Therapeutic Effect of Brace on Adolescent Idiopathic Scoliosis
Objective: To observe the deformity development of adolescent idiopathic scoliosis (AIS) after brace treatment, so as to explore the effects of compliance, initial angle, initial diagnosis age, scoliosis type, bone development and other factors on the change of Cobb angle after wearing orthotic brace. Methods: From January 2018 to December 2021, 39 patients with adolescent idiopathic scoliosis (AIS) with Cobb angle ≥ 20 ° were selected. The data were complete and the follow-up time was ≥ 6 months, including 4 males and 35 females, aged 10-17 years, and the follow-up time was 6-25 months. The full-length frontal and lateral X-ray films of the spine at the initial diagnosis and the last follow-up were selected to measure the Cobb angle, and the effects of the above factors on the Cobb angle were observed; If the difference between the initial Cobb angle and the last Cobb angle is > 0, it is valid; if ≤ 0, it is invalid. Results: There were 39 cases in this group, 31 cases were effective and 8 cases were ineffective. Conclusion: Brace treatment is effective for most adolescent idiopathic scoliosis, but ineffective in a few cases; Due to the small sample size of this observation, the analysis of the observation data shows that the specific curative effect has no correlation with the initial angle, age of initial diagnosis, bone development, etc.
Introduction
Adolescent idiopathic scoliosis (AIS) is a teenager aged 10-18 years. No specific etiology of scoliosis has been found. Spinal deformity with coronal Cobb angle exceeding 10° [1]. For AIS, the general treatment principle is that the Cobb angle is 10°-20°, guide patients to carry out appropriate spinal flexibility training, take films every 6 months and follow up for a long time; Cobb angle 20° - 40°, brace treatment, film re-examination every 3-6 months and long-term follow-up; Cobb angle > 40°, surgical treatment is recommended. From January 2018 to December 2021, 39 patients with adolescent idiopathic scoliosis (AIS) with Cobb angle ≥ 20° and brace treatment were selected for observation. The report is as follows.
Clinical Data
General Data: take AIS patients who were treated in the special disease clinic of children’s spinal deformity of Gansu Hospital of traditional Chinese medicine from January 2018 to December 2021 as the research object. Inclusion criteria:
- Aged 10-17 years
- Cobb angle ≥ 20°
- No abnormal vertebral development or other system abnormalities were found
- The data were complete and the follow-up time was ≥ 6 months. Exclusion criteria
- Various types of vertebral dysplasia
- Scoliosis caused by various congenital diseases
- Age < 10 years old or > 18 years old
- Cobb angle ≥ 50°
- Those who fail to take films on time for follow-up or follow-up for less than 6 months.
There were 39 patients in this group, including 4 males and 35 females, aged 10-17 years, followed up for 6-25 months. Table 1 for details.
| Serial Number | Gender | Age of Initial Diagnosis (Years) | Cobb Angle at Initial Diagno- sis (°) | Last Cobb Angle (°) | Follow Up Duration (Months) | Angle Differ- ence (°) | Correction Rate (%) |
|---|---|---|---|---|---|---|---|
| 1 | F | 17 | 43 | 40 | 17 | 3 | 6.98 |
| 2 | F | 14 | 35 | 30 | 10 | 5 | 14.29 |
| 3 | F | 11 | 49 | 34 | 24 | 5 | 10.2 |
| 4 | F | 14 | 30 | 28 | 10 | 2 | 6.67 |
| 5 | F | 11 | 38 | 47 | 25 | -11 | 0 |
| 6 | F | 10 | 27 | 23 | 9 | 4 | 14.81 |
| 7 | F | 15 | 32 | 23 | 4 | 9 | 28.13 |
| 8 | M | 17 | 30 | 21 | 12 | 9 | 30 |
| 9 | F | 14 | 28 | 27 | 11 | 1 | 7.14 |
| 10 | F | 10 | 22 | 13 | 8 | 9 | 40.91 |
| 11 | F | 13 | 22 | 13 | 9 | 9 | 40.91 |
| 12 | F | 15 | 29 | 33 | 8 | -4 | 0 |
| 13 | F | 15 | 23 | 21 | 6 | 2 | 8.7 |
| 14 | M | 16 | 33 | 33 | 6 | 0 | 0 |
| 15 | F | 16 | 30 | 30 | 7 | 0 | 0 |
| 16 | M | 13 | 20 | 7 | 6 | 13 | 65 |
| 17 | F | 12 | 28 | 13 | 6 | 15 | 53.57 |
| 18 | F | 13 | 30 | 21 | 6 | 9 | 30 |
| 19 | M | 13 | 29 | 29 | 11 | 0 | 0 |
| 20 | F | 13 | 35 | 34 | 18 | 1 | 2.86 |
| 21 | F | 10 | 39 | 45 | 12 | -6 | 0 |
| 22 | F | 17 | 30 | 20 | 23 | 10 | 33.33 |
| 23 | F | 14 | 25 | 20 | 6 | 5 | 20 |
| 24 | F | 15 | 15 | 23 | 15 | -8 | 0 |
| 25 | F | 16 | 20 | 27 | 13 | -7 | 0 |
| 26 | F | 10 | 27 | 26 | 25 | 1 | 10 |
| 27 | F | 15 | 20 | 20 | 18 | 0 | 0 |
| 28 | F | 15 | 35 | 35 | 12 | 0 | 0 |
| 29 | F | 12 | 37 | 30 | 6 | 7 | 18.92 |
| 30 | F | 16 | 27 | 24 | 6 | 3 | 11.11 |
| 31 | F | 12 | 25 | 28 | 6 | -3 | 0 |
| 32 | F | 13 | 32 | 25 | 6 | 7 | 21.88 |
| 33 | F | 12 | 26 | 26 | 6 | 0 | 0 |
| 34 | F | 12 | 48 | 59 | 6 | -11 | 0 |
| 35 | F | 10 | 39 | 45 | 12 | -6 | 0 |
| 36 | F | 15 | 28 | 25 | 6 | 3 | 10.71 |
| 37 | F | 11 | 29 | 28 | 8 | 1 | 3.45 |
| 38 | F | 11 | 22 | 17 | 19 | 5 | 22.73 |
| 39 | F | 14 | 30 | 23 | 7 | 7 | 23.33 |
Table 1: Specific conditions of 39 patients in this group.
Note: 1 Angle difference = initial Cobb angle - last Cobb angle Correction rate = angle difference/Cobb angle of initial diagnosis × 100% If the angle difference is negative, the correction rate is 0, which is invalid. Table 1: Specific conditions of 39 patients in this group.
Research Method
Wearing Methods: Wearing method of braces all braces are customized by professional orthopaedic brace manufacturers. For the first time, it is required to wear 20 hours a day, emphasizing night wear; When not wearing, encourage patients to carry out spinal flexibility training, such as gymnastics, broadcast gymnastics, dance, swimming, etc; 3-6 months (generally the fourth month after the third month), and take full-length films of the spine; Adjust the brace and wearing time according to the change of Cobb angle.
Observation Methods: The full-length anteroposterior and lateral X-ray films of the spine at the initial diagnosis and the last follow-up were selected to measure the Cobb angle. The improvement rate of Cobb angle at the last follow-up compared with the initial Cobb angle is > 0, which is effective, and ≤ 0 is ineffective.
was used to calculate the difference, P < 0.05.
Results
For 39 patients in this group, see Table 2 for different correction rates.
| Correction rate (%) | Number of cases | Proportion (%) |
|---|---|---|
| ≥50.00 | 2 | 5.13 |
| 40.00-49.99 | 2 | 5.13 |
| 30.00-39.99 | 3 | 7.69 |
| 20.00-29.99 | 5 | 12.82 |
| 10.00-19.99 | 7 | 17.95 |
| 0-9.99 | 5 | 12.82 |
| <0 | 8 | 20.51 |
Table 2: Comparison of imaging findings between the brace before treatment and the last follow-up (x) ̅±s).
- Note: if the correction rate is > 0, the Cobb angle decreases;
- Correction rate ≤ 0, Cobb angle does not change or increase.
- Statistical Processing
- Adopt spss24 0. The imaging parameters before and after treatment and before treatment were compared with those at the last follow-up by paired t-test (P < 0.05). The
- Fisher test was used to compare the data, or the Fisher test
- After the initial treatment and the last follow-up, the Cobb angle was significantly better than that before treatment (P
- < 0.05) Table 3.
- Initial diagnosis Cobb angle/° final Cobb angle /°
- Initial Cobb angle and final Cobb angle (before and after treatment) t p
- 29.92±7.43
- 27.33±10.17
- 2.531
- 0.016
Table 3: Comparison of imaging findings between the brace before treatment and the last follow-up (x) ̅±s).
In this group of patients, the relationship between initial Cobb angle, age of initial diagnosis, scoliosis type, bone maturity and correction rate is shown in Table 4.
| Serial number | Initial Cobb angle (°) | Age of initial diagnosis (years) | Scoliosis type | Risser’s rating | Is the Y-shaped cartilage closed | Correction rate (%) |
|---|---|---|---|---|---|---|
| 1 | 43 | 17 | L | 4 | Y | 6.98 |
| 2 | 35 | 14 | L | 3 | Y | 14.29 |
| 3 | 49 | 11 | T | 3 | Y | 10.2 |
| 4 | 30 | 14 | D | 3 | Y | 6.67 |
| 5 | 38 | 11 | T | 1 | N | -28.95 |
| 6 | 27 | 10 | T | 0 | N | 14.81 |
| 7 | 32 | 15 | T | 3 | Y | 28.13 |
| 8 | 30 | 17 | TL | 5 | Y | 30 |
| 9 | 28 | 14 | T | 3 | Y | 7.14 |
| 10 | 22 | 10 | T | 0 | N | 40.91 |
| 11 | 22 | 13 | T | 2 | Y | 40.91 |
| 12 | 29 | 15 | D | 4 | Y | -13.79 |
| 13 | 23 | 15 | T | 3 | Y | 8.7 |
| 14 | 33 | 16 | T | 4 | Y | 0 |
| 15 | 30 | 16 | T | 3 | Y | 0 |
| 16 | 20 | 13 | T | 1 | Y | 65 |
| 17 | 28 | 12 | T | 2 | Y | 53.57 |
| 18 | 30 | 13 | L | 2 | Y | 30 |
| 19 | 29 | 13 | TL | 0 | N | 0 |
| 20 | 35 | 13 | L | 0 | N | 2.86 |
| 21 | 39 | 10 | T | 0 | Y | -15.38 |
| 22 | 30 | 17 | L | 4 | Y | 30.33 |
| 23 | 25 | 14 | T | 0 | N | 20 |
| 24 | 15 | 15 | T | 3 | Y | -53.33 |
| 25 | 20 | 16 | T | 2 | Y | -35 |
| 26 | 27 | 10 | T | 0 | N | 10 |
| 27 | 20 | 15 | L | 3 | Y | 0 |
| 28 | 35 | 15 | T | 3 | Y | 0 |
| 29 | 37 | 12 | D | 2 | Y | 18.92 |
| 30 | 27 | 16 | TL | 3 | Y | 11.11 |
| 31 | 25 | 12 | D | 1 | Y | -12 |
| 32 | 32 | 13 | L | 2 | Y | 21.88 |
| 33 | 26 | 12 | D | 2 | Y | 0 |
| 34 | 48 | 12 | T | 0 | Y | -22.92 |
| 35 | 39 | 10 | T | 0 | Y | -15.38 |
| 36 | 28 | 15 | TL | 3 | Y | 10.71 |
| 37 | 29 | 11 | T | 0 | Y | 3.45 |
| 38 | 22 | 11 | L | 0 | Y | 22.73 |
| 39 | 30 | 14 | T | 3 | Y | 23.33 |
Table 4: Relationship between initial Cobb angle, age of initial diagnosis, scoliosis type, bone maturity and correction rate.
Note: Lumbar curvature=L; Thoracic curvature=T; Thoracolumbar curvature=TL; Double bend=D; Yes=Y; No=N Table 4: Relationship between initial Cobb angle, age of initial diagnosis, scoliosis type, bone maturity and correction rate.
There was no significant difference in the effects of initial Cobb angle, initial diagnosis age, scoliosis type and bone maturity on the correction rate (P > 0.05), as shown in Table 5.
| Initial diagnosis Cobb angle/ ° | Age at first visit / year | Correction rate /% | |
|---|---|---|---|
| x±s | 29.92±7.43 | 13.38±2.16 | 13.66±16.29 |
| statistic p | 0.163 | 0.132 | 0.201 |
| 0.228 | 0.468 | 0.074 |
Table 5: Relationship between initial Cobb angle, initial diagnosis age, scoliosis type, bone maturity and correction rate.
Typical Cases
Case 1
Female, 12 years old, was treated with brace for 6 months. Before treatment (Figure 1), after treatment (Figure 2), Cobb angle decreased by 15° after treatment.
Case 2
Male, 13 years old, was treated with brace for 11 months. There was no change in Cobb angle before and after treatment (Figure 3) and (Figure 4).
Case 3
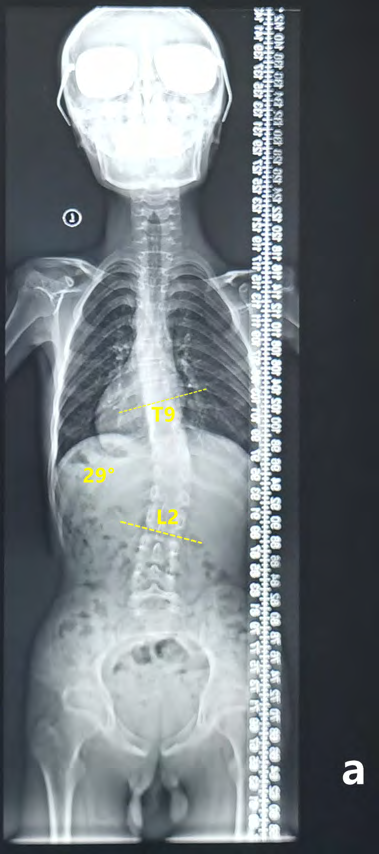
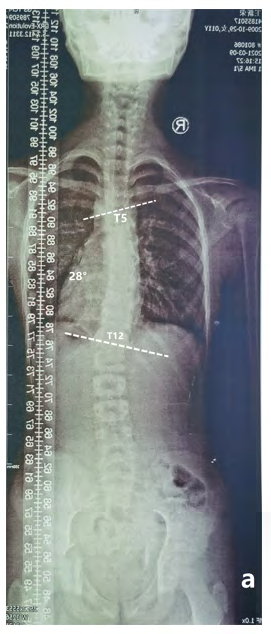
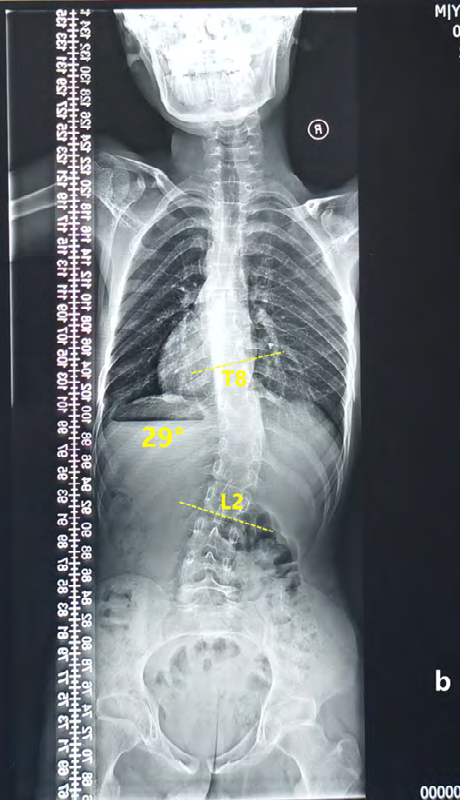
Female, 11 years old, was treated with brace for 25 months. Before treatment (Figure 5), after treatment for 7 months (Figure 6), after treatment for 25 months (Figure 7), the Cobb angle decreased after treatment for 7 months, but the patient’s compliance was poor and did not return to the clinic on time. After 25 months, the Cobb angle increased and there were surgical indications.

Discussion
The exact cause of adolescent idiopathic scoliosis (AIS) is still unclear, but its complex pathogenesis has been described by Institutions [2]. The intervention measures to prevent the progression of AIS mainly include exercise therapy, brace treatment and surgical treatment. The efficacy of brace treatment has been controversial for a long time. Until 2013, a multicenter randomized controlled trial confirmed the effect of brace treatment. This study shows that brace treatment can effectively prevent the progression of Cobb angle to the surgical threshold in patients with AIS, i.e. more than 50° [2, 3]. The author believes that the role of the brace is first to “delay the progress of scoliosis” and then “improve the angle of scoliosis”. Therefore, this group recognizes the patients who wear the brace for 6 months with Cobb angle correction rate = 0 as effective because the scoliosis is not aggravated under the action of the brace. The theoretical basis of brace treatment and correction of scoliosis includes frontal “three-point force system”, local “force pair system” and sagittal spinal balance. The international Scoliosis Research Association (SRS) points out that brace treatment is suitable for AIS patients with immature bones and Cobb angle between 20°~45° [4].
The systematic research of Hawary RE, et al. [5] and Xu L, et al. [6] shows that the main factors leading to the failure of brace treatment are:
- Large initial Cobb angle.
- Lower Risser score; Lower bone maturity.
- The type of scoliosis can be used as a determinant to predict the success of brace treatment.
However, after the initial treatment and the last follow- up, the Cobb angle was significantly better than that before treatment (P < 0.05)., There was no significant correlation between the initial Cobb angle, the age of initial diagnosis, the type of scoliosis and bone maturity. Because the number of cases in this group is small, only reference is provided. After follow-up, it was found that there was a great relationship between brace compliance and treatment effect. Patients who strictly followed the doctor’s advice, wore braces for 20 hours a day and insisted on flexibility training achieved a good correction rate.
Conclusion
In conclusion, brace treatment can delay the progress of scoliosis and improve the angle of scoliosis in adolescents. It is an effective conservative treatment. The effect of brace treatment has nothing to do with the patient’s initial age, Cobb angle, scoliosis type and bone development, which is inconsistent with the research results of some scholars. The correlation between the effect of brace treatment remains to be further observed. This study initially provided relevant data to observe the therapeutic effect of brace in 39 patients with AIS. However, this group has a small sample size and a short observation time, so it can only make a preliminary observation of the treatment process of one group of patients.
References
-
Weinstein SL, Dolan LA, Cheng JC, Danielsson A, Morcuende JA (2008) Adolescent idiopathic scoliosis. Lancet 371(9623): 1527-1537.
-
Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, et al. (2018) 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and Spinal Disorders 13: 3.
-
Weinstein SL, Dolan LA, Wright JG, Dobbs MB (2013) Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 369(16): 1512-1521.
-
Stephens RB, Robert MB, Charles RD, George HT (2005) Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS committee on bracing and nonoperative management. Spine 30(18): 2068-2075.
-
Hawary RE, Regev DZ,Floman Y, Lonner BS, Alkhalife YI, et al. (2019) Brace treatment in adolescent idiopathic scoliosis:risk factors for failure-a literature review. Spine J 19(12): 1917-1925.
-
Xu L, Qin X, Qiu Y, Zhu Z (2017) Initial correction rate can be predictive of the outcome of brace treatment in patients with adolescent idiopathic scoliosis. Clin Spine Surg 30(4): E475-E479.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria