Human Immune Virus (HIV) Infection among Children, Treatment and Under-5 Deaths in Nigeria: An Empirical Analysis
Purpose: This study investigates the impact of Human Immune Virus (HIV) infections among children and under-5 deaths in Nigeria. Since the prevalence of HIV infection, Nigeria health care and the government has experienced many challenges towards achieving healthy outlook among the citizens and this struggle has continued over the years, with the consideration of the thunderous increase of the under-5 deaths caused by HIV infections in Nigeria. Therefore, this study investigates HIV infections, its treatment and under-5 deaths in Nigeria and contributes a way forward towards recuperation in achieving a healthy society among Nigerians. Design/Methodology/Approach: This study used the Ordinary Least Square (OLS) method to investigate the impact of HIV infections among children on under-5 deaths in Nigeria. Being an empirical study, the data used for its analysis were annual secondary data and they were obtained from World Bank indicators which is a reliable source. Findings: The findings from the result of the OLS method of analysis prove that HIV infections increase under-5 deaths at 1% significant level in Nigeria. The result also proved that treatment of HIV victims definitely reduces under-5 deaths in Nigeria at 1% significant level.
Introduction
The prevalence of diseases and their existence have become a great concern to humanity. Human Immune Virus/ Acquired Immune Deficiency Syndrome (HIV/AIDS) which is an infectious disease and one of the killer diseases in the world has become a night mare to those in Africa, especially Nigeria. As a result of the negative impact this disease has created in Nigeria society and the world at large, scholars and biological science researchers have deepened scientific investigation on efforts to eradicate HIV/AIDS from its prevalence in the world. Also, with understanding that HIV/ AIDS is a virus disease that runs in the blood of the infected person and could not have a complete cure for its eradication, scientist also went on to investigate for a remedial solution (Antiretroviral treatment) that an infected person will apply for sustenance. But, it is a pity that all these efforts by biological scientist proves to be abortive because HIV/AIDS
continues to prevail and kill in thousands annually, UNAIDS (2018) [1].
In 2005, approximately 40.3 million Nigerians were living with HIV/AIDS out of the total population of Nigeria in the same year. Nigeria was ranked as the world’s third largest disease-burden country as well the second largest HIV/AIDS epidemic country in the world, WHO (2005). Also in 2017, about 150,000 people died from HIV/AIDS in Nigeria while in 2018 about 1.9 million people of the total Nigeria population were living with HIV/AIDS, UNAIDS (2018) [1]. The mortality rate as a result of HIV/AIDS prevalence continue to increase in Nigeria irrespective of the Millennium Development Goals (MDGs) target against HIV/AIDS which Nigeria is a member country that emancipated the implementation of the MDGs which one of its target was the fight against HIV/AIDS and other infectious diseases. With obvious understanding on the failure of Nigeria for achieving this target of the MDGs, against HIV/AIDS which ended in 2015, the sustainable development goals (SDGs) kicked off and it is also another world emancipated strategy which one of its key target is the total limitation of HIV/AIDS prevalence among people in different countries. But seeing the continuous prevalence of HIV/AIDS in Nigeria, it is hard to believe that Nigeria will achieve the SDGs target against HIV/AIDS before the year 2030.
In Nigeria, 58% of the women population is estimated to be living with HIV. Women and girls are the most affected by HIV because of gender inequality that exist in Nigeria Society. Not only that, most of these women and girls that are affected with HIV are also pregnant women, and breast feeding mothers, lingering the prevalence of HIV/AIDS diseases to their children. Thus, causing under-5 mortality rate to be high in Nigeria recently. Nigeria under-5 mortality rate is from 281.4 deaths per 1000 live births in 1970 and 117.2 deaths per 1000 live births in 2019 as well 95.12 deaths per 1000 live births in 2020. This simply implies that one out of ten children born in Nigeria never reached the age of 5 years, WHO (2021).
The decrease associated with under-5 mortality rate in Nigeria is not as expected because of the world advancement on health care industries which Nigeria is not exceptional and is also upgrading to suit the need of the citizens on health care affairs. The cause of this high under-5 mortality rate in Nigeria becomes worrisome because government efforts to protect the infants and under-5 children seems meaningless irrespective of all the efforts government is making to provide all the basic needs of man relating to health improvements in Nigeria. This led to the motivation of this study to check if HIV/AIDS, which is a killer disease has effect on the under-5 mortality rate in Nigeria. The Figure 1 shows the number of children (ages, 0-14 years) living with HIV/AIDS and newly infected with HIV/AIDS as well number of under-5 deaths in Nigeria.
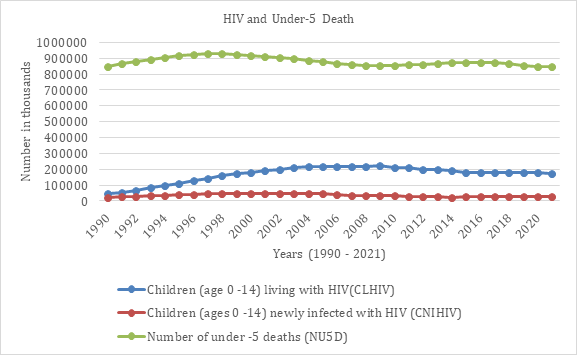
Source: World Bank data, 2022. Figure 1: HIV infections and under-5 deaths in Nigeria-(1990-2021).
Figure 1 shows the number of children from the age of 0–14 years living with HIV and also newly infected with HIV annually. It is shows the number of under-5 deaths in Nigeria from 1990 to 2021. It clearly indicates that the annual number of under-5 deaths is higher than the annually number of children living with HIV and newly infected with HIV. This indication is a prove that there are other related issues that may cause under-5 deaths in Nigeria such as malnutrition, fever, meningitis and other related health issues. But it is obvious that the prevalence of HIV among the children contributes and accelerates to their deaths.
HIV/AIDS infection remains the most public health crises in Nigeria, a country in which more people living with HIV/AIDS are high compared to other countries of the world with the exception of South Africa and India. In addition, the international health initiatives targeted many countries which Nigeria was included for the treatment and expansion of the antiretroviral therapy (ART) programs for the increasing number of affected patients. It is to be believed that the success of the ART initiatives will depend on the treated patients’ continual adherence to antiretroviral (ARV) drugs. Nevertheless, studies in Nigeria explained that only few among those infected with HIV/AIDS adhered to the treatment with ART and ARV which had a mix mode, that is both high and low adherence to treatment. The reasons for non-adherence were identified and the most common reasons for the patient non-adherence to treatment were, cost of therapy, medication side effects, non-availability of ARV drugs, and the stigma of taking the drugs, Monjok E, et al. [2].
Figure 2, explains the percentage of the pregnant women and the entire people in Nigeria who have access to ART treatment from 1990 to 2021. The figure shows that there were no treatments of patients living with HIV/AIDS in Nigeria from 1990 until 2003. The worst of it is that pregnant women who were infected with HIV, could not access as well the antenatal treatment because they are HIV carriers. The scenario contributed the increase of HIV infections in Nigeria till date. Also those who were opportune to access the ART treatment failed to adhere to the doctor’s advice on measures to administer the treatment, such action leading to the worsening of the situations of the HIV infection in Nigeria.
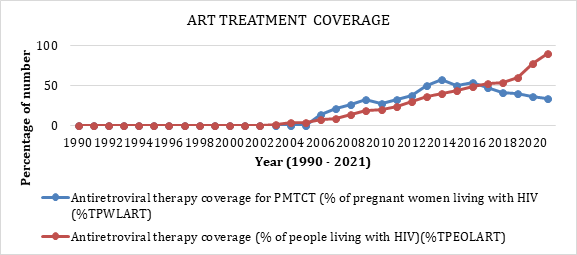
Source: World Bank Data, 2022. Figure 2: ART Coverage in Nigeria (1990-2021).
Therefore, Nigeria and Nigerians are indeed in a mess with the prevalence of HIV. In addition, this study contributes to the current literature by looking into the impact or role HIV/AIDS prevalence plays in the number of under-5 deaths in Nigeria. Most of the literatures have not or gave a little attention to the relationship associated with under-5 deaths and HIV/AIDS prevalence in Nigeria, forgetting to understand that the young ones are the futures of our tomorrow, hence this study will consider the gap. Having considered all these issues, this paper emancipated to answer the question, does the prevalence of HIV/AIDS contributes to under-5 deaths in Nigeria? This study will answer this question through its objective which is “to investigate the impact of HIV/AIDS prevalence and under-5 mortality in Nigeria”. This study has five sections, section one is the introduction, section two is the literature review, and section three is the methodology used in the study while section four is the result analysis and finally section five is the conclusion of the study.
Literature Review
Theoretical Review
Considering the biological science theories, and looking at theory of epidemiology transition, Omran AR [3], is a theory which describes the changes in population patterns in terms of fertility, life expectancy, mortality and leading causes of death. Epidemiological concept is a quantitative science concerned with infectious diseases, with the circumstances under which diseases processes occur, the factors that affects their incidence and the host response to which the infectious agent, and the use of this knowledge for control and prevention.
Therefore, the theory of epidemiology transition concisely explains about the changes in population as a result of deaths caused by HIV/AIDS prevalence. It is an infectious disease, and the theory explains the process in which HIV/ AIDS occurs, the factors affecting the treatment of HIV among carriers and the control of the HIV infections. The theory of epidemiological transition explains the ideology associated with this study which is to investigate the outcome relating HIV and under-5 mortality rate in Nigeria.
Empirical Review
The connection between HIV/AIDS and under-5 mortalities has attracted fewer awareness through current research. The prevalence of HIV/AIDS that exerts influence directly on under-5 mortality has many causes and different countries have different reasons leading to the incidence of HIV/AIDS prevalence.
Eduardo V, et al. [4] on their study titled “ Child mortality in relation to HIV infection, nutritional status, and socio-economic background, examine the impact of child HIV infection on mortality and to identify nutritional and sociodemographic factors that increase the risk of child mortality independent of human immunodeficiency virus (HIV) infection” using primary data method of analysis concluded that HIV infection was associated with an adjusted 4-fold higher risk of mortality and HIV infection appeared to be a stronger predictor of mortality among children who were wasted than among those who were not.
Another study is Weldemariam SA, et al. [5], which is titled “Time to death among HIV-infected under-five children after initiation of anti-retroviral therapy and its predictors in Oromiya liyu zone, Amhara region, Ethiopia: A retrospective cohort study”, using a primary data methods of collection and multivariable Cox-proportional hazard regression model conducted a study among 376 under-5 HIV infected children who are on antiretroviral therapy from January 2014 to December 2019, Oromia Liyu Zone Amhara region in Ethiopia. The result of this study indicated that approximately 81% of HIV infected children were alive, 11% were lost to follow up, 3.2% were transferred out while 5.6% were dead due to HIV/AIDS. The study also proved that the overall mean time to death was 19.7 months with incidence of 5.9 deaths per 100 children in a month. It concluded that poor adherence to ART were significantly associated to high mortality events and death of HIV-infected under-five children on ART is high within the first one year after enrolment.
Cuddington JT [6] study was on modelling the macro- economic effects of AIDS using the Solow framework and he focused on one country, Tanzania. This study reported that the rise of HIV/AIDS deaths had reduced labour productivity, leading to the high rate of healthcare cost and investment which reduced savings and consumption expenditure. Such a scenario is reported to be linked to reduced human capital investment at the family level due to the inability to afford the healthcare cost. Cuddington JT [6] also explained that an increase in mortality as a result of infectious diseases would lead to reduced average age and experience of the working population, leading to a reduction in average productivity and economic growth. This will likely increase the dependency ratio due to the deaths of many working- aged people. Cuddington JT [6] concludes that the presence of AIDS in Tanzania may lower the per capita income by up to 11% annually.
Methodology and Data
This area of study will explain the model used in this study, it will also explain the methods of this study analysis that helped this study to arrive at a conclusion as well explain about the data used and their sources.
Empirical Model Specification
The model specification simply specifies the function that expresses the relationship between the HIV infections and under-5 mortality variables as well with the other independent variables to help this study achieve its objective. We acknowledge and emulate a simple mathematical/ economic function stated by Cobb CW, et al. [7] output (Y) is a function of inputs (K) for capital and (L) for labour and it is stated below as:
Y = KαLβ (1) In equation 1, β and α estimates the proportion of capital and labour used for the level of output (Y) achieved. Therefore, this study expresses the impact of HIV infections as an input to the outcome of under-5 mortalities in consideration with the ART exercise during the study period. The advantage of this function form is that under-5 mortalities depends on the level of HIV infections. Therefore, this study model is stated as NU5D = CLHIVβ1CNIHIVβ2 TPWLARTβ3TPEOLARTβ4 (2) Where NU5D = Number of under -5 deaths, CLHIV = Children (age 0 -14) living with HIV, CNIHIV = Children (ages 0 -14) newly infected with HIV, TPWLART = Antiretroviral therapy coverage for PMTCT (% of pregnant women living with HIV and TPEOLART = Antiretroviral therapy coverage (% of people living with HIV). β1, β2, β3 and β4 measures the rate of the independent variable incidences within the period of this research. Statistically, Equ (2) is reduced to the form NU5D = Z + β1CLHIVt + β2CNIHIVt + β3TPWLARTt + β4TPEOLARTt + ɛt (3) And equation 3 is modified and reduced to natural logarithm to help the interpretation of the coefficient estimated results of the variables in the model and its reduction into the natural logarithm is written and stated as InNU5D = Z + β1InCLHIVt + β2InCNIHIVt + β3InTPWLARTt + β4InTPEOLARTt + ɛt (4) Where Z = intercept; In = natural logarithm; t = time; ɛ = error term; β1, β2, β3 and β4 are the coefficient of the independent variables.
Methodology
The methodology used in this study depends on the outcome of the unit root test result conducted among the variables to know their stationary characteristics. The unit root test is conducted to know if the variables in the model are stationary at the level I(0), the first difference I(1) or mix mode, that is if the variables are stationary at both I(0) and I(1). If all the variables are stationary at I(0), this study will not use the ARDL model approach for its estimation, rather the Ordinary Least Square (OLS) approach will be used because variables exhibit their stationarity at I(0) suits the OLS method of analysis. Also if the variables are stationary at I(1) or mix mode, then the ARDL method suits the analysis. Moreover, the ARDL method has the advantage over other methods like the OLS in the estimation of linear relationships among variables because the lag of the dependent variable can be used as an independent variable in the estimation process. Other methods of analysis lack this characteristic.
After conducting the unit root test, it proved that the variables in the model are stationary at level I (0), therefore this study continued to adopt the OLS. Also, this study suits the use of OLS method for its analysis because the lag of the dependent variable is not included in the model. Estimation of the coefficient relationship is performed to find out the equilibrium relationship that exists between the dependent and independent variables. The formula is thus $$ \begin{array}{l} \mathrm {I n N U 5 D} _ {\mathrm {t}} = A + \sum_ {i = 1} ^ {p} \beta_ {1} \mathrm {I n N U 5 D} _ {\mathrm {t - i}} + \sum_ {i = 0} ^ {q} \beta_ {2} \mathrm {I n C L H I V} _ {\mathrm {t - i}} + \sum_ {i = 0} ^ {r} \beta_ {3} \mathrm {I n C N I H I V} _ {\mathrm {t - i}} \\ + \sum_ {i = 0} ^ {s} \beta_ {4} \mathrm {I n T P W L A R T} _ {\mathrm {t - i}} + \sum_ {i = 0} ^ {T} \beta_ {5} \mathrm {I n T P E O L A R T} _ {\mathrm {t - i}} + \varepsilon_ {\mathrm {t}} \\ \end{array} $$ (5) After the estimation of the coefficient relationship that exists among the variables in the model, the next test to be done is the diagnostics test which comprises of the serial correlation, heteroscedasticity and normality test to check if there is any serial or auto correlation problem, constant variance problem and normality distribution problems in the models used to explain the relationship between the dependent and independent variables in the model after the coefficient analysis test.
Data Sources and Justification of the Sample Size
Data sources are very important in every research mostly when the data collection is secondary. This study used secondary data collection method and all the data were collected from World Bank. The data are annual time series starting from 1990 to 2021 which is 32 years of observation Table 1.
| Data | Source | Measurement | |
|---|---|---|---|
| 1 | Children (ages 0 -14) living with HIV (1990 – 2021) (CLHIV) | World Bank | Total number of Children between the age of 0 to 14 years that are living with HIV in Nigeria |
| 2 | Children (ages 0 -14) newly infected with HIV (1990 – 2021) (CNIHIV) | World Bank | Total number of Children between the age of 0 to 14 years that are newly infected with HIV in Nigeria |
| 3 | Antiretroviral therapy coverage for PMTCT (% of pregnant women living with HIV) (1990 – 2021) (TPWLART) | World Bank | Percentage number of the pregnant women living with HIV that receives ART in Nigeria. |
| 4 | Antiretroviral therapy coverage (% of people living with HIV) (1990 – 2021) (TPEOLART) | World Bank | Percentage number of the total people living with HIV that receives ART in Nigeria. |
| 5 | Number of under -5 deaths (1990 – 2021) (NU5D) | World Bank | Total number of Children that died in Nigeria before the age of 5 years. |
Table 1: Data Sources and Justifications.
Table 1 presents the sources and justifications of the variables used in this study. The dependent variable is NU5D. The independent variables are CLHIV, CNIHIV, TPWLART and TPEOLART.
Result Estimation
Descriptive Statistics
The descriptive statistics value of this study is found in Table 2 below. It shows the variables and their years of observation, the mean, standard deviation, minimum and maximum values used in the study.
| Variable | Obs. | Mean | Std. Dev. | Max. | Min |
|---|---|---|---|---|---|
| NU5D | 32 | 880951.9 | 26750.06 | 927731.0 | 844321.0 |
| CLHIV | 32 | 169343.8 | 51679.29 | 222000.0 | 44000.0 |
| CNIHIV | 32 | 34687.50 | 8125.775 | 46000.00 | 22000.0 |
| TPWLART | 32 | 18.62500 | 20.73761 | 57.00000 | 0.00000 |
| TPEOLART | 32 | 19.68750 | 25.75748 | 90.00000 | 0.00000 |
Table 2: Descriptive Statistics.
Note: OBS = observation; Std.Dev = Standard Deviation; Max = Maximum; Min = Minimum; NU5D = number of under-5 deaths; CLHIV = number of children living with HIV/AIDS; CNIHIV = number of children newly infected with HIV; TPWLART = total percentage number of pregnant women living with HIV that receives ART treatment and TPEOLART = the total percentage number of people living with HIV that receives ART treatment in Nigeria. Table 2: Descriptive Statistics.
The descriptive statistics values show that NU5D has the highest maximum value of 927731.0 as well has the highest minimum value, proving that NU5D is high in Nigeria.
Covariance Matrix
Table 3 below is the covariance matrix table. It shows the diagonal relationship among the variables used in this study model. For example, the relationship between NU5D and CNIHIV is positive with the value of 1.63E8 indicating that increase in CNIHIV leads to increase in NU5D, and also consider the relationship between NU5D and TPWLART which has a negative value of -337353.0 which implies that increase in the percentage number of pregnant woman receiving ART reduces NU5D.
The covariance matrix coefficient relationship does not give a complete analysis of the relationship among the variables. This study will continue with other necessary analysis needed to ascertain the objective of this study.
| E(V) | NU5D | CLHIV | CNIHIV | TPWLART | TPEOLART |
|---|---|---|---|---|---|
| NU5D | 6.93E8 | ||||
| CLHIV | -2.59E8 | 2.59E9 | |||
| CNIHIV | 1.63E8 | 86607422 | 63964844 | ||
| TPWLART | -337353.0 | 432347.7 | -119335.9 | 5201458 | |
| TPEOLART | -409084.3 | 345294.9 | -130316.4 | 425.5703 | 642.7148 |
Table 3: Covariance Matrix of coefficient of NU5D model.
Note: NU5D = number of under-5 deaths; CLHIV = number of children living with HIV/AIDS; CNIHIV = number of children newly infected with HIV; TPWLART = total percentage number of pregnant women living with HIV that receives ART treatment and TPEOLART = the total percentage number of people living with HIV that receives ART treatment in Nigeria. Table 3: Covariance Matrix of coefficient of NU5D model.
Unit Root Test
The unit root test of this study was performed using the Augmented Dickey Fuller (ADF) test to find the stationary properties of the variables used in this study. The Philip Perron (PP) unit root test was also conducted in conformity with the ADF test result.
Table 4 is the unit root test results of the variables in the model for this study. It shows that for the ADF, all the variables are significantly stationary at the level I(0). Also for the PP unit root test, only CLHIV and TPEOLART were significantly stationary at level I(0). Therefore, the result of the unit test is in agreement with the OLS model testing approach.
| ADF TEST | PP TEST | |||
|---|---|---|---|---|
| Variables | ||||
| Level I(0) | 1st Difference I(1) | Level I(0) | 1st Difference I(1) | |
| NU5D | -4.0996** | -1.8317 | -1.5149 | -2.0300 |
| CLHIV | -2.7800* | -0.8401 | -3.1498** | -1.3780 |
| CNIHIV | -4.1478*** | -2.4743 | -1.6430 | -2.3471 |
| TPWLART | -3.4718** | -1.3809 | -0.9126 | -3.7593 |
| TPEOLART | 3.4591** | 0.9249 | 6.0875*** | -0.8038 |
Table 4: Unit Root Test Result.
Note: Significant level *10%, 5%, and *1% respectively. NOTE: Obs = observation; Std.Dev = Standard Deviation; Max = Maximum; Min = Minimum; NU5D = number of under-5 deaths; CLHIV = number of children living with HIV/AIDS; CNIHIV = number of children newly infected with HIV; TPWLART = total percentage number of pregnant women living with HIV that receives ART treatment and TPEOLART = the total percentage number of people living with HIV that receives ART treatment in Nigeria. Table 4: Unit Root Test Result.
OLS Estimated Long-Run Coefficient Test
The long-run coefficient test is important to run in the OLS model. It is performed to determine the connection and behavioural relationship between the dependent and independent variable in the long-run. The results are tabulated in Table 5 below.
| Variables | Coefficient | Probability |
|---|---|---|
| LCLHIV | -0.2183*** | 0.0005 |
| LCNIHIV | 0.0114 | 0.6946 |
| LTPWLART | 0.0396*** | 0.0036 |
| LTPEOLART | -0.0407*** | 0.0000 |
Table 5: Coefficient Estimation-NU5D Model.
Note: *, and * means significant at 10%, 5% and 1% respectively. LCLHIV = Log of number of children living with HIV/AIDS; LCNIHIV = Log of number of children newly infected with HIV; LTPWLART = Log of total percentage number of pregnant women living with HIV that receives ART treatment; LTPEOLART = Log of the total percentage number of people living with HIV that receives ART treatment in Nigeria Table 5: Coefficient Estimation-NU5D Model.
The long-run coefficient test was done to achieve the objective of this study which was to investigate the impact of HIV infections among children on under-5 deaths in Nigeria. The result in table 5 shows that NU5D has a negative relationship with CLHIV, which means increase in the number of under-5 deaths leads to decrease in the number of children living with HIV/AIDS. This simply means that children living with HIV/AIDS constitutes among the number of under-5 deaths in Nigeria. Also the coefficient value of CLHIV is -0.2183, that means for every 21% increase of NU5D, there is 1% decrease of CLHIV and it is significant at 1%.
Also, CNIHIV which is the number of children newly infected with HIV has a positive relationship with NU5D. That means increase in CNIHIV leads to increase in NU5D. This result is true because when the number of children newly infected with HIV increases, there is tendency for the number of under-5 deaths to increase. The coefficient of CNIHIV is 0.0114, which means any 1% increase of CNIHIV will lead to 1% increase of NU5D but not significant.
Additionally, TPWLART is the total percentage number of pregnant women living with HIV that receives ART treatment. The coefficient of TPWLART is 0.0396 which indicates a positive relationship with NU5D. It means increase in TPWLART brings increase to NU5D. And any 3% increase of TPWLART leads to 1% increase of NU5D. Finally, TPEOLART is the total percentage number of people living with HIV that receives ART treatment in Nigeria. The coefficient of TPEOLART is -0.0407 indicating a negative relationship between TPEOLART and NU5D. It means increase in total percentage of people living with HIV that receives ART treatment (TPEOLART) leads to decrease in number of under-5 deaths (NU5D), and any 4% increase of TPEOLART leads to 1% decrease of NU5D at 1% significant level.
Diagnostic Test
The diagnostic test for this study are the serial correlations test which helps to check if there is any serial correlation among the variables in the model of this study. Also the next is the heteroscedasticity test which is conducted to check if there is any constant variance in the regression model, and the normality test is to confirm that all the variables in the model are normally distributed and placed. Table 6 shows the summary of the diagnostic test results for this study.
| Obs*R-square | Prob. Chi-Square | |
|---|---|---|
| Serial Correlation LM Test | 1.1375 | 0.5662 |
| Heteroscedasticity test | 5.7851 | 0.2158 |
| Normality Test | 1.8942 | 0.3878 |
Table 6: Diagnostic Test-NU5D Model.
As tabulated in Table 6 the NU5D Model, serial correlation LM test showed that the Obs*R-square was 1.1375 which is higher than the probability value of 0.5662, and its percentage value of 56.6% is above the 10% significance level. It implies that at 56.6%, this study proves there is no serial correlation in the study model. Also the Heteroscedasticity test has its Obs*R-square to be 5.7851 which is above the probability value of 0.2158, having its percentage value as 21.5% which is above the 10% significant level. It means that at 21.5% there is no constant variance in the model used for this study. Finally, the normality test which has its Obs*R-square value as 1.8942 which is higher than the probability value of 0.3878 proves that at 38.7% there is no problem of normality in the model. Therefore, the variables in the model are normally distributed.
Discussion
It is a fact that the number of children being infected with HIV have been at alarm in Nigeria over the period of this study. Also this study has clearly proved that as a result of increase in the number of children being infected with HIV, the number of under-5 deaths have been at increase. This is proved from the result of this study which indicated a positive relationship between number of children infected with HIV and number of under-5 deaths in Nigeria at table 5. Also, increase in the number of pregnant women infected with HIV have contributed to the increase of number of children living with HIV, this is proved in table 3 where both variables have a positive correlation of 432347.7. Finally, non-availability of the ART therapy for those living with HIV in Nigeria contributes to the tremendous increase of HIV infections and incidences among Nigerians, and this study have clearly enlightened the loopholes where the Nigeria government should put into consideration in efforts to reduce/stop the manifestation of HIV infection among Nigerians.
Conclusion
This study investigated the impact of HIV infections and treatment among children and under-5 deaths in Nigeria. The motivation for this study resulted from the continuous prevalence of HIV/AIDS infections and the high rate of under-5 deaths in Nigeria irrespective of the measures government have put in place to control the menace. If this trend continues, Nigeria in the future will lack huge number of youths which are the engine working population force that helps to develop the country. There, this study has come to the following conclusions. First, HIV infections have a great impact and it has contributed immensely to under-5 deaths in Nigeria, because the higher the number of newly infected people with HIV, the higher the number of under-5 deaths in Nigeria. Secondly, the percentage number of people receiving treatment has a negative relationship with under-5 deaths which implies that if the people who are infected with HIV were able to receive appropriate treatment, then the number of under-5 deaths will definitely reduce and people and children will not be dying easily as a result of HIV infections.
Policy Recommendation
For the Nigeria government to be in full control of HIV infections, there is need for creating of awareness and educating of people on the issues relating to HIV infections, ways to avoid being infected, its treatment and sustenance if one is infected. This will help the public to understand the contagious disease HIV. Secondly, the treatment of HIV (Antiretroviral Therapy) should be free of charge to all citizens as well make the treatment centres available to a common man. This is because some people who have been infected with HIV could not be able to access the centres where treatments are given and many could afford for the cost of the treatment, such condition will continue to linger the prevalence of HIV if the infected people are not treated and its prevalence not controlled.
Under-5 deaths which is at increase should be controlled by the government by providing special and adequate health care facilities for children. Some parents in Nigeria are poor and they cannot be able to afford taking their children to hospitals for appropriate treatment when they are sick, hence this scenario increase the under-5 deaths in Nigeria. Therefore, poverty among Nigerians have also been a tool for under-5 deaths in Nigeria, hence there is need for government to consider this effects.
Limitations of Study
There are some limitations that this study undergone. There was a need for a proxy to get the exact number of under-5 children that are receiving treatment for HIV annually, but such proxy was not obtained hence this study used total number of people (Adult and Children) that are receiving HIV treatment in Nigeria annually. Secondly this study considered only the under-5 children in its investigation, hence there is need for children beyond the age of 5 to be investigated as well.
Acknowledgements
All cited papers for this manuscript are completely acknowledged. There is a complete compliance on ethical standards and there is no conflict of interest in this study.
References
-
UNAIDS (2018) 2018 Progress reports submitted by countries. GENEVA.
-
Monjok E, Smesny A, Ita BO, Osaro M, Essien EJ (2010) Adherence to antiretroviral therapy in Nigeria: an overview of research studies and implications for policy and practice. HIV AIDS (Auckl) 2(1): 69-76.
-
Omran AR (2005) The epidemiologic transition: A theory of the epidemiology of population change. Milbank Quarterly 83(4): 731-757.
-
Eduardo V, Lara M, Fataki MR, Mbise RL, Fawzi WW (2005) Child mortality in relation to HIV infection, nutritional status, and socio-economic background. International Journal of Epidemiology 34(1): 61-68. **5.** Weldemariam SA, Dagnew Z, Tafere Y, Bereka TM, Bitewa YB (2022) Time to death among HIV-infected under- five children after initiation of anti-retroviral therapy and its predictors in Oromiya liyu zone, Amhara region, Ethiopia: A retrospective cohort study. BMC Pediatr 22(5): 5.
-
Cuddington JT (1993) Modeling the macro-economic effects of AIDS, with an application to Tanzania. The World Bank Economic Review _7_(2): 173-189.
-
Cobb CW, Douglas PH (1928) A Theory of Production. The American Economic Review 18(1): 139-165.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria