Early Multidrug Treatment of SARS-Cov-2 (COVID-19) and Decreased Case Fatality Rates in Honduras
Introduction: Within 2 months of first detection of SARS-CoV-2 in Honduras, its government promoted nationwide implementation of multidrug COVID-19 inpatient and outpatient protocols. This was associated with a case fatality rate decrease from 9.33% to 2.97%. No decrease was seen in Mexico, a similar Latin-American country that did not introduce multidrug treatment protocols at that time. Objective: The primary objective of the study was to use statistical process control to assess the likelihood that the decrease in case fatality rate in Honduras was due to chance, using Mexico as a control country. Methods: Fourteen day running average COVID-19 case fatality rates in Mexico and Honduras were used to create Shewhart control charts during the first 6 months of the epidemic. The date of implementation in Honduras of the inpatient and outpatient multidrug COVID-19 protocols were plotted on control charts, with a Mexican COVID-19 case fatality control chart as a comparison. Results: The case fatality rate for COVID-19 in Honduras dropped below the lower control limit 9 days after implementation of an inpatient multidrug inpatient protocol, from an average 9.33% case fatality rate to 5.01%. The Honduran COVID-19 case fatality rate again dropped below the 5.01% control chart limit 17 days after implementation of an outpatient multidrug protocol, to an average 2.97%, suggesting statistically significant anomalies. No control limit anomalies were seen during the same period in neighbouring Mexico. Conclusion: There was an association between both inpatient and outpatient multidrug treatment of COVID-19 and decreased fatality rates in Honduras.
Introduction
Honduras is a low middle-income country with 66 percent of its population in poverty in 2016, and with 20 percent of Hondurans living in extreme poverty-that is, on less than US$1.90 per day [1]. Honduras experienced its first case of COVID-19 documented by SARS CoV-2 RT-PCR testing on March 10, 2020[2]. As the COVID-19 pandemic unfolded in New York in the spring of 2020, Honduras faced the potential collapse of its health care system from COVID-19, with but 19 critical care physicians and 125 intensive care unit (ICU) beds to serve a population of 9.9 million [3]. By contrast, New York City with a population of 8.9 million had 1060 critical care physicians and 1644 ICU beds [4]. Still recovering from a recent Dengue epidemic, the Honduran government responded proactively to the COVID-19 pandemic based on the recommendations of its critical care and infectious disease consultants. Honduran physicians theorized that a multi-mechanism approach (MMA) to treating COVID-19 could block the inflammation, immune system disruption, and hypercoagulation that initial reports suggested as the cause for mortality from SARS CoV-2 infections. They created the MMA protocol based on the hypothesis that COVID-19 mortality resulted less from direct viral infection and more from the self-perpetuating cytokine storm and thrombosis triggered by the virus that, once triggered, increased independently of viral replication. Given Honduras’ limited resources, the MMA protocol used repurposed, inexpensive medications already proven safe and effective for other indications, for which in vitro and clinical evidence suggested clinical efficacy against COVID-19.
| Intervention | Purpose | Dose | Duration | Comments | |||
|---|---|---|---|---|---|---|---|
| Inpatient (CATRACHO) | Dexamethasone | Anti-inflammatory | 0.2-0.4 mg/kg IV daily | 5-7 days | May substitute methylprednisolone (1-2 mg/kg/day divided every 6 hours) | ||
| Inpatient (CATRACHO) | Colchicine | Anti-inflammatory | 1 mg orally every 12 hours first day, then 0.5 mg orally every 12 hours | 5 days | Adjust for renal function | ||
| Inpatient (CATRACHO) | Tocilizumab | Anti-inflammatory rescue | 4-8 mg/kg IV | Once. May repeat X 1 in 3 days if inadequate response | Second dose for worsening acute phase reactants and ventilation parameters | ||
| Inpatient (CATRACHO) | Ivermectin | Immunomodulation (IL-6 inhibition) | 200 micrograms/kg orally on a full stomach | 5 days | |||
| Inpatient (CATRACHO) | Zinc | Anti-viral | 50 mg q 12 hours | 10 days | |||
| Inpatient (CATRACHO) | Azithromycin | Anti-viral | 500 mg po q day | 5 days | |||
| Inpatient (CATRACHO) | Low molecular weight heparin | Anticoagulation | 1 mg/kg every 12 hours subcutaneously | 14 days | Alternative apixaban or rivarixoban orally | ||
| Inpatient (CATRACHO) | Hi flow oxygen and pronation | Oxygenation | Pulse oximetry above 92% | Until no longer required | |||
| Inpatient (CATRACHO) | MAIZ | Outpatient | Sodium hypochlorite 0.25% + Hydrogen peroxide | Anti-septic | 3 mouthwashes (without swallowing) and 2 nasal sprays every 6 hours | 7 days | |
| Azithromycin | MAIZ | Outpatient | Anti-viral | 500 mg po q day | 5 days | ||
| Ivermectin | MAIZ | Outpatient | Immunomodulation (IL-6 inhibition) | 200 micrograms/kg orally on a full stomach | 5 days | ||
| Zinc | MAIZ | Outpatient | Anti-viral | 50 mg q 12 hours | 10 days | ||
| MAIZ -AA | MAIZ | Outpatient | Prednisone | Anti-inflammatory | 1-1.5 mg/kg daily | 7 days | Additional 3 days per inflammatory markers |
| MAIZ -AA | Colchicine | Outpatient | Anti-inflammatory | 1.5 mg orally first dose, then 0.5 mg orally every 12 hours | 7 days | As tolerated | |
| MAIZ -AA | Rivaroxaban | Outpatient | Anticoagulation | 20 mg po q day | 14 days | Alternative apixaban 5 mg q 12 hrs orally |
Table 1: Inpatient and Outpatient Medication Protocols for Honduras’ Multi-Mechanism Approach to COVID-19 Therapy.
The MMA protocol also optimized oxygenation with high- flow O2 therapy and self-pronation rather than mechanical ventilation whenever possible, conserving limited intensive care resources. In mid-April 2020, Honduran physicians began treating COVID-19 patients with the MMA protocol immediately upon admission to the hospital, as well as in outpatient clinics immediately on diagnosis with COVID-19. Decreased morbidity and mortality were observed in patients receiving the MMA inpatient protocol, documented in a peer-reviewed retrospective cohort study that showed a decrease ICU length of stay by 5.4 days with a trend towards decreased mortality [5]. The MMA protocol [6] (Table 1) medications have yet to be labelled by the FDA as effective for COVID-19 therapy, although they have been labelled as safe for non-COVID-19 indications.
After the initial promising results, the protocol was promoted by the Honduran Health Department on May 3, 2020, in a nationally televised educational program for health care professionals, detailing recommendations on treating COVID-19 with MMA for inpatients and outpatients. The Honduran Health Department hosted additional Zoom™ video meetings to educate clinicians throughout the month of May 2020. The inpatient MMA protocol was marketed as “CATRACHO,” an acronym of the protocol’s components that references General Florencio Xatruch, the Honduran leader who defeated aggressors from the U.S. in 1856. Hondurans refer to themselves as “catrachos,” a Nicaraguan pronunciation of the Catalan surname Xatruch [7].
As the pandemic in Honduras spread, the number of COVID-19 outpatients overwhelmed existing clinic capacity. The Honduran government elected to create “medical brigades” that performed home visits, identifying underserved COVID-19 patients early and immediately dispensing outpatient protocol medications. The initial 7-day course of outpatient therapy was pre-packaged as “MAIZ” (Spanish for “corn,” Honduras’ staple food), an acronym for mouthwash of sodium hypochlorite and hydrogen peroxide, azithromycin, ivermectin, and zinc. Patients that continued to have COVID-19 symptoms after 7 days were prescribed an enhanced outpatient therapy, “MAIZ-AA”, which added anti- inflammatory medications (colchicine and prednisone) and an anticoagulant (rivaroxaban). Within three months after the initiation of the MMA protocols in Honduras, clinicians worldwide began to publish reports supporting the efficacy against SARS CoV2 infections of the main components of the MMA protocols: namely colchicine, ivermectin, tocilizumab, dexamethasone, and full dose heparin [8, 9, 10, 11, 12, 13].
Methods
Due to the urgency of the pandemic and the paucity of local healthcare resources, it was impractical to prospectively organize randomized, controlled, double blinded trials to evaluate the MMA protocol’s efficacy against COVID-19 prior to its implementation in Honduras. An alternative methodology, statistical process control (SPC), is a well validated approach initially developed to improve manufacturing outcomes at the Bell Laboratories about a century ago. SPC has gained increasing acceptance in health care applications [14]. It is less resource intensive, achieving statistical significance through frequent measurements over time rather than by large patient sample sizes, and represents results in easy to comprehend control charts [15]. For this reason, SPC tools have been widely used for monitoring the evolution and impacts of the COVID-19 pandemic in the past two years [16]. Shewhart control charts were used to compare COVID-19 case fatality rates in Honduras (Figure 1A) with those in a control country, Mexico (Figure 1B), whose population has comparable age, demographics, and socio-economic status, has a similar climate, and experienced nearly identical case fatality rate increases during its initial exposure to SARS CoV2. The case fatality data came from the publicly available World Health Organization online dashboard [17]. In each control chart, the black dot represents the 14-day running average case fatality rate calculated at each day, while the red solid and dashed curves represent the upper and lower, respectively, control limits with a confidence level of 95%.
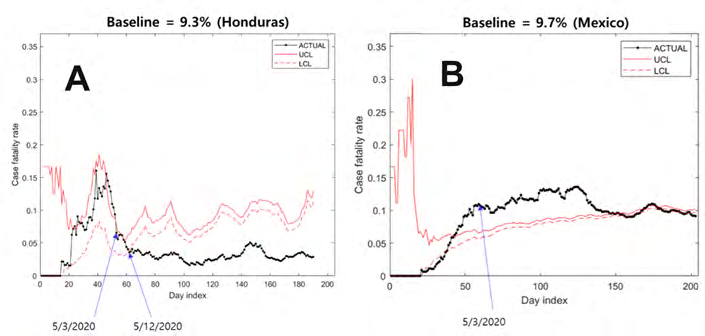
Figure 1A-B: Shewhart control chart upper and lower control limits for 14 day rolling average case fatality rate. Control limits were estimated using a baseline which was the average case fatality as of May 3, 2020 for Honduras (A) and Mexico (B); and as of June 10, 2020 for Honduras (C).
The control limits in the Shewhart control chart were obtained by Monte Carlo simulation which is often used for control limit estimation when the distribution of the statistic under study is unknown or complex [18]. The simulation was based on an assumption that patients could die at any time within a 14-day period following his/her positive test, which is consistent with the doctors’ experience. Given a baseline case fatality rate, the number of deaths at each day was simulated and its 95% confidence interval was obtained by repeating the simulation for 100000 times. The control limits, which are the upper and lower bounds of the confidence interval, represent the range of the 14-day running average case fatality rate when the true (or population) case fatality rate equals the baseline. The control charts were made in Matlab 2020 software. Any anomaly in a control chart, i.e., a point falling outside the control limits, indicates statistically significant evidence that the true case fatality rate is different from the baseline; in other words, the difference cannot be explained by chance. Specifically, it suggests that the true case fatality rate is higher or lower than the baseline if the upper or lower control limit is violated.
Results
On May 3, 2020, the Honduran Department of Health encouraged physicians to implement the MMA protocol (Table 1) for inpatients (CATRACHO protocol) immediately on hospital admission, and for outpatients (MAIZ protocol) immediately on diagnosis. If outpatients continued to have symptoms after 7 days, the “MAIZ-AA” anti-inflammatory and anticoagulant medications (colchicine, prednisone and rivaroxiban) were added. The Honduran COVID-19 case fatality rate dropped below the Shewhart control chart’s lower control limit on May 12, 2021 (Figure 1A), nine days after the publication of the MMA recommendations. The baseline case fatality rate of 9.3% used to calculate the control limits was the average case fatality rate in Honduras on May 3, when the MMA inpatient and outpatient protocols were first implemented. Synchrony exists between the case fatality rate control chart anomaly in Honduras and the dates on which its government published the MMA COVID-19 treatment protocol. Figure 1C shows that in Honduras, the case fatality rate dropped below the Shewhart control limit a second time 17 days after an outpatient protocol (Table 1) was adopted on June 10, 2020, when volunteer medical brigades went out into the community to identify COVID-19 cases and distributed packets containing the early antiviral medication regimen.
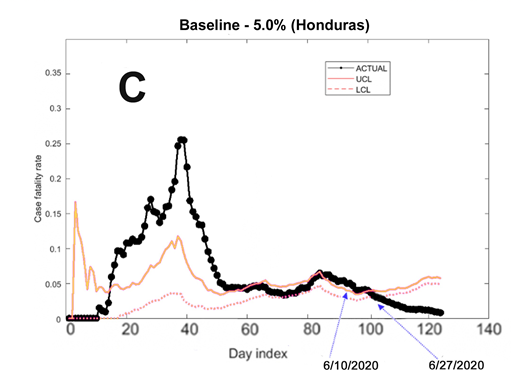
Figure 1C: Shewhart control chart upper and lower control limits for 14 day rolling average case fatality rate. Control limits were estimated using a baseline which was the average case fatality as of May 3, 2020 for Honduras (A) and Mexico (B); and as of June 10, 2020 for Honduras (C).
Discussion
The initial implementation of the MMA protocols was associated with a 6.36% decrease in COVID-19 case fatality rate in Honduras, from 9.33% before May 3, 2020 to 2.97% after. This suggests the number needed to treat (NNT) is 16 patients to prevent one COVID-19 fatality for the combined inpatient (CATRACHO) and outpatient (MAIZ/MAIZ-AA). Recalculating the control chart limits using the 5.01% average case fatality rate on June 10, 2020 as baseline demonstrated a statistically significant drop below the lower control limit on June 27, 2020. This case fatality rate decrease from 5.01% to 2.97% suggests the avoidance of 1 COVID-19 fatality for every 49 outpatients treated by the additional outreach initiative by Honduran medical brigades implementing the MAIZ/MAIZ-AA outpatient therapeutic protocol.
Conclusion
Our findings demonstrate the utility of statistical process control methodology for quickly and efficiently evaluating and monitoring the efficacy of therapies for COVID-19, which could be generalizable to other emergent conditions.
Acknowledgement
The success and final outcome of this study required the assistance from many people and institutions. We would like to express our gratitude to Mr. Daniel Antonio Fortin, who ingeniously created the “CATRACHO” acronym and helped us reach key decision-makers and local media in order to promote our treatment protocols. As well to Mr. Edgardo Melgar, prestigious journalist, who through the television programs “Hoy Mismo” and “30/30”, provided an information dissemination platform that helped us connect with people nationwide, thereby facilitating the acceptance of these treatments. And we forever thank Dra. Karla Pavon and her team at the Honduran National Surveillance Unit, who did the tenous work of obtain all the detail data and Dr. Angel Díaz and Dr. Danny Ramos for the enormous support in the creation and socialization of the first Honduran National treatment COVID 19 guidelines.
References
-
World Bank. The World Bank in Honduras.
-
(2020) Honduras confirms first 2 cases of new coronavirus. Associated Press.
-
United Nations. World Population Prospects-Population Division. Department of Economic and Social Affairs.
-
Choi A, Bhat S, Velasquez J, Welch W (2022) Coronavirus in New York City. The City.
-
Pascua FV, Diaz O, Medina R, Contreras B, Mistroff J, et al. (2021) A multi-mechanism approach reduces length of stay in the ICU for severe COVID-19 patients. PLoS One 16(1): e0245025.
-
Summary of cases in Honduras. Covid-19 Honduras.
-
(2004) The general who brought the first catrachos. La Prensa.
-
Tardif JC, Bouabdallaoui N, L’Allier P, Gaudet D, Shah B, et al. (2021) Colchicine for community-treated patients with COVID-19 (COLCORONA): a phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. Lancet Resp Med 9(8): 924-932.
-
Sandhu T, Tieng A, Chilimuri S, Franchin G (2020) A Case Control Study to Evaluate the Impact of Colchicine on Patients Admitted to the Hospital with Moderate to Severe COVID-19 Infection. Canadian Journal of Infectious Diseases and Medical Microbiology 2020: 1-9.
-
Bryant A, Lawrie TA, Dowswell T, Fordham EJ, Mitchell S, et al. (2021) Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta- analysis, and Trial Sequential Analysis to Inform Clinical Guidelines. Am J Ther 28(4): e434-e460.
-
Mariette X, Hermine O, Tharaux P, Rigon MR, Steg PG, et al. (2021) Effectiveness of Tocilizumab in Patients Hospitalized With COVID-19: A Follow-up of the Corimuno-Toci-1 Randomized Clinical Trial. JAMA Intern Med 181(9): 1241-1243.
-
Horby P, Lim WS, Emberson JR, Mafham M, Bell JL, et al. (2021) Dexamethasone in Hospitalized Patients with Covid-19. N Engl J Med 384(8): 693-704.
-
Lemos ACB, do Espírito Santo DA, Salvetti MC, Gilo RN, Agra LB, et al. (2020) Therapeutic versus prophylactic anticoagulation for severe COVID-19: A randomized phase II clinical trial (HESACOVID). Thromb Res 196: 359-366.
-
Statistical Process Control: Possible uses to monitor and evaluate patient centered medical home models. PCMH Research Methods Series, pp: 1-10.
-
Thor J, Lundberg J, Ask J, Olsson J, Carli C, et al. (2007) Application of statistical process control in healthcare improvement: systematic review. Qual Saf Health Care 16(5): 387-399.
-
Perla R, Provost S, Parry G, Little K, Provost LP (2021) Understanding variation in reported covid-19 death with a novel Shewhart chart application. Int J Qual Health Care 33(1): mzaa069.
-
World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard.
-
Padgett W, Spurrier J (1990) Shewhart-type charts for percentiles of strength distributions. Journal of Quality Technology 22(4): 283-288.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria