Multidimensional Evaluation and Profile of Institutionalized Elderly in Pindamonhangaba-SP, Brazil
Introduction: With the increase in the elderly population, it is necessary to use tools that identify health problems efficiently, in primary care and in Long-stay institution for the elderly (LSIE). Objective: The present study aimed to identify and characterize functional alterations through multidimensional assessment of the elderly (MAE) and to estimate the prevalence of elderly people with a suggestion of Dynapenia. Methods: This is a descriptive cross-sectional observational study. Thirty-one elderly people of both sexes, living in two LSIEs in the municipality of Pindamonhangaba, were included. The instrument for the multidimensional assessment of the elderly proposed for this study was developed to be used in a primary health care outpatient clinic. Information on sociodemographic characteristics, history of personal morbidity, musculoskeletal symptoms, quality of balance, functionality, lifestyle, medication use, anthropometric measurements and quality of life were searched. Data were statistically analyzed using the chi-square method and the Bioestat 5.0 software as a support tool. Results: When evaluating the domains in the AMI, we identified: absence of upper limb dysfunction and a significantly high rate (p
Introduction
According to the World Health Organization (WHO) [1], an elderly person is anyone aged 60 years or over. The Brazilian Institute of Geography and Statistics (IBGE) states that today 13% of the entire population of the country is elderly and that this number tends to double in the coming decades. The Pan American Health Organization (PAHO) defines aging as “a sequential, individual, cumulative, irreversible, universal, non-pathological process of deterioration of a mature organism, characteristic of all members of a species, in a way that time makes it less able to cope with the stress of the environment and therefore increase their possibility of death [1].
In this aging process, from the third decade of life onwards, there is a gradual reduction in the ability to maintain homeostasis in each organ and system, but this decline is influenced by diet, environmental conditions, life habits and genetic factors, making old age a unique experience for each individual [2]. From the fourth decade of life onwards, one can generally observe that the hair becomes whitish, the skin becomes drier and less elastic, and sensory perception is reduced during aging, which is well observed in relation to auditory sensitivity. The touch, in addition to the perception of taste, is also affected and decreases with aging. However, with regard to pain sensitivity, it seems to be preserved and can often be increased due to pathologies that affect the joints, which are common in the elderly [3].
In old age, there are changes in the nervous system resulting from the loss of brain mass, with consequent impairment of balance. There is also an increase in adipose tissue, especially in characteristic regions such as the abdominal region. There are changes in the myocardium and respiratory system, postural changes, changes in the ventilation-perfusion ratio; the digestive system slows down, changes occur in hormone levels, with a decrease in estrogen production in women and a gradual reduction in testosterone in men; the urinary and glandular systems also undergo a degenerative process over the years [4]. Modifications also become evident with aging in the musculoskeletal system with the respective decrease in length, elasticity and number of muscle fibers [5]. The musculoskeletal system is progressively transformed and starts to acquire specific structural and morphological characteristics that impair the functional and physical capacity of the individual. Also notable is the loss of muscle mass and elasticity of tendons and ligaments [6].
In the elderly, there is an important decrease in the proportion of anaerobic, fast-twitch muscle fibers, compared to aerobic, slow-twitch fibers. Evidence shows that age- related changes in muscle mass can explain less than 5% of the variation in muscle strength, that is, the relationship between these two conditions is not linear. Therefore, the decline in muscle strength seems to occur much faster than the decrease in muscle mass [7]. Dynapenia is the name given by Clark BC, et al. [8] in 2008, to the loss of muscle strength related to advancing age and that is not caused by neurological or muscular diseases. Dynapenia predisposes older adults to an increased risk of functional limitations and mortality. On the other hand, subclinical deficits in the structure and function of the nervous system and/or deficiencies in the intrinsic force-generating properties of skeletal muscle are potential antecedents for this condition [8].
Considering the increase in life expectancy and the number of elderly people in Brazil, and that physiological changes are inherent to the aging process, creating strategies to track important systemic changes that result in loss of function and independence are essential to contain the advance of morbidities and mortality. For a comprehensive assessment, taking into account different dimensions of aging, Sirena SA [9] proposed a quick and easy-to-apply instrument for the Multidimensional Assessment of the Elderly. The information provided in this instrument associated with simple methods of classic assessment, such as weight, height and hand grip strength, can lead to the diagnosis of Dynapenia, an important pathology in the impairment of functionality.
In this sense, the objective of the present study was to characterize the functional alterations identified through the multidimensional assessment of the elderly and to estimate the prevalence of elderly people with characteristics suggestive of Dynapenia.
Methodology
This is a descriptive cross-sectional observational study, whose variables investigated were: multidimensional assessment of the elderly, sociodemographic characteristics (age, sex, race, marital status, education, occupation and income), history of morbidity (systemic arterial hypertension, diabetes mellitus, heart diseases, depression, musculoskeletal symptoms and obesity), life habits (smoking, alcohol consumption and physical exercise), cognition, static and dynamic balance, medication use, quality of life and anthropometric measurements (weight, height, abdominal circumference and palm grip strength). Thirty-one elderly people over 60 years of age, of both sexes, residents of two Long-Term Care Institutions for the Elderly in the city of Pindamonhangaba-SP were invited, composing a convenience sample, where all agreed to participate, with no withdrawal. Elderly people who had difficulty speaking, hearing or understanding were excluded due to the impossibility of responding to the interview.
To collect the handgrip strength, a digital manual dynamometer, brand CAMRY, model EH 101, was used. Three measurements were obtained with an interval of one minute between them, and the result was presented in kilograms/ force (kg/f). The mean value between the measurements was considered and the cutoff points proposed by Mancini RB, et al. [10], which are values below 26 kg for men and 16 kg for women, were adopted. For the multidimensional assessment of the elderly, the instrument proposed by Sirena SA [9] was used to screen the main problems related to aging in primary care. These are simple tests and quick application identifying the following changes: 1. Vision-The Jaeger card was placed at a distance of 35 cm from the elderly person. The vision of the two eyes was tested separately and then together, with corrective lenses if the elderly person used them. Patients who were able to read up to the 20/40 level were considered without dysfunction.
2. Hearing-from the Whisper test or the whisper test, where the examiner, outside the patient’s visual field, at a distance of approximately 33 cm, whispers a brief and simple question, e.g. ex. “What’s your name?” in each ear. If the patient does not respond, they should be referred for a more detailed and specialized investigation.
3. Function of the upper limbs-the patient is asked to place both hands on the back of the neck, observing the presence of pain and limitation during the execution of the test. If the patient is able to touch the back of the head with both hands, he probably has adequate proximal upper limb function. The patient was also asked to pick up a pencil on the table, with both hands. The ability to wield and perform the function of digital tweezers is essential in maintaining the ability to dress, bathe and eat. The ability to pick up this object suggests that the patient has the ability to write and manipulate utensils, being free from distal upper limb dysfunction.
4. Lower limb function-This function can be tested using the Time Up and Go Test (TUGT). The patient is asked to get up from the chair, walk approximately 3 meters, turn around and return to their chair and sit down again. Excessive slowness, hesitation, excessive trunk sway, need for support, or stumbling indicate gait and/or balance dysfunction.
5. Mental Status-the Mini Mental Status Examination was used to assess cognitive function and the Geriatric Depression Scale (GDS) to assess mood disorders in patients.
6. Risk of Home Falls-To identify potential risks, the patient should be asked about difficulty with stairs, presence of loose rugs and adequacy of internal and external light in the house. It is also important to inquire about the presence of safety equipment, such as a handrail in the bathroom.
7. Activities of Daily Living-the elderly were asked about performing activities of daily living such as bathing, eating, dressing, going to the bathroom, moving around and walking. It was investigated whether these activities are performed independently, semi-independently (needs help) or dependent (needs someone else to do it). Difficulties with self-care require a more detailed assessment.
8. Urinary incontinence-the simple direct question “Have you ever lost urine or felt wet?” was used.
9. Nutritional Status-the elderly person was asked about unintentional weight loss in the last month. The most useful indicator of nutritional status in the elderly is weight variation from baseline or the presence of anorexia. A weight loss of more than 5% (+/- 2.3 kg) in 1 month or more than 10% (+/- 4.5 kg) in 6 months is significant.
10. Social Support-information about retirement and family or friends to contact in case urgent support was needed from the patient’s medical record.
For the investigation of the other variables, a Roadmap for Data Collection was created by the researchers, containing questions about sociodemographic characteristics, life habits, history of morbidity, medication use and anthropometric measurements. Data collection took place at the two selected LTCFs over a period of 30 days at the year 2019 and included six trained and calibrated researchers, aged between 20 and 40 years. All researchers made previous visits to minimize possible negative reactions of the elderly to the research. The researchers, grouped in pairs, went to the room of the selected elderly and made the invitation to research, in case of acceptance, the evaluation was initiated by the interview, which lasted an average of 30 minutes. Then, physical tests and anthropometry were performed (average of 20 minutes), and finally, medical records were consulted to gather additional information. All data collected were identified by codes, maintaining their confidentiality, and stored in a file only for study purposes and information for proposed measures for prevention programs and possible multidisciplinary interventions of the institutions. Data were statistically evaluated by the chi-square method, at a significance level of 0.05, using the bioestat 5.0 software as a support tool.
Ethical Aspects
The present research was previously submitted to the Research Ethics Committee of the UniFUNVIC University
Center, and approved under protocol number 3,596,759. The two LSIEs involved signed an Authorization Term to carry out the study, and all participants signed, by means of spelling or fingerprint of the right thumb, the Free and Informed Consent Term, after clarifying the procedures, study objectives, risks and benefits.
Results
Thirty-one elderly residents of LSIEs in Pindamonhangaba were evaluated. Of these, 14 (45.2%) were women and 17 were male (54.8%), aged between 63 and 98 years and mean age of 78 years (SD± 8.9 years). Most were white (71.0%), widowed (51.6%), retired (80.6%) and studied up to elementary school I or II (45.3%), as shown in Table 1.
| Features | n | % | |
|---|---|---|---|
| Age | 60 – 70 | 6 | 19.4 |
| Age | 71 – 80 | 13 | 42 |
| Age | 81 – 90 | 10 | 32.3 |
| Age | 91 – 100 | 2 | 6.5 |
| Ethnicity | White | 22 | 71 |
| Ethnicity | Black | 5 | 16 |
| Ethnicity | Brown | 4 | 13 |
| Marital Status | Single | 12 | 39 |
| Marital Status | Married | 2 | 7 |
| Marital Status | Divorced | 3 | 9.7 |
| Marital Status | widowed | 16 | 51.6 |
| Retirement | Yes | 25 | 80.6 |
| Retirement | No | 6 | 19.4 |
| Education | Functional illiterate | 4 | 13 |
| Education | Elementary school I | 9 | 29.1 |
| Education | Elementary school II | 5 | 16.2 |
| Education | High school | 9 | 29.1 |
| Education | Higher school | 4 | 13 |
Table 2: Sociodemographic characteristics of 31 elderly people living in Long Stay Institutions for the Elderly in Pindamonhangab
Considering the associated morbidities, Table 2 presents the most prevalent ones in ascending order, with emphasis on musculoskeletal symptoms and characteristics suggestive of cognitive alterations, which were present in more than half of the elderly who participated in the study, 67.7% and 83.9% respectively, such indicators being significantly (Chi-square) higher than those observed for dyslipidemia, osteoporosis, diabetes mellitus, Metabolic syndrome and Depression, as showed in table 2.
| Morbidities | n | % |
|---|---|---|
| Dyslipidemia | 2 | 6.5 |
| Osteoporosis | 2 | 6.5 |
| diabetes Mellitus | 5 | 16.1 |
| Metabolic Syndrome | 9 | 29 |
| Depression | 10 | 32.3 |
| Systemic Arterial Hypertension - SAH | 12 | 38.7 |
| Musculoskeletal Symptomsc,d | 21 | 67.7 |
| Features Suggestive of Cognitive Changes - FSCC a,b | 26 | 83.9 |
Table 1: Associated morbidities of 31 elderly residents in Long Stay Institutions for the Elderly in Pindamonhangaba- SP, 2019
a=significant difference (Chi-square - p<0.0001) compared to depression, metabolic syndrome, diabetes mellitus, osteoporosis and dyslipidemia; b =significant difference (Chi- square - p<0.01) compared to SAH; c = significant difference (Chi-square - p<0.05) compared to SAH and depression; d = significant difference (Chi-square - p<0.0001) compared to diabetes mellitus, osteoporosis and dyslipidemia. Table 2: Associated morbidities of 31 elderly residents in Long Stay Institutions for the Elderly in Pindamonhangaba- SP, 2019 (n=31).
Through anthropometric assessment, it was possible to identify the high prevalence of overweight and obesity among the elderly. The criterion recommended by the World Health Organization (WHO, 2001) was used to research the Body Mass Index (BMI), characterized by the ratio of weight (kg) divided by height squared (m2). Among the participants, 54.8% (17) were considered overweight and 16.1% (5) obese, been important to highlight that all obese patients corresponded to women. For Palmar Grip Strength (PGS) we obtained an average of 15.7 kg and a standard deviation of 7.9 kg. According to the cut-off score, there was a prevalence of 100% (14) of women with a suggestion of dynapenia, and 82,35% (14) among men, thus, there was no significant difference in the occurrence of dynapenia by gender.
Already relating dynapenia with overweight, 9 (64.28%) of the 14 men with dynapenia were overweight. Among women, 5 (35.7%) of the 14 who had dynapenia were overweight; in relation to dynapenia and obesity, 100% (5) of women were obtained. The mean waist circumference was 100.01 centimeters, with a standard deviation of 10.78 centimeters, also indicating abdominal obesity among the participants. In terms of quality of life, an average score was performed on the SF-36 questionnaire according to each of the following domains: Functional capacity (48.5 points), Limitation due to physical aspects (42.6 points), Pain (64.4 points), General health status (68.7 points), Vitality (70.2 points), Social aspects (75.5 points), Limitation by emotional aspects (70.4 points) and Mental health (76.9 spots). The questionnaire score ranges from 0 to 100, where the closer to 100, the better the quality of life. The elderly in this study showed better quality of life when related to Mental Health, and worse quality of life related to Limitation by physical aspects.
When performing the BERG, POMA and TUGT tests, it was identified that 55.0% (17), 67.0% (21) and 71.0% (27) presented changes in balance and risk of falls, respectively. Considering only the elderly in the study who presented changes in balance, 74.2% were positive in the three tests, indicating an important risk. When evaluating the 10 domains recommended in the Multidimensional Assessment of the Elderly, it was possible to identify four of them that deserve to be highlighted due to their high prevalence: vision changes in 51.6% of the elderly, cognition and memory changes in 45.2%, history of falls in 41.9% and LL dysfunction in 90.3%, hearing problems in 29%. In the social support domain, 80.6% were retired, however it was not possible to obtain information about support related to family or friends. Figure 1 shows the frequency distribution of each of the domains evaluated.
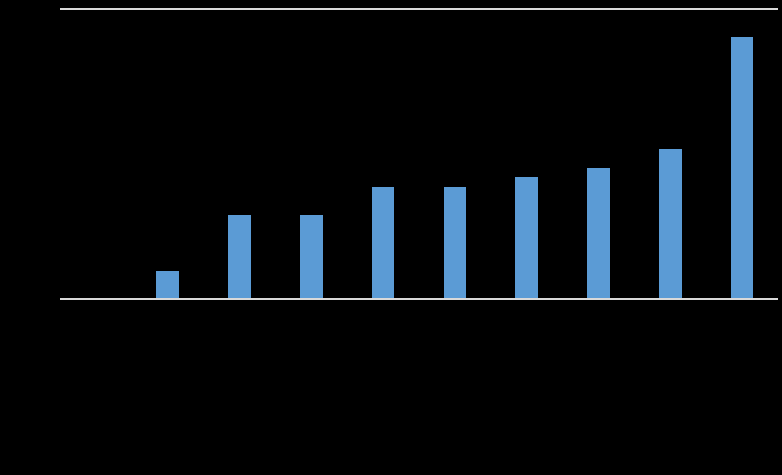
*significant difference (p<0.01) in relation to the other factors Figure 1: Multidimensional Assessment of the Elderly.
Discussion
Regarding the assessment of the occurrence of dynapenia in relation to ethnicity, the small number of black elderly people who participated in the research, which corresponded to only 5 participants (16% of the total), did not allow us to infer possible correlations with this variable. However, it is already widely known that blacks, despite having a superior muscle quality compared to other ethnic groups, have greater muscle loss from the age of 60, reaching up to 28% greater than that observed in white people [11]. As for the occurrence of dynapenia by gender, although there was no significant difference in the occurrence of such a disorder between men and women, it is known that men are prone to suffer this process, since, in senescence, this loss from the age of 60 is twice as long as that observed in females [11].
In relation to the ten domains of the Multidimensional Assessment of the Elderly, four of them deserve to be highlighted due to the results, lower limb dysfunction (90.3%), vision (51.6%), cognition and memory (45.2%) and falls (41.9%). Some information regarding the physical examination is also highlighted, such as the overweight that 54.8% of the elderly presented and the dynapenia presented in 100% of the women. In the “vision” domain, more than half of the elderly had difficulty performing some activity due to visual problems. This result is different from that presented in a study with institutionalized elderly people carried out in Tucuruí, Pará -BR [12] given that, in such research only 46 % of elderly had these problems. The results here exposed were also discrepant to those observed in a study as well as the results evidenced in a study with institutionalized elderly in Rio Grande do Sul-BR, where the medical records of residents were analyzed been observed that 43% of them had this problem [13]. In fact it is already widespread knowledge that visual impairment is a factor that exerts great influence on limitations to perform routine activities, a factor that can influence the quality of life in old age [14, 15].
Regarding the “hearing” domain, the result of the present study agreed with the results obtained by Reis DLA, et al. [12], according to which 23% of the elderly presented, in the whisper test, hearing impairment in both ears, a value close to the one presented here, which corresponded to 22.6%. The importance of detecting and correcting hearing problems early is related to the fact that, as a result of this loss resulting from the effects of aging, the elderly have to face the difficulty of communicating with others, compromising their relationship with family members and friends [16]. The isolation of the elderly and the consequent decline in the quality of their communication, due to sensory deficits, generate a profound impact, since the constant flow of communication and information is what keeps the individual active in society [17].
Regarding the occurrence of weight loss, a study that evaluated frailty in elderly residents in Anápolis-GO found that 33% of them had unintentional weight loss [18] corroborating with the findings of the present study, in which the weight loss were present in 38.7% of the research participants.. It’s possible to infer that the weight loss in elderly is probably related to the natural loss of appetite in most elderly people that tends to develop as they get older. Body weight, which makes up the Body Mass Index (BMI), is the main measure used in anthropometric assessment. Changes in weight reflect an imbalance between food intake and consumption. Involuntary weight loss is closely related to the frailty syndrome in the elderly and is characterized by a decrease in physiological reserves and deficits capable of causing adverse health effects, such as falls, aggravation of diseases, functional disability, comorbidities, hospitalization, prolonged institutionalization and death [19].
In the “falls” domain, in relation to the study in Tucuruí- PA [12] the results presented here differ little from those evidenced in that study, since in Tucuruí there was a prevalence of 46.2% of elderly people who suffered a fall at least once and in this study this proportion was 41.9%. Falls in the elderly are an important cause of morbidity. Because it is an event that causes several injuries, in cases of the elderly, it can be considered a fateful factor. The event of a fall, in addition to being responsible for prolonged treatment times and large health expenditures, can accelerate the process of dependence [20]. Urinary incontinence is very common in the elderly and more frequent in women, but rarely reported, and therefore, the identification and intervention for treatment has a great impact on quality of life. In the study carried out in Tucuruí, Pará [12] the incidence of this disorder was 17%, being slightly lower than the results presented here, which was equivalent to 29% of the research participants, possibly due to differences in the composition of the sample group, which in this case of the present study consisted of men and women while in the Tucuruí study the study was carried out only with men. In Long Stay Institutions in Pindamonhangaba, the prevalence of men with this problem was 9.6%.
As for the ability to perform activities of daily living, such as getting dressed, showering and getting out of bed alone, in this study most of the elderly do this independently, which was also evident in the study in Pará [12] where 70 % of the elderly were totally independent. In a study carried out in Natal with 144 institutionalized elderly people, 53% of the residents had some type of disability in this type of activity [21]. As for social support, in Tucuruí [12] they did not quantify how many elderly people have social support, they mention that most of them have at least one child, however there is an unjustified social distance from the family. In the elderly evaluated in the present study, more than half of them have help, in case of need, from a family member.
There was a difficulty in finding other studies that addressed this issue in institutionalized elderly, since when found, they address more whether or not there is family visit to the elderly, and this was not the focus of the present study, but to know if in case of need this elderly person has someone to count on. Regarding the cognition and memory domain, in the study carried out in Natal [21] it was found that 79.9% of the elderly had cognitive disability. Likewise, in a study carried out by Carneiro DN, et al. [22], in 2016, in Jequié, Bahia-BR, where institutionalized elderly and elderly people in the community were studied, only 29.4% of nursing home residents had preserved cognitive status, while in the community the number was 82.3%. In view of the above, the result of this research goes against the grain of the literature, where it is known that the elderly who live in a long-stay institution tend to develop greater cognition and memory problems, and this discrepancy may be related to the way in which the elderly are approached and with the dynamics that are carried out in the care routine with them.
Regarding the function of the proximal and distal upper limbs, in the present study, all 31 elderly people had this function preserved, however, no articles were identified in the literature that corroborated a discussion about this result, since all the articles found were Palmar Grip Strength test to determine upper limb function.
The limitation in shoulder movement can determine muscle weakness, decreased resistance, chronic pain, and severe limitations in activities of daily living in the most severe cases. The ability to wield and perform the function of digital tweezers is essential in maintaining the ability and ability to pick up and replace light objects, manipulate utensils and write, for example [23]. The domain that assesses lower limb function uses the Timed Up and Go test for this analysis, this test is an important predictor of falls in the elderly with high reliability. This study identified that only three of the 31 elderly were able to complete the test in a time ≤10s, which is in agreement with a study with elderly people from a Long Stay Institution in Ceará, which identified that 100% of the evaluated elderly were at risk. From low to high in different percentages [24].
Another result that drew attention in this study was the number of overweight elderly people with a suggestion of dynapenia measured by the handgrip strength. Dynapenia, which is characterized by a decrease in muscle strength, has an important impact on public health because it is associated with the development of functional disabilities among the elderly, leaving them more susceptible to dependence in carrying out activities of daily living, loss of autonomy, falls and mortality [21]. A study of older adults conducted in China also using handgrip strength to determine dynapenia concluded that dynapenia alone, obesity alone and dynapenicobesity were associated with an increased risk of disability in activities of daily living and instrumental activity of daily living. Dynapenic obesity was associated with a higher risk of daily living and instrumental daily living disability, compared with dynapenia alone or obesity alone [23].
The authors of a study carried out in Rio de Janeiro, with 502 adults aged between 33 and 81 years, where 51% were women, suggested that lower muscle strength, at least in the presence of obesity, results in fewer adverse effects on bone health in older women compared to men. They also observed higher bone mineral density in obese Indian women compared to their non-obese counterparts, suggesting that the presence of obesity may benefit bone health in women when muscle strength is impaired [24]. To carry out the tracking of these health problems, in the elderly, in primary care, the physical therapist is a trained professional, and can use the Multidimensional Assessment of the Elderly for this purpose. Through this screening, these elderly people would be promptly assisted by specialists in each domain found.
The musculoskeletal changes that were the work of the physical therapist would be treated early by him, from the prescription of exercises right there in primary care or making home visits, teaching exercises to be done at home, and in more serious cases making the referral. This elderly person to a secondary level in a physiotherapy specialty, preventing future falls, fractures, hospitalizations, hospital infections and even death. In this way, the cost to the health system would be reduced by making early and low-cost identification in primary care, favoring the economy and improving the quality of life of the elderly.
A limitation of the present study was in relation to the collection of information, since, despite the fact that dynapenia was identified in 2012, by Manini TM, et al. [25], most articles on the elderly deal only with sarcopenia [26], with the existence of few articles dealing with dynapenia as a factor of decreased functional capacity in the elderly. Finally, there is still no recommendation that the institutionalized elderly undergo an assessment at the time of entering the long-stay home, and that they be constantly monitored in order to avoid their functional loss. Much is said about primary care, but there is no mention of bringing into long- stay institutions instruments that can prevent loss of function and impairment in Activities of Daily Living.
Conclusion
The multidimensional assessment of the institutionalized elderly in Pindamonhangaba, São Paulo-BR identified a high prevalence of alterations mainly related to vision, cognitive alterations and history of falls. It also identified a high prevalence of urinary incontinence and associated with this assessment, the physical examination showed a large number of overweight among the elderly and decreased hand grip strength. The results here exposed bring to the fore the importance of the multifunctional characterization of the elderly, particularly with respect to dynapenia, for a better tracking and monitoring of possible functional losses of this institutionalized elderly in a manner to develop prevention programs and direct specific treatment plans for this population. In addition, the instrument provides this broader focus for the health of the elderly as a whole, allowing actions to reduce losses in activities of daily living.
References
-
World Health Organization (2005) Active aging: a health policy. Pan American Health Organization, Brazil.
-
Cancela EMC (2007) The aging process.
-
Rebellato JR, Morelli JGS (2007) Geriatric Physiotherapy- The practice of assisting the Elderly. In: 2nd (Edn.), Manole.
-
Chagas AM, Rocha ED (2012) Physiological aspects of aging and contribution of Odontology to the health of elderly. Rev Bras Odontol 69(1): 94-96.
-
Freitas VE, Py L (2016) Treatise on geriatrics and gerontology.
-
Papalleo Netto M (2005) Physiology of aging. Geriatrics: fundamentals, clinical and therapeutics. Athena.
-
Fechine Basílio RA, Trompieri N (2012) The aging process: the main changes that happen to the elderly over the years. International Scientific Journal 20(1): 106-194.
-
Clark BC, Manini BM (2008) Sarcopenia =/= dynapenia. The Journal of Gerontology, Series A: Biological Sciences and Medical Sciences 63(8): 829-834.
-
Sirena SA (2002) Multidimensional assessment of the elderly: an approach in primary health care. PUCRS.
-
Mancini RB, Silva Junior JP, Araujo TL, Matsudo SM, Matsudo V (2019) Prevalence and factors associated with dynapenia in institutionalized elderly. A cross- sectional study. Diagn Tratamento 24(3): 111-118.
-
Silva AM, Shen W, Heo M, Gallagher D, Wang Z, et al. (2010) Ethnicity-related skeletal muscle difference across the lifespan. Am J Hum Biol 22(1): 76-82
-
Reis DLA, Church PN, Silva Moia MY, Souza Reis CA, Sousa Borges RC, et al. (2020) Quick multidimensional evaluation applied to elderly people from a long- stay institution in Tucuruí-PA. Brazilian Journal of Development 6(3): 12018-12034.
-
Silva RS, Fedosse E, Pascotini FS, Riehs EB (2019) Health conditions of institutionalized elderly: contributions to interdisciplinary action and health promoter. Brazilian Notebooks of Occupational Therapy 27(2): 345-356.
-
De Nadai RAA, Gonçalves GB (2019) Analysis of balance and postural control in visual disabilities acquired. Brazilian Journal of Health Review 2(3): 1754-1772.
-
Ribeiro JEC, Freitas MM, Araujo GS, Rodrigues Rocha TH (2004) Association between depressive features and visual deficit caused by cataracts in elderly patients. Arch Brazil Ophthalmol 67(5): 795-799.
-
Silva BSR, Sousa GB, Pacheco Russo IC, Ribeiro da Silva JAP (2007) Characterization of the complaints, kind of hearing loss and treatment for elderly people seen at a private clinic in Belem-PA. Intl Arch Otorhinolaryngol 11(4): 387-395.
-
Russo ICP (1999) Speech therapy intervention in old age. Revinter.
-
Fernandes LC, Silva Fernandes VL, Costa MN, Siqueira A, Menezes RL (2016) Elderly Institutionalized: Frailty and without Balance. Resu-Education in Health Magazine 4(2): 95-102.
-
Tribess S, Oliveira RJ (2011) Biological fragility syndrome in the elderly: systematic review. Rev Public Health 13(5): 853-864.
-
Souza NS, Martins ACG, Machado D de CD, Dias KP, Nader S, et al. (2012) The influence of the visuo-podal axis on the regulation of morphostatic balance in the elderly. Neuroscience Journal 20(2): 320-327.
-
Roig JJ, Bezerra Souza DL, Andrade FL, Lima Filho BF, Medeiros RJ, et al. (2016) Self-perception of health in institutionalized elderly. Science & Public Health 21(11): 3367-3375.
-
Carneiro DN, Vilela ABA, Meira SS (2016) Evaluation of Cognitive Deficit, Mobility and Activities of Daily Life among Elderly People. Revista de APS 19(2): 203-209.
-
Yang M, Ding X, Luo L, Hao Q, Dong B (2014) Disability associated with obesity, dynapenia and dynapenic- obesity in chinese older adults. J Am Med Dir Assoc 15(2): 150.e11-150.e16.
-
Chain A, Faerstein E, Wahrlich V, Bezerra FF (2021) Obesity, dynapenia, and their combination: Implications for boné mineral density in Brazilian adults-the Pró- Saúde study. Nutrition 81: 110898.
-
Clark BC, Manini TM (2012) What is dynapenia? Nutrition 28(5): 495-503.
-
Laurentani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, et al. (2003) Age associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol 95(5): 1851-1860.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria