Increased Incidence in Gestational Diabetes Mellitus by Race and Ethnicity during the COVID-19 Pandemic: Results from a Large Medical Center in the United States
Background: Gestational diabetes mellitus (GDM) is a common pregnancy complication, and its risk increases in females exposed to stressful events. The COVID-19 pandemic has affected the healthcare system and individuals’ behaviors, but its impact on GDM risk remains unclear. We aimed to investigate the influence of the pandemic on GDM risk in the United States (US), overall and by race/ethnicity. Methods: This retrospective cohort study included pregnancies in an academic medical system in Los Angeles, California. We divided 8,518 pregnancies into the pre-COVID cohort (4,507 delivered between 9/1/2018 and 2/29/2020; 18 months) and the intra-COVID cohort (4,011 delivered between 3/1/2020 and 8/31/2021; 18 months). We ascertained GDM cases using the ICD-10 codes, calculated the age-standardized GDM incidences, and estimated the risk ratios (RR) of GDM (intra-COVID vs. pre-COVID) using Poisson regressions. Results: The age-standardized GDM incidence was 8.49% in the pre-COVID and 10.02% in the intra-COVID cohorts. The GDM risk was 17% higher in the intra-COVID cohort than in the pre-COVID cohort (RR=1.17; 95% CI: 1.02, 1.35) after adjusting for race/ethnicity, maternal age, nulliparity, marital status, pre-pregnancy body mass index, gestational weight gain, and utilization days of prenatal care. When stratified by race/ethnicity, the GDM risk was higher in non-Hispanic Whites (RR=1.34; 95% CI: 1.03, 1.74), Hispanics (RR=1.26; 95% CI: 1.00, 1.59), and potentially in non-Hispanic Blacks (RR=1.32; 95% CI: 0.63, 2.76), but not in Asians (RR=0.99; 95% CI: 0.75, 1.30). Conclusion: GDM incidences increased during the COVID-19 pandemic in a large US city, especially among non-Hispanic Whites, Hispanics, and non-Hispanic Blacks.
Introduction
Gestational diabetes mellitus (GDM), hyperglycemia first detected during pregnancy, is one of the most common pregnancy complications [1, 2]. It affects 4-9% of pregnancies in the United States (US), and its incidence has continued to rise over the past 40 years [3, 4, 5, 6, 7]. GDM has well-documented racial and ethnic disparities, with Asian and Hispanic females having 2-3 times higher risk than non-Hispanic White females [2, 3, 8]. Moreover, GDM has been associated with a variety of short-term and long-term adverse health outcomes in both mothers (e.g., pre-eclampsia, type 2 diabetes mellitus, and cardiovascular diseases) and their offspring (e.g., large for gestational age at birth, metabolic syndrome, and autism spectrum disorder [9, 10, 11, 12, 13, 14]).
Multiple lifestyle and psychological factors are risk factors for GDM, including pre-pregnancy obesity, poor diet, lack of physical activity, depression, stress, and anxiety [2]. The COVID-19 pandemic had a significant impact on healthcare access and quality as well as lifestyle [15, 16, 17] and psychological factors related to GDM risk [18]. A few studies have reported a rise in GDM rates during the COVID-19 pandemic compared to the pre-pandemic period [19, 20, 21, 22, 23]. However, most of these studies did not adjust for potential confounders, focused only on the initial pandemic period (i.e., the lockdown window or during 2020), and did not explore the underlying reasons (e.g., SARS-CoV-2 infections) for the observed increase in GDM rate during the COVID-19 pandemic. Blacks and Hispanics have experienced disproportionally higher rates of SARS-CoV-2 infection [24] and have had more undesired changes regarding health behaviors during the COVID-19 pandemic [16] in the US; however, no previous studies have examined the COVID-19 pandemic impact on GDM rates by race and ethnicity. Therefore, this study aimed to examine the COVID-19 pandemic’s impact on the risk of GDM and whether racial and ethnic groups were affected differently by the COVID-19 pandemic in the US.
Materials and Methods
This retrospective cohort study leveraged electronic medical records (EHR) from a large academic medical system with multiple hospitals and clinics in Los Angeles, California. It has over 2.5 million annual visits and 100,000 annual hospital admissions for patients from socioeconomically diverse backgrounds. We identified pregnancies (N = 8,691) between 24-44 gestational weeks (GW) from 9/1/2018 to 8/31/2021 (36 months). We excluded 173 pregnancies with pre-pregnancy diabetes (International Classification of Diseases, 10th edition [ICD-10] codes: E10.x, E11.x, E13.x). The final analytical sample included a total of 8,518 pregnancies from individuals aged 15-49 years. The study was approved for exemption by the University of California, Los Angeles Institutional Review Board (IRB #20-001806).
We divided the overall sample into the pre-COVID cohort (4,507 pregnancies delivered between 9/1/2018 and 2/29/2020 [18 months]) and the intra-COVID cohort (4,011 pregnancies delivered between 3/1/2020 and 8/31/2021 [18 months]) according to delivery dates (Figure 1). In our healthcare system, all pregnant individuals were screened for GDM during 24-28 GW. We ascertained GDM cases using the ICD-10 codes (O24.4x). We validated the GDM diagnosis by the ICD-10 codes using the plasma glucose values obtained during the GDM screening using the Carpenter & Coustan criteria among those with laboratory data (~60%). We also extracted the sociodemographic (e.g., maternal age, race and ethnicity, and marital status), anthropometric measures (e.g., pre-pregnancy body mass index [BMI]), pregnancy outcomes (e.g., gestational weight gain and gestational weeks at delivery), and utilization of prenatal care from the EHR.
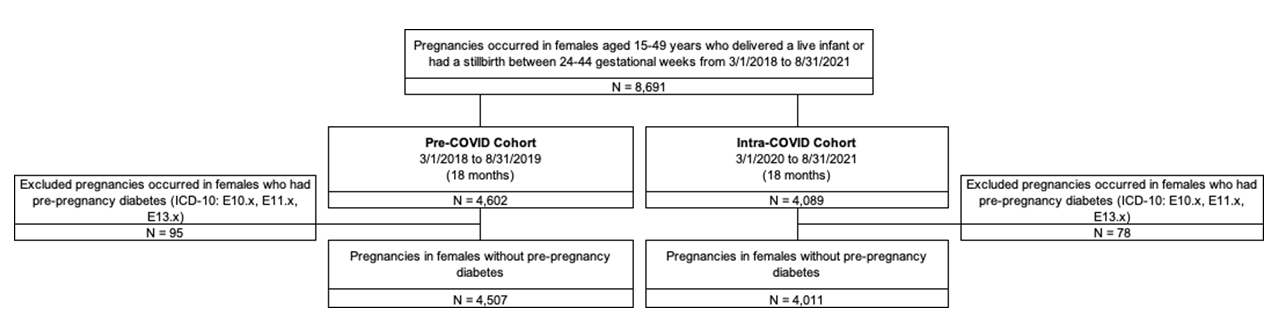
Abbreviations: CI, confidence interval; GDM, gestational diabetes mellitus; ICD-10, International Classification of Diseases, Tenth Revision. Figure 1: Sample Selection Flow Chart.
We compared maternal characteristics and clinical outcomes between the pre-COVID and intra-COVID cohorts using the chi-squared test or t-test. We calculated age- standardized incidences using the age distribution of US females aged 15-49 years in 2018 [25]. We applied multivariable Poisson regressions (log link) with robust standard errors to estimate the risk ratios (RR) and 95% confidence intervals (CI) of GDM for the overall sample and by racial and ethnic groups. A random effect was specified to control the correlation due to multiple pregnancies per individual. Models were adjusted for pre-selected potential confounders: race and ethnicity (the overall sample only), maternal age, nulliparity, marital status, pre-pregnancy BMI, gestational weight gain, and utilization days of prenatal care. We further examined the association of SARS-CoV-2 infection with the risk of GDM. We identified SARS-CoV-2 infections among pregnant individuals using the ICD-code (U07.1).
We performed several sensitivity analyses to examine the robustness of the results. First, we excluded pregnancies with SARS-CoV-2 infections in order to test whether the changes in GDM rates were directly caused by SARS-CoV-2 infection. Second, we excluded pregnancies that were screened for GDM before 3/1/2020 in the intra-COVID cohort, as those pregnancies were not affected by the COVID-19 pandemic before the GDM diagnosis. Lastly, we applied a more restrictive approach to classifying the pre- COVID (pregnancies conceived between 3/1/2018 and 2/28/2019 [12 months]) and intra-COVID (pregnancies conceived between 3/1/2020 and 2/28/2021 [12 months]) cohorts using conception dates, in which all pregnancies in the intra-COVID cohort were affected by the pandemic from the beginning. The conception dates were determined by subtracting the estimated gestational weeks from the delivery dates. We conducted all analyses in R Version 4.0.5. A two-sided p-value < 0.05 was considered statistically significant.
Results
The pre-COVID and intra-COVID cohorts generally had similar maternal characteristics and outcomes, except for marital status, nulliparity, utilization duration of prenatal care, number of prenatal care visits, and gestational weight gain at delivery. There was no difference in the pre-pregnancy BMI, either mean or distribution of pre-pregnancy BMI categories, between the two cohorts. The racial and ethnic compositions of the overall sample (pre-COVID vs. intra- COVID) were: Asian (17.1% vs. 17.1%), non-Hispanic Black (4.7% vs. 4.8%), Hispanic (21.9% vs. 21.9%), non-Hispanic White (42.2% vs. 38.3%), and other or unknown race and ethnicity (14.0% vs. 17.9%) (Table 1).
| Pre-COVID N = 4,507 | Intra-COVID N = 4,011 | P-value | |
|---|---|---|---|
| Maternal age at delivery, years, mean (SD) | 33.8 (5.0) | 34.0 (4.8) | 0.11 |
| Race and ethnicity, N (%) | <0.001* | ||
| Asian | 769 (17.1%) | 687 (17.1%) | |
| Hispanic | 989 (21.9%) | 880 (21.9%) | |
| Non-Hispanic Black | 214 (4.7%) | 191 (4.8%) | |
| Non-Hispanic White | 1904 (42.2%) | 1537 (38.3%) | |
| Other or unknown | 631 (14.0%) | 716 (17.9%) | |
| Married, N (%) | 3568 (79.2%) | 3093 (77.1%) | 0.004* |
| The first pregnancy in the EHR (nulliparity), N (%) | 3132 (69.5%) | 2924 (72.9%) | <0.001* |
| Singleton pregnancy, N (%) | 4316 (95.8%) | 3864 (96.3%) | 0.20 |
| Pre-pregnancy BMI, kg/m2, mean (SD) | 25.4 (5.4) | 25.3 (5.4) | 0.58 |
| Pre-pregnancy BMI category, N (%) | 0.97 | ||
| Underweight (<18.5 kg/m2) | 102 (2.3%) | 93 (2.3%) | |
| Normal weight (18.5-24.9 kg/m2) | 2448 (54.3%) | 2195 (54.7%) | |
| Overweight (25-29.9 kg/m2) | 1166 (25.9%) | 1034 (25.8%) | |
| Obese (≥30 kg/m2) | 760 (16.9%) | 658 (16.4%) | |
| Unknown | 31 (0.7%) | 31 (0.8%) | |
| National area deprivation index, mean (SD) | 16.6 (22.9) | 16.9 (22.9) | 0.57 |
| Smoking during pregnancy, N (%) | 65 (1.4%) | 62 (1.5%) | 0.84 |
| Utilization days of prenatal care, mean (SD) | 176 (79.6) | 186 (73.9) | <0.001* |
| Number of prenatal care visits, N (%) | 12.9 (6.9) | 13.8 (6.4) | <0.001* |
| Gestational weight gain at delivery (pound), mean (SD) | 23.0 (14.4) | 24.1 (14.0) | 0.002* |
| Gestational weeks at delivery, N (%) | 39.0 (2.0) | 39.0 (1.8) | 0.24 |
Table 1: ** Maternal characteristics and outcomes in the pre-and intra-COVID cohorts.
Abbreviations: BMI, body mass index; COVID, coronavirus disease; EHR, electronic health record; GW, gestational week; ICD-10, International Classification of Diseases; SD, standard deviation. Notes:
- Other races and ethnicity included individuals self-reported as other races, multiple races, American Indian, Alaska Native, or Pacific Islander. 2.3% and 3.3% of pregnancies had unknown race/ethnicity in the pre-and intra-COVID periods, respectively.
- 0.7% and 0.8% of pregnancies had missing pre-pregnancy BMI in the pre-and intra-COVID periods, respectively.
- 12.9% and 16.4% of pregnancies had missing national area deprivation index in the pre-and intra-COVID periods, respectively.
- 22.4% and 22.0% of pregnancies had missing gestational weight gain in the pre-and intra-COVID periods, respectively. *P<0.05. Chi-squared and T-tests were applied. Table 1: Maternal characteristics and outcomes in the pre-and intra-COVID cohorts.
In the validation study, the GDM cases identified using the ICD-10 codes were highly accurate (accuracy, 98.3%), with a sensitivity of 97.6%, specificity of 98.3%, positive predictive value of 81.2%, and negative predictive value of 99.8%, when using the plasma glucose values from the GDM screen tests as the “gold standard” among those with laboratory data (N=4,841) (Supplementary Figure 1).
| Pre-COVID (reference) N = 4,507 | Intra-COVID N = 4,011 | Multivariable- adjusted | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Crude | 95% CI | Age-std | 95% CI | Crude | 95% CI | Age-std | 95% CI | RR | 95% CI | |
| Overall | 9.03% | (8.19%, 9.87%) | 8.49% | (7.52%, 9.45%) | 10.57% | (9.62%, 11.52%) | 10.02% | (8.88%, 11.16%) | 1.17* | (1.02, 1.35) |
| By race and ethnicity | ||||||||||
| Asian | 14.56% | (12.07%, 17.06%) | 12.68% | (9.61%, 15.76%) | 14.41% | (11.78%, 17.04%) | 13.66% | (9.98%, 17.33%) | 0.99 | (0.75, 1.30) |
| Hispanic | 11.63% | (9.63%, 13.63%) | 11.53% | (9.28%, 13.78%) | 15% | (12.64%, 17.36%) | 14.68% | (12.01%, 17.36%) | 1.26* | (1.00, 1.59) |
| Non-Hispanic Black | 6.07% | (2.87%, 9.28%) | 5.37% | (2.18%, 8.57%) | 8.38% | (4.45%, 12.31%) | 8.68% | (4.17%, 13.19%) | 1.32 | (0.63, 2.76) |
| Non-Hispanic White | 5.78% | (4.73%, 6.83%) | 4.78% | (3.65%, 5.91%) | 7.48% | (6.17%, 8.80%) | 6.76% | (5.05%, 8.48%) | 1.34* | (1.03, 1.74) |
| Other/ unknown | 9.03% | (6.80%, 11.27%) | 9.44% | (6.55%, 12.33%) | 8.66% | (6.60%, 10.72%) | 8.31% | (5.87%, 10.76%) | 0.99 | (0.69, 1.42) |
Table 2: ** Crude and age-standardized GDM incidences in the pre-and intra-COVID cohorts.
Abbreviations: age-std, age-standardized; BMI, body mass index; EHR, electronic medical record; CI, confidence interval; COVID, coronavirus disease; GDM, gestational diabetes mellitus; RR, risk ratio. Notes:
- Age-standardized incidences were standardized to the age distribution of females 15-49 years in 2018 (US Census Bureau, Current Population Survey, Annual Social and Economic Supplement, 2018).
- Multivariable models adjusted for maternal age, nulliparity, marital status, pre-pregnancy BMI, gestational weight gain, and utilization days of prenatal care. In the overall sample, race and ethnicity was also adjusted.
- Poisson regressions (log link) with robust standard errors and a random effect for each pregnant individual were applied to calculate RR and 95% CI. *P<0.05. Table 2: Crude and age-standardized GDM incidences in the pre-and intra-COVID cohorts.
The age-standardized GDM incidence was 8.49% (95% CI: 7.52%, 9.45%) in the pre-COVID cohort and 10.02% (95% CI: 8.88%, 11.16%) in the intra-COVID cohort. In both cohorts, the age-standardized GDM incidences were highest among Asians (12.68% and 13.66%) and Hispanics (11.53% and 14.68%), followed by non-Hispanic Blacks (5.37% and
8.68%) and non-Hispanic Whites (4.78% and 6.76%). The risk of GDM was 17% higher (RR=1.17; 95% CI: 1.02, 1.35) in the intra-COVID cohort than in the pre-COVID cohort among the overall sample after adjusting for race and ethnicity, maternal age, nulliparity, marital status, pre-pregnancy BMI, gestational weight gain, and utilization of prenatal care. When stratified by racial and ethnic groups, significant increases in GDM incidences were observed in non-Hispanic Whites (RR=1.34; 95% CI: 1.03, 1.74), Hispanics (RR=1.26; 95% CI: 1.00, 1.59), and non-Hispanic Blacks (RR=1.32; 95% CI: 0.63, 2.76; although not significant due to the small sample size), but not in Asians (RR=0.99; 95% CI: 0.75, 1.30) and the other/ unknown group (RR=0.99; 95% CI: 0.69, 1.42) (Table 2).
We further examined the association between SARS- CoV-2 infection and GDM risk. The RR of GDM was 1.18 (95% CI: 0.75, 1.87) when comparing pregnancies infected by SARS- CoV-2 to those not infected by SARS-CoV-2 with a p-value of 0.47. In addition, when comparing the GDM incidence between the pre-COVID and intra-COVID cohorts by excluding pregnancies with SARS-CoV-2 infections (N=153), the results were almost unchanged (RR=1.18; 95% CI: 1.02, 1.35), suggesting that the observed changes in GDM rates between the intra-COVID and pre-COVID cohorts were unlikely due to SARS-CoV-2 infections. (Supplementary Table 1).
In additional sensitivity analyses to examine the influence of possible bias due to the misclassification of exposure, the results remained similar. (Supplementary Table 1). We first excluded a small number of pregnancies (N=560) with GDM screened before 3/1/2020 in the intra- COVID cohort (i.e., these pregnancies might not have been exposed to the pandemic by the time of GDM diagnosis), and the RR was unchanged (RR=1.19; 95% CI: 1.03, 1.37). In addition, when using the more restrictive conception dates to define the pre-COVID (N=2,186) and intra-COVID (N=2,041) cohorts, the RR was even slightly elevated (RR=1.24; 95% CI: 1.01, 1.52). The statistically insignificant results from the race and ethnicity stratified analyses were likely due to the considerable reduction in sample size.
Discussion
We found a 17% increase in GDM incidence during the COVID-19 pandemic in a US cohort, independent of race and ethnicity, maternal age, nulliparity, marital status, pre- pregnancy BMI, gestational weight gain, and utilization of prenatal care. GDM incidence increased among non-Hispanic Whites (34%), Hispanics (26%), and non-Hispanic Blacks (32%), but not among Asians (-1%) and the other/unknown group (-1%). The statistically insignificant result among non- Hispanic Blacks (p-value=0.46) is likely due to their small sample size in our study (i.e., 4.7% in the pre-COVID cohort and 4.8% in the intra-COVID cohort).
The observed increase in GDM incidence in our study is consistent with the findings from a few previous studies that focused on the impact of the lockdown period in China and Italy [19, 20, 21]. Our results also align with a large study using insurance claims in the US, in which the unadjusted GDM risk increased by 12% during the pandemic period (3/1/2020 to 12/31/2020) as compared to the reference period (3/1/2019 to 12/31/2019) [22]. Notably, these studies did not adjust for any confounders. A more recent study in Canada reported that the GDM rate increased by 5% in the early pandemic period (3/1/2020 to 8/22/2020) and 14% in the late pandemic period (8/23/2020 to 3/31/2021) as compared to the pre-pandemic period (8/23/2019-2/29/2020) [23]. Although the Canadian study controlled for maternal age, parity, comorbidity, socioeconomic disadvantage, and place of residence in their analyses, the more critical GDM risk factors, such as pre-pregnancy BMI and gestational weight gain, were not controlled. Nonetheless, the finding in our study with a more extended period during the pandemic is in accordance with findings from different populations and counties, indicating a higher rate of GDM during the COVID-19 pandemic.
To our knowledge, this is the first study to examine the impact of COVID-19 on GDM incidence by race and ethnicity. Our results of increased GDM incidences among certain racial and ethnic groups (i.e., non-Hispanic Whites, Hispanics, and non-Hispanic Blacks) but not others (i.e., Asians), even after adjusting for potential confounders, are novel and intriguing. Asian females had the highest GDM incidence both before and during the pandemic, but their risk seems unaffected by the pandemic.
Another significant finding of our study is that the increased GDM incidence during the COVID-19 pandemic may not be directly caused by SARS-CoV-2 infections, as evidenced by the non-significant association between SARS-CoV-2 infection and GDM incidence in our study and a population-based cohort study in the US [26]. In addition, after excluding the 153 pregnancies infected with SARS- CoV-2, the GDM incidence remained significantly higher in the intra-COVID cohort than in the pre-COVID cohort.
The elevated GDM incidence during the COVID-19 pandemic may be explained by changes in GDM risk factors related to behavioral and psychological factors, including an unhealthy diet, decreased physical activity, reduced sleep duration, and increased depression and anxiety [17, 18]. The pandemic may also disproportionally affect these risk factors in certain racial and ethnic groups. For example, Asians tend to have fewer undesired lifestyle changes, including less increase in smoking or alcohol consumption, than other racial and ethnic groups in the US during the COVID-19 pandemic [16, 27], which may explain why the GDM incidence in Asians did not increase during the pandemic. Unfortunately, we do not have data on lifestyle and psychological factors in our cohort; thus, we cannot explore the above explanations. Future studies are needed to investigate the underlying reasons for the changes in GDM rates, overall and by racial and ethnic groups.
It is worth mentioning that the GDM incidence in our study was higher than the national rates (5-6%), which were based on data obtained from birth certificates [3]. However, birth certificates are known for their underestimation of the GDM rates [28]. Another possible reason is that our cohort included higher proportions of Asians and Hispanics than the national averages. It is well-documented [2], and also shown in our study, that Asians and Hispanics had higher GDM incidence than other racial and ethnic groups.
This study has several unique strengths. First, this study included a large number of racially and ethnically diverse pregnant individuals, which not only provides an adequate sample size for the stratified analyses by race and ethnicity, but also enhances the generalizability of the study findings. Second, the study cohorts underwent the same universal GDM screening test before and during the pandemic, which enabled a valid comparison of GDM incidences pre- vs. intra-COVID pandemic. Third, we extracted rich data regarding sociodemographic and clinical characteristics and carefully controlled for potential confounders, including pre-pregnancy BMI and gestational weight gain. Third, we conducted a validation analysis and found that there is very little possibility of misclassification of outcomes. GDM was accurately identified using ICD-10 codes with an accuracy of 98.3%. Lastly, we conducted sensitivity analyses using different methods to define the pre- and intra-pandemic cohorts in order to assess the potential influence of misclassification of exposure. The robustness results from these sensitivity analyses indicated that the possibility of exposure misclassification was unlikely to occur.
A few potential limitations need to be considered. First, our study is observational by design, so residual confounding cannot be ruled out. In addition, as our cohort was from a large city in the US, the findings from our study may not be generalized to rural populations. Nevertheless, the increase in GDM rate estimated from our study is of a similar magnitude to that found in several other studies conducted in different populations and countries.
Conclusion
Compared to the pre-pandemic period, we found an increase in GDM incidence during the COVID-19 pandemic, especially among non-Hispanic Whites, Hispanics, and likely non-Hispanic Blacks in a racially and ethnically diverse cohort from a US metropolitan city. Future studies in other populations are warranted to confirm our findings, particularly by racial and ethnic groups. Further investigations are needed to explore specific reasons for the pandemic-related GDM risk increases in particular racial and ethnic groups and to develop possible mitigation strategies.
References
-
McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, et al. (2019) Gestational diabetes mellitus. Nat Rev Dis Primers 5(1): 47.
-
Chen L, Mayo R, Chatry A, Hu G (2016) Gestational diabetes mellitus: its epidemiology and implication beyond pregnancy. Current Epidemiology Reports 3(1): 1-11.
-
Shah NS, Wang MC, Freaney PM, Perak AM, Carnethon MR, et al. (2021) Trends in gestational diabetes at first live birth by race and ethnicity in the US, 2011-2019. JAMA 326(7): 660-669.
-
Bardenheier BH, Imperatore G, Gilboa SM, Geiss LS, Saydah SH, et al. (2015) Trends in gestational diabetes among hospital deliveries in 19 US States, 2000-2010. Am J Prev Med 49(1): 12-19.
-
DeSisto CL, Kim SY, Sharma AJ (2014) Peer reviewed: Prevalence estimates of gestational diabetes mellitus in the United States, pregnancy risk assessment monitoring system (prams), 2007-2010. Prev Chronic Dis 11: E104.
-
Lavery J, Friedman A, Keyes K, Wright J, Ananth C (2017) Gestational diabetes in the United States: temporal changes in prevalence rates between 1979 and 2010. BJOG 124(5): 804-813.
-
Baraban E, McCoy L, Simon P (2008) Increasing Prevalence of Gestational Diabetes and Pregnancy- Related Hypertension in Los Angeles County, California, 1991-2003. Prev Chronic Dis 5(3): A77.
-
Wang H, Li N, Chivese T, Werfalli M, Sun H, et al. (2022) IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diabetes Res Clin Pract 183: 109050.
-
Carr DB, Newton KM, Utzschneider KM, Faulenbach MV, Kahn SE, et al. (2011) Gestational diabetes or lesser degrees of glucose intolerance and risk of preeclampsia. Hypertens Pregnancy 30(2): 153-163.
-
Bellamy L, Casas JP, Hingorani AD, Williams D (2009) Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. The Lancet 373(9677): 1773-1779.
-
Kramer CK, Campbell S, Retnakaran R (2019) Gestational diabetes and the risk of cardiovascular disease in women: a systematic review and meta-analysis. Diabetologia 62(6): 905-914.
-
HAPO Study Cooperative Research Group (2002) The hyperglycemia and adverse pregnancy outcome (HAPO) study. Int J Gynecol Obstet 78(1): 69-77.
-
Boney CM, Verma A, Tucker R, Vohr BR (2005) Metabolic syndrome in childhood: association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 115(3): e290-e296.
-
Rowland J, Wilson CA (2021) The association between gestational diabetes and ASD and ADHD: a systematic review and meta-analysis. Sci Rep 11(1): 5136.
-
Javaid S, Barringer S, Compton SD, Kaselitz E, Muzik M, et al. (2021) The impact of COVID-19 on prenatal care in the United States: Qualitative analysis from a survey of 2519 pregnant women. Midwifery 98: 102991.
-
Chen L, Li J, Xia T, Matthews TA, Tseng TS, et al. (2021) Changes of Exercise, Screen Time, Fast Food Consumption, Alcohol, and Cigarette Smoking during the COVID-19 Pandemic among Adults in the United States. Nutrients 13(10): 3359.
-
Whitaker KM, Hung P, Alberg AJ, Hair NL, Liu J (2021) Variations in health behaviors among pregnant women during the COVID-19 pandemic. Midwifery 95: 102929.
-
Tomfohr Madsen LM, Racine N, Giesbrecht GF, Lebel C, Madigan S (2021) Depression and anxiety in pregnancy during COVID-19: A rapid review and meta-analysis. Psychiatry Res 300: 113912.
-
He Z, Lv Y, Zheng S, Pu Y, Lin Q, et al. (2022) Association of COVID-19 Lockdown With Gestational Diabetes Mellitus. Front Endocrinol 13: 824245.
-
Zanardo V, Tortora D, Sandri A, Severino L, Mesirca P, et al. (2022) COVID-19 pandemic: Impact on gestational diabetes mellitus prevalence. Diabetes Res Clin Pract 183: 109149.
-
La Verde M, Torella M, Riemma G, Narciso G, Iavarone I, et al. (2022) Incidence of gestational diabetes mellitus before and after the Covid‐19 lockdown: A retrospective cohort study. J Obstet Gynaecol Res 48(5): 1126-1131.
-
Sun S, Savitz DA, Wellenius GA (2021) Changes in adverse pregnancy outcomes associated with the COVID-19 pandemic in the United States. JAMA Network Open 4(10): e2129560.
-
Auger N, Wei SQ, Dayan N, Ukah UV, Quach C, et al. (2022) Impact of Covid-19 on rates of gestational diabetes in a North American pandemic epicentre. Acta Diabetologica, pp: 1-8.
-
Mackey K, Ayers CK, Kondo KK, Saha S, Advani SM, et al. (2021) Racial and ethnic disparities in COVID-19–related infections, hospitalizations, and deaths: a systematic review. Ann Intern Med 174(3): 362-373.
-
US Census Bureau (2018) Current Population Survey, Annual Social and Economic Supplement.
-
Ferrara A, Hedderson MM, Zhu Y, Avalos LA, Kuzniewicz MW, et al. (2022) Perinatal Complications in Individuals in California With or Without SARS-CoV-2 Infection During Pregnancy. JAMA Internal Medicine 182(5): 503- 512.
-
Avalos LA, Nance N, Zhu Y, Croen LA, Young Wolff KC, et al. (2022) Contributions of COVID-19 pandemic-related stressors to racial and ethnic disparities in mental health during pregnancy. Front Psychiatry 13: 837659.
-
Devlin HM, Desai J, Walaszek A (2009) Reviewing performance of birth certificate and hospital discharge data to identify births complicated by maternal diabetes. Matern Child Health J 13(5): 660-666.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria