Death from COVID-19 in Thailand 2020-2021
The disease COVID-19 outbreak began in Thailand in May 2020 in Bangkok. And spread too many provinces across the country, resulting in Thailand having 2,361,702 cases and 22,000 deaths (as of January 21, 2022), with the highest number of deaths reported on August 18, 2021, of 312 people. Most of the deaths were aged 70 years or more, accounting for 46.17 percent, followed by the age of 60-69 years, accounting for 22.63% and aged 50-59 years, accounting for 16.94%, respectively, and found that most of the deaths were 84.8% each not vaccinated. From the past studies, it was found that patients infected with the COVID-19 with risk factors are having underlying disease, overweight and smoking behavior are more likely to die than those without those risk factors. And patients vaccinated against COVID-19 are less likely to die than unvaccinated patients. Although vaccines are currently being developed to prevent disease and the production of therapeutic drugs. But still the number of deaths raises continuously, so care, prevention of infection and maintaining health is the best way to deal with the coronavirus disease 2019. Thus, promoting good food intake, exercise and refraining from smoking or unhealthy habits is paramount in the fight against COVID-19.
Introduction
COVID-19, a disease caused by a new strain of Corona Virus, is severe acute (SARS-CoV-2). The coronavirus disease 2019 epidemic began in December 2019 in Wuhan, China
and spread around the world, including Thailand [1]. The epidemic in Thailand started in May 2020 from the situation in the boxing stadium Bangkok and started the second round of outbreaks from Burmese migrant workers who travel to find work in Thailand a lot. This has resulted in outbreaks in provinces where these workers work. And the biggest outbreak was a ripple in April 2021 from an entertainment venue in Thonglor. This wave of outbreaks has spread rapidly across the country. Department of Mental Health [2] resulting in a large number of patients and deaths. Bangkok area which is a large crowds and congestion. In addition, during the said period, there was an announcement of the closure of the city in the Bangkok area. Caused the movement of the population out to different provinces causing the infected people to spread out to the provinces [3]. Compared to the number of deaths, it was found that in 2020 there were only 61 deaths, but in 2021, 21,604 deaths were found, 354 times more than in 2020. In line with the countries continuing rise in the number of cases in the critically ill population [4].
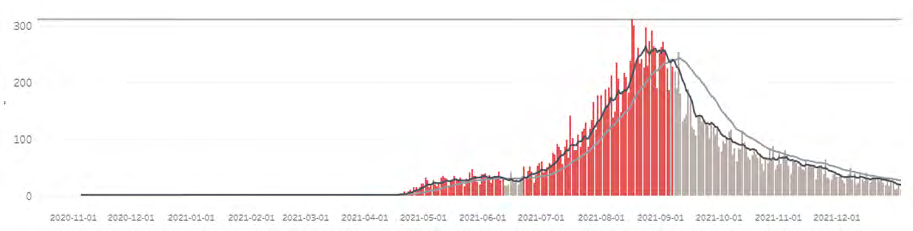
When comparing the number of deaths from the first wave of epidemic (January 01-December 15, 2020) number 60, new wave (December 16, 2020-March 31, 2021) number of 34 cases and April wave (April 1, 2021-August 20, 2021) of 8,492 cases, which accounted for 98.90 percent of the number of deaths, as shown in Figure 1 of all since the start of the outbreak, 76.97% of which were people with underlying diseases such as high blood pressure, heart disease, respiratory disease, chronic diseases and obesity, etc [5].
Vaccines
There are 280 vaccines for the prevention of coronavirus disease 2019, of which 100 are currently being studied in humans and 184 are currently being tested on animals. And these vaccines come in a variety of manufacturing technologies, with most vaccines aiming to boost the body’s immune response to Spike protein. It has been found that those who have recovered from COVID-19 have higher levels of antibodies to Spike protein, especially in for RBD (Anti- RBD Antibody). We use RBD antibody levels as a measure of the level of immunity and response to vaccines. The technology for producing vaccines that have been studied in humans is divided into 4 main processes:
- Genetic vaccines are DNA (DNA) or mRNA (mRNA) vaccines such as Moderna and Pfizer.
- Recombinant viral vector vaccines such as AstraZeneca
- A vaccine made from part of the protein (protein subunit vaccine), such as Novavax.
- Inactivated vaccines such as Sinopharm and Sinovac.
Vaccines can prevent severe symptoms of the disease and death. A Sinovac company study found that the vaccine was 50.70 percent effective in preventing disease among all patients and 83.70% effective in preventing moderate and severe disease. It was effective in preventing hospitalization and severe disease by 100.00%. Sinopharm found its efficacy in a phase 3 study in several Middle Eastern countries and China. The effectiveness of preventing hospitalization was 78.72% and prevention was 78.10% [15]. Moderna found that it could reduce the severity of the disease by 100% and reduce the mortality from infection. 100% of COVID-19 and from the latest laboratory data it was found that the immune stimulation was high enough to suppress the strains B.1.17 from England and B.1.351 from South Africa [16]. Five types of vaccines are available in Thailand are Sinovac, Sinopharm, AstraZeneca, Moderna and Pfizer. Thailand had the first dose of vaccination on February 28, 2021.
Previous studies of mortallity risk factors
Underlying Diseases
Past studies have shown that people with underlying diseases are at risk for death compared to healthy people. Namely, patients with coronary artery disease (OR = 7.34, 95% CI was 0.23-87.02), hypertension (OR = 5.52, 95% CI = 0.26-65.03) and myocardial infarction (OR = 7.32, 95%. CI = 0.28-95.02) risk of death in severe and critically ill COVID-19 patients during hospitalization [19], including diabetes (pooled ORs. = 2.41: 95%CI = 1.05–5.51) Chronic obstructive pulmonary disease (COPD) (pooled ORs = 3.53: 95%CI = 1.79– 6.96) and cancer (pooled ORs = 3.04: 95%CI = 1.80–5.14) have a higher risk of death than COVID-19 patients with no history of underlying disease and a study in Italy [20] found that patients with chronic obstructive pulmonary disease were associated with the loss of patients with COVID-19. Statistically significant, patients with COPD were 1.68 times more likely to die than patients without COPD (p<0.001: HR = 1.68 ; 95% CI = 1.28 -2.19) and patients with heart disease are associated with the loss of patients with COVID-19 at no statistically significant (p=0.38), patients with heart disease were 1.09 times more likely to die than patients without heart disease (HR=1.09; 95%CI=0.91-1.29) [21].
BMI
A study in the United States found that BMI was associated with death in coronavirus patients with statistical significance (p<0.05), that is, patients with COVID-19 and BMI of 30 to 39 kg/m2 were 1.02 times as likely to die as those with a BMI < 23 kg/m2 (OR = 1.02; 95% CI =1.02-1.04) [22], consistent with the study in Iran. BMI is related to death in COVID-19 patients. Statistically significant, that is, patients with COVID-19 and BMI > 35 kg/m2 were 4.22 times more likely to die than those with a BMI ≤ 35 kg/m2 (p<0.001; OR= 4.22 : 95% CI= 2.01- 8.85) and Rast City Studies Iran [23]. BMI was statistically associated with mortality among patients with COVID-19 highest BMI of 33 kg/m2 were 2.49 times more likely to die compared to those with the lowest BMI of 28 kg/m2 (p=0.01; ORadj=2.49:95%. CI=1.15-5.41) [24].
Smoking
A study of risk factors associated with death in COVID-19 patients. A systematic review and meta-analysis study, collected from the COVID-19 resource centers of The Lancet, found that COVID-19 patients with a history of smoking were significantly associated with hospital deaths, that is, COVID-19 patients with a history of smoking were 1.26 times more likely to die than those without a history of smoking (p<0.001; RR=1.26; 95% CI=1.20-1.32) [25]. In Ethiopia COVID-19 patients with a history of smoking is associated with death statistically significant (p=0.02), that is, patients with COVID-19 with a history of smoking were 2.55 times more likely to die compared to those without a history of smoking (ORadj=2.55 ;95%CI=1.15-5.65) [26].
Treatment
Currently, there is a drug to treat coronavirus disease 2019. The first drug called Molnupiravia is manufactured by Merck and Ridgeback BioTeraputics, and the second drug, Paxlovid, is made by Pfizer. However, these two drugs are new drugs. And still need to study further. And be careful before using it in the clinical practice [27]. In Thailand, favipiravir is used as the main drug to treat COVID-19 patients according to the COVID-19 care guidelines by the Department of Medicine Ministry of Health. This is because the drug is very effective in reducing the viral load. And from the historical analysis of COVID-19 patients in Thailand, it was found that favipiravir treatment is an important factor that reduces the risk of severe cases of COVID-19 [28, 29, 30, 31].
Summary
Coronavirus disease 2019 is an emerging infectious disease that has been spreading for 2 years and still can’t control the epidemic in many countries around the world, including Thailand. Although vaccines and drugs to treat coronavirus have been produced, deaths are still being reported. Many studies on risk factors in the past have found that risk factors contributing to the death of coronavirus disease 2019 patients are caused by the patient’s own health behaviors. Thus, promoting good food intake, exercise and refraining from smoking or unhealthy habits is paramount in the fight against COVID-19.
References
-
World Health Organization (2020) Naming the coronavirus disease (COVID-19) and the virus that causes it.
-
Department of Mental Health (2021) Coping with the new wave of COVID-19 outbreak.
-
Department of Disease Control (2021) Disease situation of COVID-19 Measure and problems to support and prent travel and tourism.
-
Covid-19 Situation Administration Center (2019) Coronavirus disease situation 2019.
-
Department of Disease Control (2021) Disease situation of COVID-19 issue 59.
-
World Health Organization (2021) Coronavirus infection 2019.
-
Department of Disease Control (2021) Disease situation of COVID-19 in Thailand.
-
Department of Disease Control (2021) Guidelines for surveillance, prevention and control of COVID-19.
-
Department of Disease Control (2021) Guidelines for clinical practice, diagnosis, treatment and prevention of healthcare-associated infection in response to patients with COVID-19 infection.
-
Heymann DL, Shindo N (2021) COVID-19: what is next for public health?. Lancet 395(10224): 542-545.
-
Ragab D, Eldin HS, Taeima M, Khattab R, Salem R (2020) The COVID-19 Cytokine Storm; What We Know So Far. Front Immunol 11: 1446.
-
Department of Disease Control (2021) Guidance for those handling dead bodies of persons confirmed or suspected to have been infected with COVID-19.
-
General Communicable Disease Division (2021) Guidance for vaccine COVID-19.
-
National Center for Code and Information Standards (2021) Corona Virus Disease 2019 (COVID 19).
-
Department of Disease Control (2021) Symptoms of omicron.
-
(2021) Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Moderna COVID-19 Vaccine- United States, December 21, 2020-January 10, 2021. Morbidity and Mortality Weekly Report 70(4): 125-129.
-
Department of Disease Control (2019) Disease situation of COVID-19.
-
Center for Covid-19 Situation Administration (2021) Disease situation of COVID-19 on 23 August 2021.
-
Hu K, Li B (2020) Logistic regression analysis of death risk factors of patients with severe and critical coronavirus disease 2019 and their predictive value. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 32(5): 544-547.
-
Parohan M, Yaghoub S, Seraj A, Hassan M, Sarraf P, et al. (2020) Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: a systematic review and meta-analysis of observational studies. Aging Male 23(5): 1416-1424.
-
Grasselli G, Greco M, Zanella A, Albano G, Antonelli M, et al. (2020) Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern Med 180(10): 1345- 1355.
-
Breland JY, Wong MS, Steers WN, Yuan AH, Haderlein TP, et al. (2021) BMI and Risk for Severe COVID-19 Among Veterans Health Administration Patients. Obesity 29(5): 825-828.
-
Alamdari NM, Afaghi S, Rahimi FS, Tarki FE, Tavana S, et al. (2020) Mortality Risk Factors among Hospitalized COVID-19 Patients in a Major Referral Center in Iran. The Tohoku Journal of Experimental Medicine 252(1): 73-84.
-
Salari A, Roshan MM, Ghorbani Z, Mortazavi SS, Naghshbandi M, et al. (2021) An investigation of risk factors of in-hospital death due to COVID-19: A case- control study in Rasht, Iran. Irish Journal of Medical Science 190(4): 1321-1333.
-
Reddy KR, Charles NW, Sklavounos A, Dutt A, Seed TP, et al. (2020) The effect of smoking on COVID-19 severity: A systematic review and meta-analysis. Journal of medical virology 93(2): 1045-1056.
-
Mamo AG, Merga BT, Birhanu A, Alemu A, Negash B, et al. (2021) Predictors of Mortality Among Hospitalized COVID-19 Patients at a Tertiary Care Hospital in Ethiopia. Infection and Drug Resistance 14: 5363-5373.
-
World Health Organization (2021) Coronavirus (COVID-19) Dashboard.
-
Health Variety Magazine (2021) Known as “Favipiravir”.
-
World Health Organization (2020) COVID-19.
-
Division of General Communicable Diseases (2021) Coronavirus infection.
-
Center for Covid-19 Situation Administration (2021) Disease situation of COVID-19 on 19 August 2021.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria