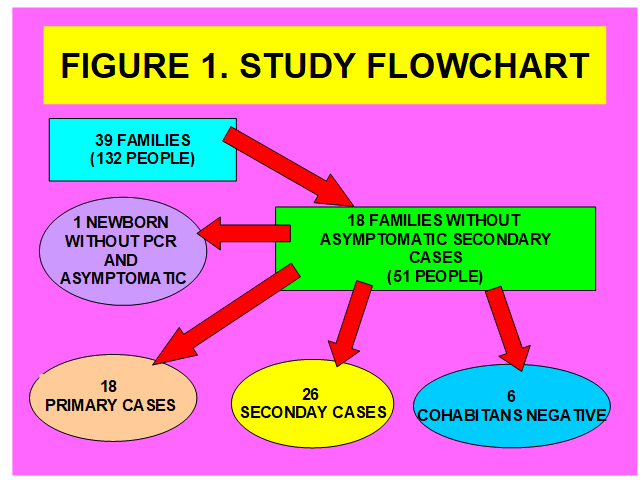
39 families with 132 cohabitants were included, and whose members were treated in the same consultation and all medical information was available. Of these families, 18 did not have asymptomatic secondary cases (obviously there were 18 primary or index cases), which were the ones analyzed in this study, with 51 people (including a newborn, who did not undergo PCR and was asymptomatic). In the 18 families, there were 32 cohabitants without counting the index cases, of which 26 were secondary cases (with positive PCR) and 6 non-ill (with negative PCR and asymptomatic). Figure 1 shows the flowchart of the study. The secondary cases only differed statistically significantly from the index cases because they were more frequently female (73% vs. 28%). The healthy cohabitants with respect to the secondary cases in the families were more frequently men (17% vs. 73%), specialized workers (83% vs. 27%), and there was a greater number of people in these families (=> 4 members) (67% vs. 19%). None of the characteristics studied in the primary cases was statistically significantly associated with the secondary cases vs. healthy cohabitants.
The family size in all of 18 families was 2.83 + -0.78 members (arithmetic mean + -standard deviation). 28% of the primary cases (5/18) referred previous known contact. The incubation period in secondary cases (18 families; n = 26) was 3.88 + -2.55 days (arithmetic mean + -standard deviation). Secondary attack rate (number of secondary cases divided by the number of people exposed to a primary case: 26/32) was 81%.
Table 1 shows the comparison between the characteristics of primary and secondary cases in the 18 families without asymptomatic secondary cases. Table 2 presents the comparison of symptoms between primary and secondary cases in the 18 families without asymptomatic secondary cases. Table 3 presents the comparison of chronic diseases between primary and secondary cases in the 18 families without asymptomatic secondary cases. Table 4 shows the comparison of the variables collected in secondary cases and healthy partners in the 18 families without asymptomatic secondary cases. Table 5 shows the comparison of chronic diseases between secondary cases and healthy cohabitants in the 18 families without asymptomatic secondary cases. And Table 6 shows the comparison between the secondary cases and the healthy cohabitants according to some variables selected from the primary cases in the 18 families.
| Index Cases (Primary) (N=18) | Positive Secondary Cases (Patients) (N=26) | Statistical Significance | |
|---|---|---|---|
| -Woman | 5 (28) | 19 (73) | X2=11.0259. p=.000898. |
| >= 65 years | 0 | 3 (11) | Fisher exact test= 0.2579. NS. |
| < 45 years | 12 (67) | 14 (54) | X2=0.7232. p=.395094. NS. |
| -Workers with some type of specialization | 7 (39) | 7 (27) | X2=0.702. P=.402114. NS. |
| -Students | 3 (17) | 6 (23) | X2 with Yates correction= 0.0191. p=.890075. NS. |
| -Ethnic minority | 3 (17) | 3 (11) | Fisher exact test= 0.676. NS. |
| -Low income household | 3 (17) | 3 (11) | Fisher exact test= 0.676. NS. |
| -Complex family | 2 (11) | 2 (8) | Fisher exact test= 1. NS. |
| -Family with >= 4 members | 4 (22) | 5 (19) | X2 with Yates correction= 0.0191. p=.890075. NS. |
| Symptoms | |||
| -Duration of symptoms in days | 11.44+-7.86 days Range= 0-24 days | 10.53+-10.16 days Range=2-35 days | t= 0.31502. p=.377153. NS |
| (arithmetic mean + -standard deviation and range) | 11.44+-7.86 days Range= 0-24 days | 10.53+-10.16 days Range=2-35 days | t= 0.31502. p=.377153. NS |
| General (Discomfort, Asthenia, Myalgia, fever) | 26 (44) | 23 (32) | X2= 2.0356. p=.153654. NS |
| Respiratory (Cough, Dyspnea, Chest pain) | 13 (22) | 24 (33) | X2= 2.0429. p=.152921. NS |
| ENT (Anosmia / Ageusia, Odynophagia, Rhinorrhea) | 7 (12) | 9 (13) | X2= 0.0839. p=.772022. NS. |
| Digestive (Anorexia, Nausea / Vomiting, Diarrhea, Abdominal pain) | 4 (7) | 6 (8) | X2 with Yates correction= 0.0896. p-value= .764696. NS. |
| Neurological (Headache, dizziness) | 6 (10) | 6 (8) | X2 with Yates correction= 0.1655. p=.684134. NS. |
| Psychiatric (Anxiety, Insomnia) | 2 (3) | 2 (3) | Fisher exact test= 1. NS. |
| Skin (Chilblains, Flictenas, Rash) | 1 (2) | 2 (3) | Fisher exact test= 1. NS |
| Total symptoms * | 59 (100) | 72 (100) | - |
| -Pneumonia | 1 (6) | 3 | Fisher exact test= 0.6337. NS. |
| -Moderate-severe severity | 1 (6) | 3 | Fisher exact test= 0.6337. NS. |
Table 1: ** Comparison between the Characteristics of Primary and Secondary Cases in the 18 Families without Asymptomatic Seconda
( ): Denotes percentages NS: Not significant at p < .05. Table 1: Comparison between the Characteristics of Primary and Secondary Cases in the 18 Families without Asymptomatic Secondary Cases.
( ): Denotes percentages * Patients could have more than one symptom. The percentages are over the total of symptoms of primary cases and of secondary cases NS: Not significant at p < .05. Table 2: Comparison of Symptoms between Primary and Secondary Cases in the 18 Families without Asymptomatic Secondary Cases.
| Chronic Diseases According To Who, Icd-10 Groups | Index Cases (Primary) (N=18) | Positive Secondary Cases (Patients) (N= 26) | Statistical Significance |
|---|---|---|---|
| -Presence of chronic diseases | 9 (50) | 14 (54) | X2= 0.0631. p= .801712. NS. |
| -IV Endocrine | 2 (14) | 13 (36) | X2 with Yates correction= 1.241. p= .265288. NS |
| -V Mental | 3 (22) | 3 (8) | Fisher exact test= 0.3274. NS |
| -VI-VIII Nervous and Senses | 2 (14) | 5 (13) | Fisher exact test= 1. NS. |
| -IX Circulatory system | 2 (15) | 4 (11) | Fisher exact test= 0.6611. NS. |
| -X Respiratory system | 1 (7) | 2 (5) | Fisher exact test= 1. NS. |
| -XI Digestive system | 1 (7) | 3 (8) | Fisher exact test= 1. NS. |
| -XII Diseases of the skin | 0 | 1 (3) | Fisher exact test= 1. NS. |
| -XIII Musculo-skeletal | 1 (7) | 1 (3) | Fisher exact test= 0.4977. NS. |
| -XIV Genitourinary | 2 (14) | 5 (13) | Fisher exact test= 1. NS. |
| TOTAL chronic diseases* | 14 (100) | 37 (100) | - |
Table 2: ** Comparison of Chronic Diseases between Primary and Secondary Cases in the 18 Families without Asymptomatic Secondary
( ): Denotes percentages *Patients could have more than one chronic disease. The percentages are over the total of chronic disease of primary and secondary cases NS: Not significant at p < .05. Table 3: Comparison of Chronic Diseases between Primary and Secondary Cases in the 18 Families without Asymptomatic Secondary Cases.
| Positive Secondary Cases (Patients) (N=26) | Negative Partners (Healthy) (N=6) | Statistical Significance | |
|---|---|---|---|
| -Woman | 19 (73) | 1 (17) | X2 with Yates correction=4.4308. p=.035297. Significant at p<.05. |
| >=65 years | 3 (11) | 0 | Fisher exact test=1. NS |
| <45 years | 14 (54) | 3 (50) | X2 with Yates correction is 0.0804. p-value is .776699. NS. |
| -Workers with some type of specialization | 7 (27) | 5 (83) | Fisher exact test=0.0185. Significant at p<.05. |
| -Students | 6 (23) | 1 (17) | Fisher exact test=1. NS. |
| -Ethnic minority | 3 (11) | 0 | Fisher exact test=1. NS. |
| -Low income household | 3 (11) | 0 | Fisher exact test=1. NS. |
| -Complex family | 2 (8) | 0 | Fisher exact test=1. NS. |
| -Number of people per family | 2.96+-0.82 | 3.83+-0.40 | t-value=-2.49928. p=.009073. Significant at p<.05. |
| -Family with >=4 members | 5 (19) | 4 (67) | Fisher exact test=0.0385. Significant at p<.05. |
| -Presence of chronic diseases | 14 (54) | 2 (33) | X2 with Yates correction=0.2051. p=.650613. NS. |
Table 3: ** Comparison Of The Variables Collected In Secondary Cases And Healthy Partners In The 18 Families Without Asymptomatic
( ): Denotes percentages NS: Not significant at p < .05. Table 4: Comparison Of The Variables Collected In Secondary Cases And Healthy Partners In The 18 Families Without Asymptomatic Secondary Cases.
| Crhonic Diseases According To Who, Icd-10 Groups | Positive Secondary Cases (Patients) (N= 26) | Negative Partners (Healthy) (N=6) | Statistical Significance |
|---|---|---|---|
| -IV Endocrine | 13 (35) | 1 (50) | Fisher exact test= 0.1959. NS. |
| -V Mental | 3 (8) | 0 | Fisher exact test= 1. NS. |
| -VI-VIII Nervous and Senses | 5 (13) | 0 | Fisher exact test= 0.5546. NS. |
| -IX Circulatory system | 4 (11) | 0 | Fisher exact test= 1. NS. |
| -X Respiratory system | 2 (6) | 0 | Fisher exact test= 1. NS. |
| -XI Digestive system | 3 (8) | 1 (50) | Fisher exact test= 1. NS. |
| -XII Diseases of the skin | 1 (3) | 0 | Fisher exact test= 1. NS. |
| -XIII Musculo-skeletal | 1 (3) | 0 | Fisher exact test= 1. NS. |
| -XIV Genitourinary | 5 (13) | 0 | Fisher exact test= 1. NS. |
| TOTAL* | 37 (100) | 2 (100) | - |
Table 4: ** Comparison of Chronic Diseases between Secondary Cases and Healthy Partners in the 18 Families without Asymptomatic S
( ): Denotes percentages *Patients could have more than one chronic disease. The percentages are over the total of chronic disease of primary and secondary cases NS: Not significant at p < .05. Table 5: Comparison of Chronic Diseases between Secondary Cases and Healthy Partners in the 18 Families without Asymptomatic Secondary Cases.
| Positive Secondary Cases (Patients) (N=26) | Negative Partners (Healthy) (N=6) | Statistical Significance | |
|---|---|---|---|
| -Female index case | 6 (23) | 3 (50) | Fisher exact test= 0.314. NS. |
| < 45 years of the index case | 18 (69) | 5 (83) | Fisher exact test= 0.6482. NS. |
| -Workers with some type of specialization of the index case | 9 (35) | 2 (33) | Fisher exact test= 1. NS. |
| -Students of the index case | 4 (15) | 3 (50) | Fisher exact test= 0.101. NS. |
| -Ethnic minority of the index case | 5 (19) | 0 | Fisher exact test= 0.5546. NS. |
| -Low income household of the index case | 4 (15) | 0 | Fisher exact test= 0.5662. NS. |
| -Complex family of the index case | 2 (8) | 0 | Fisher exact test= 1. NS. |
| -Known contact in index case | 8 (31) | 3 (50) | Fisher exact test= 0.3897. NS. |
| -Cough of the index case | 17 (65) | 5 (83) | Fisher exact test= 0.6367. NS. |
| -Diarrhea of the index case | 3 (11) | 0 | Fisher exact test= 0.0711. NS. |
| -With gravity of the index case | 2 (8) | 0 | Fisher exact test= 1. NS. |
Table 5: ** Comparison between Secondary Cases and Healthy Partners According To Some Selected Variables from Primary Cases in th
( ): Denotes percentages NS: Not significant at p < .05. Table 6: Comparison between Secondary Cases and Healthy Partners According To Some Selected Variables from Primary Cases in the 18 Families.
Secondary cases only differed statistically significantly from the index cases because they were more frequently female (73% vs. 28%; X2 = 8.8031. P = .003007). The healthy cohabitants with respect to the secondary cases in the families were more frequently male (17% vs. 73%; X2 with Yates correction = 4.4308. P= .035297), specialized workers (83% vs. 27 %; Fisher exact test = 0.0185), and there were a greater number of people in the family (2.96 + -0.82 vs. 3.83 + -0.40 members; t-value = -2.49928. P= .009073); the 67% vs. 19% families with => 4 members; Fisher exact test = 0.0385). None of the characteristics studied in the primary cases was statistically significantly associated with the secondary cases or healthy cohabitants.
Discussion
There is increasing evidence that SARS-CoV2 has substantial transmission heterogeneity [43, 44]. Analysis of contact tracing data from laboratory-confirmed cases of SARS-CoV-2 infection in Hong Kong between January and April, 2020, revealed that the majority of transmission pairs infected by an identified contact involved household contacts [45]. Viral load in the upper respiratory tract appears to peak at the time of onset of symptoms, and viral transmission begins approximately 2 to 3 days before onset of symptoms [46]. But, the viral shedding kinetics of asymptomatic COVID-19 is not well understood. At the beginning of infection, individuals have similar viral loads regardless of the severity of symptoms, but asymptomatic cases have lower titters at the peak of replication, faster viral shedding, and therefore a shorter infectious period. Current research suggests that infection rates are particularly high in young adults. The evidence on transmission is complicated by the fact that infected children are also less likely to show symptoms than infected adults [47]. Consequently, given the high frequency of asymptomatic cases, especially in children and adolescents, studies on domestic transmission are biased; If only symptoms are looked for to detect initial cases, infected children and young people are not detected because they are less likely to present symptoms [48].
Reported secondary attack rates among so-called high- risk contacts have ranged widely from less than 1% to 55% [49]. Overall, both the observed secondary attack rate and the model-estimated probabilities of infection (with respect to susceptibility) increased with age of household contacts, and female contacts were slightly more susceptible than male contacts [27]. But, the lack of surveillance evidence makes analysis of secondary attack rates (the percentage of cases that result from an infected person within a defined group) for asymptomatic cases extremely difficult.
Gender-based health inequalities also appear to be evident within the COVID-19 pandemic and its aftermath: increased mortality among men and increased morbidity among women [50]. Women are the primary caregiver for home patients with an active COVID-19 infection. On the other hand, although viruses and other pathogens do not affect women and men equally, it seems that there is a set of biological mechanisms that provide women with stronger immune responses to viruses at the cost of an increased risk of autoimmune diseases often later in life [51]. To the extent that family structure and functioning is poorer in poor families, these variables are linked to health [52]. However, the connection between the risk of infection and the number of all people living in the same household is not clear [53].
People who belong to sexual and racial/ethnic minorities are more likely to have underlying health conditions associated with severe COVID-19 [54], and underlying medical conditions related to the severity of COVID-19 include cancer, kidney disease, chronic obstructive pulmonary disease, heart disease, obesity, smoking, diabetes, asthma, hypertension, and stroke. COVID-19 shows a spectrum of severity and lethality characterized by a marked age gradient. Generally, infections younger than 20 years have mostly mild or no symptoms, while older people are at increased risk of developing severe symptoms, such as respiratory failure, multi-organ dysfunction, and death [55, 56]. Cross-protection induced by exposure to endemic human coronaviruses may explain the low frequency of severe COVID-19 symptoms in people younger than 20 years [57].
Our study, without asymptomatic cases, found that the index cases in families are men who transmit the disease to women, with other men with a higher professional level remaining healthy in the family and living in larger families. With respect to what is known, social factors lose importance in families without asymptomatic cases. In the same population of our study, it had been previously reported, in a family transmission study where asymptomatic cases were included, that Family secondary cases compared to primary ones were statistically significantly more women (73% vs. 51%), younger (average 32 years vs. 39 years), more students and a lower socio-occupational level, more asymptomatic (36% vs. 8%), with shorter duration of the symptoms (mean 5 vs. 12 days), and less severe ( 96% mild vs. 85%). Thus, studies of transmission in families, which include asymptomatic cases, suggest that psychosocial factors can be more important vs. biological ones in secondary contagion within families.
In this study, in the analysis of families without asymptomatic cases (which could confuse whether they were primary or secondary) when comparing the results with families with symptomatic cases, it suggests that studies that include asymptomatic cases skew the characteristics of the secondary cases towards younger ages, students, lower socio-occupational level, and lower severity; in a sense, in studies that include asymptomatic cases there is a bias towards a greater importance of social factors vs. the biological ones: It seem that social factors are more linked to asymptomatic cases.
Study Limitations
- Our study, although in our opinion it is novel, has some limitations that must be taken into account: The sample of included families was not a probabilistic sample; it was a convenience sample (The families participating in the study were chosen because their members were treated in the same consultation and all the medical information was available). However, there are no logical reasons to think that the current research sample was different from the ideal, randomly selected sample (from the entire population), nor that there might be under- or over- represented people in the sample. Furthermore, by being able to compare the results with previous studies in the same population, it reinforces the value of the results.
- The small sample size. Although the sample size met the requirements for some variables, it did not do so for all of them.
Conclusion
In the context of general medicine in Toledo (Spain), the index cases in families without asymptomatic cases are men who transmit the disease to women, with other men with a higher professional level remaining healthy in the family and living in larger families. With respect to what is known, social factors lose importance in families without asymptomatic cases. In summary, when it is compared the results of families with symptomatic cases with families without asymptomatic cases (that is, without the confounding factor that the presence of asymptomatic cases supposes in the transmission dynamics and in the characteristics of primary and secondary cases) it seems that these asymptomatic cases skew the characteristics of secondary cases towards younger ages, students and lower socio-occupational level.
References
-
(2020) Naming the coronavirus disease (COVID-19) and the virus that causes it. WHO.
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med 382(8): 727-733.
-
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins. The Center for Systems Science and Engineering (CSSE) at JHU.
-
Harris BHL, Zuhair M, Di Giovannantonio M, Rosadas C, Khan M, et al. (2021) Asymptomatic Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in a Rehabilitation Facility: Evolution of the Presence of Nasopharyngeal SARS-CoV-2 and Serological Antibody Responses. J Infect Dis 223(2): 192-196.
-
Russell TW, Golding N, Hellewell J, Abbott S, Wright L, et al. (2020) Reconstructing the early global dynamics of under-ascertained COVID-19 cases and infections. BMC Med 18: 332.
-
Abbott S, Hellewell J, Munday J (2020) The transmissibility of novel Coronavirus in the early stages of the 2019–20 outbreak in Wuhan: Exploring initial point-source exposure sizes and durations using scenario analysis. Wellcome Open Res 5: 17.
-
Tindale LC, Coombe M, Stockdale JE, Garlock ES, Lau WYU, et al. (2020) Transmission interval estimates suggest pre-symptomatic spread of COVID-19. Medrxiv.
-
Kucharski AJ, Russell TW, Diamond C, Liu Y, Edmunds J, et al. (2020) Early dynamics of transmission and control of COVID-19: a mathematical modeling study. Lancet Infect Dis 20(5): 553-558.
-
Hellewell J, Abbott S, Gimma A, Bosse NI, Jarvis CI, et al. (2020) Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob Health 8(4): 488-496.
-
Bai Y, Yao L, Wei T, Tian F, Jin DY, et al. (2020) Presumed asymptomatic carrier transmission of COVID-19. JAMA 323(14): 1406-1407.
-
Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, et al. (2020) The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med 172(9): 577-582.
-
Oran DP, Topol EJ (2020) Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann Intern Med 173: 362-367.
-
Warren EL (2020) Why Do Some People Weather Coronavirus Infection Unscathed?. Medscape.
-
Pan Y, Yu X, Du X, Li Q, Qin X, et al. (2020) Epidemiological and Clinical Characteristics of 26 Asymptomatic Severe Acute Respiratory Syndrome Coronavirus 2 Carriers. J Infect Dis 221(12): 1940-1947.
-
Lee S, Kim T, Lee E, Lee C, Kim H, et al. (2020) Clinical course and molecular viral shedding among asymptomatic and symptomatic patients with SARS-CoV-2 infection in a community treatment center in the Republic of Korea. JAMA Intern Med 180(11): 1447-1452.
-
Oran DP, Topol EJ (2021) The Proportion of SARS-CoV-2 Infections That Are Asymptomatic: A Systematic Review. Ann Intern Med.
-
Apuzzo M, Gebrekidan S, Kirkpatrick DD (2020) How the World Missed Covid-19’s Silent Spread. Symptomless transmission makes the coronavirus far harder to fight. But health officials dismissed the risk for months, pushing misleading and contradictory claims in the face of mounting evidence. New York Times.
-
Kim MC, Cui C, Kweon OJ, Jung SY, Park MS, et al. (2021) Duration of Culturable SARS-CoV-2 in Hospitalized Patients with Covid-19. N Engl J Med 384: 671-673.
-
Nogrady B (2020) What the data say about asymptomatic COVID infections. Nature.
-
Turabian JL (2020) The Importance of Asymptomatic Coronavirus Disease-19 Patients: Never Trust a “Silent Customer”. J Community Prev Med 3(2): 1-7.
-
Turabian JL (2021) Asymptomatic Family Cases of Covid-19. Archives of Medicine 17(1): 1-3.
-
Jing QL, Liu MJ, Zhang ZB, Fang LQ, Yuan J, et al. (2020) Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: a retrospective cohort study. Lancet Infect Dis 20(10): 1141-1150.
-
Rosenberg ES, Dufort EM, Blog DS, Hall EW, Hoefer D, et al. (2020) COVID-19 Testing, Epidemic Features, Hospital Outcomes, and Household Prevalence, New York State- March 2020. Clin Infect Dis 71(8): 1953-1959.
-
Wu J, Huang J, Tu C, Bi C, Chen Z, et al. (2020) Household Transmission of SARS-CoV-2, Zhuhai, China, 2020. Clin Infect Dis 71(16): 2099-2108.
-
Little P, Read RC, Amlot R, Chadborn T, Rice C, et al. (2020) Reducing risks from coronavirus transmission in the home-the role of viral load. BMJ 369: 1728.
-
Haroon S, Chandan JS, Middleton J, Cheng KK (2020) Covid-19: breaking the chain of household transmission. BMJ 370: 3181.
-
Li F, Li YY, Liu MJ, Fang LQ, Dean NE, et al. (2021) Household transmission of SARS-CoV-2 and risk factors for susceptibility and infectivity in Wuhan: a retrospective observational study. Lancet Infect Dis 21(5): 617-628.
-
Rasmussen AL, Popescu SV (2021) SARS-CoV-2 transmission without symptoms. Science 371(6535): 1206-1207.
-
Turabian JL (2021) COVID-19 Asymptomatic Cases in the Family Distort the Characteristics of True Primary and Secondary Cases. Epidemol Int J 5(1): 1-12.
-
Turabian JL (2021) A Longitudinal Study of SARS- CoV-2 Secondary Infection Risks in Family Members: Psychosocial Factors May be More Important than Biological Ones. Epidemol Int J 5(1): 1-11.
-
Turabian JL (2021) SARS-COV-2 infection prevalence and characteristics in domestic contacts: Study of 39 families and 132 people in a general medicine clinic in Toledo (Spain): Implications for the general practitioners. Int J Epidemiol Health Sci 2(1): 07.
-
(2020) Strategy For Early Detection, Surveillance And Control Of Covid-19. Ministry of Health. Spain.
-
Mao S, Huang T, Yuan H, Li M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20: 1525.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The C.V. Mosby Company.
-
(2019) International Statistical Classification of Diseases and Health-Related Problems. ICD-10 Version, WHO.
-
(1986) The Classification and Analisis of General Practice Data. Royal Collage of General Practitioners.
-
Donaldson RJ, Donaldson LJ (1983) Essential Comunity Medicine. Lancaster: MTP Press.
-
Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci. 3(1).
-
Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs 26(4): 287- 293.
-
Watts C, Shrader E (1998) The genogram: a new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy Plan 13(4): 459-464.
-
McIlvain H, Crabtree B, Medder J, Stange KC, Miller WL (1998) Using practice genograms to understand and describe practice configurations. Fam Med 30(7): 490- 496.
-
Open Source Epidemiologic Statistics for Public Health.
-
Moschetti J (2020) Massive screening: Professor Antoine Flahault is “not convinced. Medscape.
-
Liu Y, Eggo RM, Kucharski AJ (2020) Secondary attack rate and superspreading events for SARS-CoV-2. Lancet 14: 395(10227).
-
Carvalho T (2020) COVID-19 clusters. Nat Med 26(12): 1806.
-
He X, Lau EHY, Wu P, Deng X, Wang J, et al. (2020) Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat Med 26(5): 672-675.
-
Nogrady B (2021) Why aren’t kids getting vaccinated? They are at lower risk of serious illness from covid-19, and there are ethical issues around vaccine trials in children-but the delay may lead to problems. MIT Technology Review.
-
Hanage WP (2020) COVID-19 Data Prospecting: Many Reasons Reopening Schools Can Go Wrong. Medscape.
-
Koh WC, Naing L, Chaw L, Rosledzana ML, Alikhan MF, et al. (2020) What do we know about SARS-CoV-2 transmission? A systematic review and meta-analysis of the secondary attack rate and associated risk factors. PLoS One 15(10).
-
Bambra C, Albani V, Franklin P (2021) COVID-19 and the gender health paradox. Scand J Public Health 49(1): 17- 26.
-
Offord C (2021) Sex Differences in Immune Responses to Viral Infection. Stronger interferon production, greater T cell activation, and increased susceptibility to autoimmunity are just some of the ways that females seem to differ from males. The Scientist.
-
Booysen F, Botha F, Wouters E (2021) Conceptual causal models of socioeconomic status, family structure, family functioning and their role in public health. BMC Public Health 21: 191.
-
Heuvel MVD (2020) Heinsberg study in the “preprint”: High number of unreported infections, death rate only 0.36%-does this apply to the whole of Germany?. Medscape.
-
Heslin KC, Hall JE (2021) Sexual Orientation Disparities in Risk Factors for Adverse COVID-19-Related Outcomes, by Race/Ethnicity-Behavioral Risk Factor Surveillance System, United States, 2017–2019. MMWR Morb Mortal Wkly Rep 70(5): 149-154.
-
(2020) Coronavirus Disease 2019 in Children - United States, February 12-April 2, 2020. MMWR Morb Mortal Wkly Rep 69(14): 422-426.
-
Wu Z, McGoogan JM (2020) Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 323(13): 1239-1242.
-
Pinotti F, Wikramaratna PS, Obolski U, Paton RS, Damineli DSC, et al. (2021) Potential impact of individual exposure histories to endemic human coronaviruses on age-dependent severity of COVID-19. BMC Med 19(1): 19.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria