Factors Affecting Utilization of Contraceptives among Women Aged 15-24 Years Attending Fort Portal Regional Referral Hospital, Fort Portal City, Uganda
Background: Fertility regulation and pregnancy prevention among young women is one of the most important health care issues of the twenty-first century. This is because more than 16 million adolescent girls give birth every year worldwide and an additional 5 million have abortions and Sub Saharan Africa accounts for 50% of these births. As a result, the need for specially tailored child spacing programs for young women has come to the fore of reproductive health services. Methods: Hospital-based cross-sectional study was conducted among women aged 15-24 years attending FRRH prevention from January to March 2021. Data were collected using structured researcher administered questionnaires. Descriptive analysis was used to present frequency and percentage of the main findings. The association between independent variables and determinants of contraceptive use was calculated using Pearson’s Chi square and p-values less than 0.05 were considered as statistically significant. Results: A total of 418 young women aged 15-24 years participated in the study with a 100% response rate. Majority 76.6% were in age category 20-24 years, had attained secondary education 82.5%, were married 62.4%), had a single child 66.3%. Majority of the women felt that their income was not enough 84.2% even though 41.4% were employed. The prevalence of contraceptive use was 95.2%. Age of the women and the contraceptive of choice p=0.001, level of education and contraceptive methods p=0.001, marital status and contraceptive methods p=0.001, discussion with partner and contraceptive uptake p = 0.001, partner’s approval to family planning p = 0.001 and finally contraceptive method with religion p=0.001 were all significant factors of contraceptive use and when all confounders were controlled in a logistic regression model, the factors that remained significant were: The age of women, Level of education, Employment status, discussion with husband/partner on number of children to have and need to have another child. Conclusion: The prevalence of contraceptive use among women aged 15-24 years attending FRRH is higher than the national prevalence and surpasses the national set targets. This is significantly determined by age of the woman, level of education, income levels through employment and opinion of their partners
Operational Definitions
- Contraception: Methods or devices used to prevent pregnancy.
- Contraceptives: Device, drug or chemical agent that prevents conception.
- Reproductive health: Reproductive health is a state of complete physical, mental, and social well- being and not merely the absence of disease or infirmity, in all matters relating to the reproductive system and to its functions and processes.
- Sexual reproductive health: Sexual health means having a responsible, satisfying, and safe sex life and not merely having sex for reproduction.
- Sexual Activity: Having ever engaged in sexual intercourse.
- Contraceptive utilization: Ever use of modern contraceptive (both current and past)
Introduction
Background of the Study
Fertility regulation and pregnancy prevention among young women is one of the most important health care issues of the twenty-first century. This is because more than 16 million adolescent girls give birth every year worldwide and an additional 5 million have abortions [1]. Sub Saharan Africa accounts for 50% of these births. As a result, the need for specially tailored adolescent’s sexual health services has become more pressing. Currently there are conflicting messages about gender sexuality; the promotion of sexual involvement on one extreme and urging of chastity on the other makes the young women feel guilty, uncertain or indecisive about contraception [2].
Globally, studies on young women sexual behavior show their premarital sexual encounters are generally unplanned, infrequent and sporadic. This pattern predisposes them to unplanned pregnancy [3]. Unplanned young women pregnancy is associated with unsafe abortion a cause of 13% of global maternal mortality. It’s more dangerous for adolescents as they tend to seek abortion later in pregnancy. Meeting the contraceptive needs of these young women could prevent this problem [4]. In Africa, young women account for over 23% of the total population [5]. Sub- Saharan Africa has the greatest proportion of young women who have begun child bearing [6]. In many parts of Sub-Saharan Africa, adolescent’s sexual and reproductive health (SRH) remains a highly charged moral and religious issue [7]. Studies have shown that while most pregnancies among young women in sub-Saharan Africa are unplanned, the use of contraceptives remains low [8].
Despite the global progress in increasing availability and coverage of family planning services, most of the contraceptive needs of young women are largely unmet [9]. Uganda’s fertility rates of young women are among the highest in the world. According to the latest Uganda Demographic and Health Survey (DHS), 24.8% of girls aged 15–19 had already begun childbearing. Furthermore, Uganda has one of the lowest contraceptive prevalence rates in the region. The high numbers of adolescents giving birth at an early age partly contributes to Uganda’s high fertility levels [9].
This study aimed at describing factors affecting utilization of contraceptives among young women aged 15 – 24 years attending Fort portal Regional Referral Hospital (FRRH). Its recommendations will help in improving implementation of programs focusing on the reproductive health needs of young women in that particular age group in areas serviced by FRRH and Uganda, which with better health; this will increase their contribution to the development of the country.
Problem Statement
Worldwide there is an estimated 14.3 million births to young women; 2.5 million adolescent girls worldwide have an unsafe abortion annually [10]. Globally, young women face a high unmet need for contraception further predisposing them to unplanned pregnancy and risk of unsafe abortion [3]. According to the latest Uganda Demographic and Health Survey (DHS), 26.2% of girls aged 15–25 had already begun childbearing. Furthermore, Uganda has one of the lowest contraceptive prevalence rates in the region. From Uganda Demographic Health Survey (UDHS) of 2016 ,one out of four (25%) of all girls, according to the findings aged 15-25 years have either a child or are pregnant, representing a 1% increase in teenage pregnancy rates over the previous 2011 survey [11]. Uganda’s fertility rate stands at 5.9 children per woman, above the Sub-Saharan average of 4.8 [12]. This high fertility rate is attributed to low use of contraceptives, however, high levels of child marriages and early child bearing also play an important role, which remains a public health concern that should be averted. Assessing the levels of contraceptive awareness and use helps to identify potential areas of intervention or barriers hindering utilization of the contraceptive among reproductive aged women. Exploring fertility preferences in relation to contraceptive use can increase the understanding of future reproductive behavior and unmet family planning needs. This knowledge can help assist women in meeting their reproductive goals in the study area. Hence this study sought to explore the factors affecting utilization of contraceptives among women aged 15-24 years attending Fort Portal Regional Referral Hospital. Objectives Broad Objective: To assess the factors affecting utilization of contraceptives among women aged 15-24 years attending Fort Portal Regional Referral Hospital, Fort Portal City, Uganda.
Specific Objectives: To determine the prevalence of contraceptive use among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City.
- To determine socio demographic, cultural and economic factors that influence the contraceptive methods option among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City.
- To determine association between the contraceptive options and family planning needs among women aged 15-24 attending Fort Portal Regional Referral Hospital in Fort Portal City.
Research Questions
- What is the prevalence of contraceptive use among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City?
- What are the socio demographic, cultural and economic factors that influence the contraceptive methods option among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City?
- Is there any association between the contraceptives options and family planning needs among women aged 15-24 seeking attending Fort Portal Regional Referral Hospital in Fort Portal City?
Justification
Uganda is one of the countries with low utilization of contraceptives among the young women categories especially in the rural areas where medical resources are limited, and risk factors associated with contraceptives related effects among youth goes unnoticed due to both economic and cultural reasons. Use of contraceptives will be beneficial to the community in that it will help to bring out the information about the accessibility and availability of contraceptives early and, Therefore, enable them to access the contraceptives. This study will also help to identify factors contributing to the utilization of contraceptives among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City, and come up with recommendations that may help in designing interventions and strategies to help the adolescents to access essential health intervention measures. The study will also help to generate useful data that could provide a base for further research to be carried out in this field.
Significance of the Study
Most studies on adolescents are on sexual activity among this sub population and the consequences of their risky sexual behavior. However, little research has been done among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City on this particular proposed subject of study. The study therefore, adds to the knowledge on the level of contraceptive uptake and factors influencing contraception among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City hence closing the conceptual gaps in young women’s utilization of contraceptives. The study through its findings contributes to future review and revision of policies and practices regarding reproductive health, sexuality and family life. This study will serve as a basis for future research on adolescents’ contraception. This study also helps the principal investigator to partially fulfill the requirements for the award of bachelor’s degree of medicine and surgery of Kampala International University.
Study Scope
- Geographical scope: The study was carried out among women aged 15 – 24 years attending FRRH. Fort Portal Regional Referral Hospital is located within the city of Fort Portal, approximately 294 kilometres (183 mi) from Kampala, Uganda’s capital and largest city. The coordinates of the hospital are: 0°39’19.0”N, 30°16’53.0”E (Latitude: 0.655278; Longitude: 30.281389).
- Content scope: This study limited itself within the boundaries of factors affecting utilization of contraceptives among women aged 15-24 years attending Fort Portal Regional Referral Hospital in Fort Portal City.
- Time scope: Data collection of the study was conducted from January 2021 to March 2021.
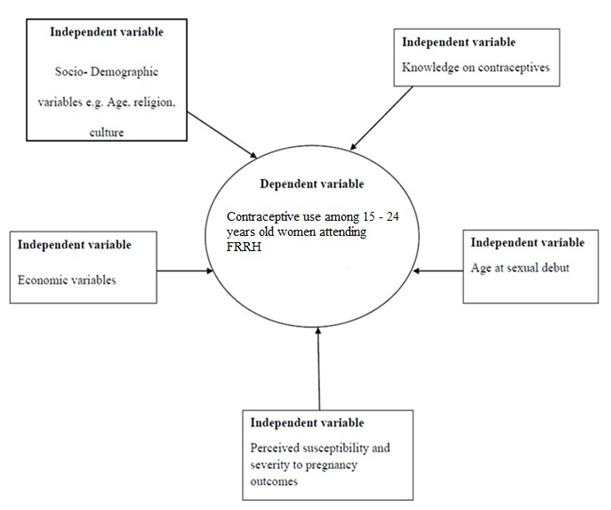
Conceptual Framework
The conceptual framework is based on the theory of reasoned action and literature review. The theory of reasoned action postulates that behavior is influenced by several factors among them, ones belief about the outcome of an action, one’s assessment that a particular behavior is desired by significant others and a motivation to comply with the views of the significant others [13]. In the social environment there are several factors that would be considered as significant others for example, peers, parents, religion, culture, knowledge/available information and economic factors.
According to this theory, adolescents and young women would have to believe that use of contraceptives would prevent unwanted pregnancies and sexually transmitted infections and that the significant others would not want them to get unplanned pregnancies and sexually transmitted infections. Complying with the significant others would mean that adolescents would take action or not take action. Taking the action to prevent pregnancy would influence adolescent’s utilization of a contraceptive method.
With this theory in mind, literature review revealed that contraceptive utilization among adolescents is influenced by socio-demographic variables such as age at sexual debut, economic variables, knowledge on contraceptives, perceived susceptibility to pregnancy and perceived severity of pregnancy outcomes among the adolescents as independent variables which will either promote or hinder contraceptive utilization. Conceptual framework adopted from the [13] and Literature.
Literature Review
Introduction
Contraception is defined as the use of a contraceptive method to prevent pregnancy by interfering with ovulation, fertilization, and/or implantation [14]. Contraceptives help women plan when and how many children to have. Contraceptive methods are classified as hormonal or non- hormonal methods. They include condoms, pills, sterilization, injections, and intra-uterine devices, spermicidal and implant [15].
The main contraceptive options for young women are condoms backed up by hormonal contraception however; hormonal contraceptives should be used in a longer, mutually monogamous relationship. With the exception of male and female sterilization, all methods that are physiologically safe for adults are also physiologically safe for adolescents [16].
Addressing the Sexual and Reproductive Health challenges faced by adolescents in Sub Saharan Africa is critical given the large contribution adolescent childbearing makes to the high levels of fertility observed in many Sub- Saharan African countries. Improved Sexual and Reproductive Health among adolescents is likely to raise women’s status and reduce poverty among families [17].
Global Overview of Family Planning Use and Options
In Latin America and the Caribbean, more than one half of pregnancies are unintended, even though about 65% of married women of reproductive age use modern contraceptives. Almost two- thirds of pregnancies in Caribbean (62%) and South America (63%) are unintended, as are 43% of pregnancies in Central America (including Mexico). Modern family planning services include counseling, provision of contraceptives and follow up [18]. Substantial evidence is found in existing literature that broadening the choice of family planning methods increases overall family planning prevalence. The provision of a wide range of contraceptive methods increases the opportunity for individual couples to obtain a method that suits their needs. Contraceptive choice is also a central element of quality of care in the provision of family planning services and an important dimension of women’s reproductive rights. To increase prevalence of use, family planning programs should offer a variety of safe, effective, acceptable and affordable contraceptive methods to help women prevent unwanted pregnancies and sexually transmitted diseases (STDs) and to help them achieve their childbearing goals [19].
Young people have a real need for reproductive health and family planning information and services. The age at which young people have their first sexual experience is falling, while the number of unmarried sexually active young people is growing significantly [11]. Although many adolescent claim to know about contraception and safe sex, their actual knowledge is often quite poor. Many young people believe that you can’t get pregnant the first time you have sex, for example, or that you can’t get pregnant if you have sex standing up. As a result of incomplete knowledge about family planning, adolescents are vulnerable to sexually transmitted infections and unwanted pregnancy [20].
A conservative estimate of the total number of abortions among adolescents in developing countries ranges from 2.2 to 4 million annually. Research shows that unmet need for contraceptive among sexually active adolescents, those who express a desire to prevent pregnancy but aren’t using any contraception, is high in many regions [7]. Many societies disapprove of premarital sex and consider reproductive health care for young people in appropriate. As a result parents, educators and health care providers often are unwilling to give young people the information and services they need. Laws and policies restrict adolescent’s access to services, for example by limiting family planning services to married adolescents [21] or by including conditions such as parental or spousal approval. In addition to ignorance about sexual and reproductive health and harmful sexual behaviours that carry on into adulthood, negative attitudes to young people’s sexuality lead to stigma against young people who use or ask for contraceptive, reinforcement of local cultural and faith based restriction on access to services, service provider’s reluctance to provide contraceptives to young people, difficulties for young people in insisting on condom use with their partners and in accessing contraceptives, unwanted pregnancies among adolescents and young people and increased rates of sexually transmitted infections, including HIV [22]. Family Planning Use and Options in Sub-Saharan Africa Sub-Saharan Africa has the highest fertility rates of any world region, 5.4 births per woman on average-double that of Asia (excluding China) and more than three times that of Europe. One of the factors underlying high maternal mortality rate is the low use of modern contraception. Only 18% of married women in Sub-Saharan Africa use modern methods of family planning. An estimated 35 million women in Sub-Saharan Africa have unmet need for family planning. They want to delay or stop childbearing but are not using any method [10].
The relatively high birth rate in Nigeria which has been accompanied by stead declines in death rates has resulted in high rates of population growth. Nigeria’s annual rate of population growth of about 2.87 % has been a major concern for population experts and policy makers for some time. With an estimated doubling period of less than 25 years at the current rate of population growth, the current level of consumption can only be maintained if production of goods and services will also double in less than 25 years. Unfortunately, this is almost impossible to achieve as all available literature indicates that the rate of growth of the economy has been lower than the rate of growth of the population. Standards of living tend to worsen when the rate of population growth exceeds the rate of economic growth. Within the last four decades, there has been increased pressure towards family limitation in Nigeria [23]. These are the results of the rapid growth of the large towns, the very great extension of educational facilities, and among the elite, the far greater difficulty of securing top jobs that have come with independence. In response to this situation, a national policy on population for development, unity, progress and self-reliance was formulated in 1998 and revised in 2014. The major goal of the policy is a reduction in fertility through increased adoption of contraception [24].
South Africa’s demographic transition is considerably more advanced than those of other Sub- Saharan African nations; its total fertility rate (TFR) has declined from approximately 6.0 births per woman in 1980 to 2.2 in 2017 [19]. Over the same period, contraceptive use among the four major population groups (black, white, colored and Asians) has increased [18]. Yet the overall modern contraceptives prevalence of 61% (urban 66%, rural 53%) masks wide racial disparities and injectable represent 30% of all use. Contraceptive method of choice is a fundamental indicator of quality of care in a family planning program. The more contraceptive methods that are available, the more likely it is that a program can meet the range of contraceptive needs of a diverse client population 25].
Family Planning Use and Options in Uganda
In Uganda the trend of family planning use among married women in the reproductive age between 15-24 years has gradually been increasing from 7% in 1978 to 46% in 2018 [26]. This has resulted to decline in fertility rate over the years from 8.1 births per woman in 1977/8 to 4.7 in 2008, 4.9 in 2013 and 4.6 in 2016 [11]. However, this fertility rate (approximately five children per woman) is still high in a developing country. The contraceptive methods available in Uganda include male or female sterilization, oral pills, intrauterine device, injections, implant, male and female condom, the traditional methods include withdrawal and rhythm/natural method [27].
Despite the increased use of contraceptive methods, as more Ugandan young women enter reproductive age, unmet need continues to grow. Limited donor resources and a skewed method mix toward short-term (and more costly) methods compound this unmet need. Modern contraceptive use increases dramatically with woman’s education. More than half of married women with at least some secondary education use modern methods, compared with only 8% of women with no education [28].
Factors Contributing to Unmet Family Planning Need
Unmet family planning need refers to Women who are not practicing contraception, but do not want any more births (limiting) or want to postpone the next birth at least two years (spacing) [14]. In East Africa young women have an unmet need for family planning and, without access to modern contraception; they face the risk of an unintended pregnancy. In Tanzania, 22 %of young married women ages 15-24 have an unmet need, as do 40 % of sexually active, unmarried women in this age group. In Rwanda 35% of young married and 55% of sexually active, unmarried women report an unmet need. Data is very scanty on young women in Uganda [29]. Understanding the factors that contribute to unmet family planning need is critical to the efforts of programmes to meet the demand for contraception. Much unmet need for family planning persists, even in settings where knowledge of family planning methods is high. Household wealth: In Tanzania, household wealth is related to unmet need: 23% of young poor women report having an unmet need, while 16% of young wealthy women do. However, household has little effect in Rwanda; 33% of both poor and wealthy young women indicate that they have an unmet need for family planning. Women with unmet need also have low status and weak bargaining power within the household [30].
Misconceptions and concern about health related risks: Studies suggest that many potential users choose not to use more reliable methods due to misperceptions and concern about health-related risks. For example a study in Maldives found that knowledge of family planning was universal, but only 30% of couples were using a contraceptive. Several studies, including one from Malaysia, found that non-use of contraceptive was linked to fears about side effects [31]. Female education: Female education has been seen as a key determinant of contraceptive use [32]. Better-educated women are argued to be more willing to engage in innovative behavior than are less educated women and in many Third World context, the use of contraception remains innovative [33]. Better educated women are also argued to have more knowledge of contraceptive methods or of how to acquire them than are less educated women because of their literacy, greater familiarity with modern institutions and greater likelihood of rejecting a fatalistic attitude towards life. Ontiri S, et al. [34] finds a positive association between the educational level of both spouses and the use of contraceptive methods. Gender of couple’s living children: The study by Ontiri S, et al. [34] also shows that, to a greater extent, contraceptive use and choice of modern method depend on the sex of couple’s living children, implying some preference for sons although generally women prefer to have children of both sexes. In a review study by Gunawardena N, et al. [35], among married women, it was found that the number of living sons a woman has influence her contraceptive use. Spousal communication on family planning: Female autonomy and seclusion, equality between spouses linked with spousal communication, influence contraceptive use [36]. Joshi AK, et al. [37] found in a study in Nepal that spousal communication on family planning was a significant predictor of contraceptive use in the study area. Sometimes women think that their husbands oppose contraceptive use when infact they approve. Thus lack of communication about family planning between partners also contribute to unmet needs [38]. Source of Contraceptives: In a comparison of 15 countries, it’s highlighted that within a year of starting a method, 7-27 of women ceased to practice contraception for reasons related to quality of the service environment [39]. The provision of a range of contraceptive methods at family planning services has also been shown to influence contraceptive option. In a U.S. study, rapid population growth, high rates of unemployment, elevated levels of religious affiliation, higher socioeconomic status and ready access to family planning services were all associated with increased uptake of contraceptives [33]. Similarly, a study in Philippines found that the presence of family planning services and community labor-market conditions and infrastructure development were strong influences on contraceptive use. Other studies have examined other community characteristics including the influence of levels of community economic development, levels of school participation, economic roles of children and community fertility norms on contraceptive [40]. There are currently over one billion people between the ages of 15 and 24, by far the largest childbearing cohort in history [18].
Sexual activity among youth places them at risk of unintended pregnancy and STIs, including HIV/AIDS. Meeting the reproductive health needs of this underserved population is therefore an essential matter for global and domestic discussion since addressing the unmet contraceptive needs will dramatically impact on their health and on future world population. This study therefore will provide a proper understanding of factors influencing realization of contraceptive needs of this age group.
Factors Influencing the Family Planning Option
Individual contraceptive use is influenced by factors at the individual, household, and community level, but the geographic distribution of contraceptive use is often associated with contextual variables, particularly at the community level [32]. These contextual variables typically include social, economic, and cultural influences at the community level [41]. Increased use of contraception is linked to rapid population growth rates, high levels of unemployment, religious affiliation, higher socioeconomic status and greater availability of contraceptive services [42]. A study in Nigeria found that provision of family planning outreach services and the average community wage for women were significant community-level predictors of the use of contraceptive services [23]. Research in South Africa has also shown significant relationships between the wealth status, level of female autonomy, level of female education of communities, and the choice of contraceptive method [43]. Other studies have examined the relationship between spatial patterns of use of contraceptive methods and the influence of community-level factors. In Bangladesh and India, districts located on the border and which share a common language were positive outliers for contraceptive use [35].
Methodology
Introduction
This chapter covers the research design and methodology, including sampling method, study population, data collection, data analysis and ethical considerations.
Study Design
This was a cross-sectional study that was conducted at Fortportal Regional Referral Hospital, in Fortportal city involving young women aged 15-24 years attending FRRH.
A cross-sectional study research design was used because the method enables data collection from a relatively large number of different categories of respondents at a particular time with the exposure and outcome being measured at the same time and there is no need to follow up with the study participants. Cross sectional studies can be generalized because they are representative of given populations; they are the best suited in determining the prevalence and in identifying associations [13].
Study Setting
Fortportal Regional Referral Hospital, commonly known as Fort Portal Hospital, sometimes referred to as Buhinga Hospital, is a hospital in the town of Fort Portal, in Kabarole District, Western Uganda. It is the referral hospital for the districts of Bundibugyo, Kabarole, Kamwenge, Kasese, Ntoroko and Kyenjojo. Fort Portal Hospital lies within the city of Fort Portal, this location is approximately 294 kilometres (183 mi), from Kampala, Uganda’s capital and largest city. The coordinates of the hospital are: 0°39’19.0”N, 30°16’53.0”E (Latitude: 0.655278; Longitude: 30.281389). The bed capacity of Fort Portal Hospital is quoted as 333 and is a government institution.
Study population
The target population was all young women aged 15-24 years attending FRRH. These included the hospital staff and students on clinical practice.
- Inclusion criteria: All young women aged 15-24 years attending FRRH who consented to take part in the study.
- Exclusion criteria: Young women aged 15-24 years attending FRRH but were seriously ill and unable to take part in the study on their own.
Sample size determination and procedures
The sampling frame for participants constituted women aged 15-24 attending FRRH. Participants were selected using systematic random sampling. The study population (N) was estimated at 1000 clients in selected clinics while the sample population (n) was 384 respondents. The sampling interval therefore, was 1000/384 = 2.604 ≈ 3 that is every third client attending FRRH who met the inclusion criteria was selected as a participant. Focused group discussion participant were conveniently selected from study population. They consisted of postnatal women who met the inclusion criterion and had not been interviewed.
Sample size determination: Sample was determined using formula by Gunawardena N, et al. [35]. n=Z2 qp/e2 Where n= desired sample size; Z= standard deviate at 95 %
level of confidence; p= proportion of sexually active women currently using any family planning method (51.3%) [11]. q=1-p e= acceptable error margin Therefore, the minimum sample size was calculated as follows n=1.962 x 0.49 x 0.51/(0.05)2 = 384 This sample size was adjusted for spoilt and incomplete questionnaires and therefore the final sample size used was 418.
Data Collection Instruments and Techniques
The study utilized semi-structured questionnaires and Focused Group Discussions (FDGs) as prime methods of data collection. This is because both methods complement one another in terms of generating ideas and understanding respondent’s views, perceptions, experiences, values, beliefs and expectations about a phenomenon [44]. A semi- structured questionnaire was used to collect quantitative data (See Appendix II). The questionnaires were administered to each study subject by the researcher. Focus Group Discussion (FDG) guides were used to collect qualitative data.
Data Processing and Analysis
Qualitative data collected during the FGDs was transcribed verbatim into Microsoft Word and thematic content analysis done. Quantitative data from the questionnaires was checked daily for completeness and coded for appropriate computer entry. Questionnaire tools were checked for their accuracy and data completeness, and then data was coded and entered into Epi info version 7, then exported into SPSS version 22.0 for analysis. Descriptive statistics was used to summarize the variables. In univariate analysis, frequency distributions showed the distribution of the study population by background characteristics. In bivariate analysis, Chi- square and fisher’s exact test were used.
Quality Control
The questionnaire was pretested amongst willing young women aged 15 – 24 years attending Kampala International University – Teaching Hospital (KIU-TH) prior to the actual data collection. The collected data was checked immediately after finalizing the questionnaire for completeness and consistency of information collected.
Ethical Considerations
Ethical clearance was obtained from Faculty of clinical medicine and dentistry of Kampala International University. Permission to conduct the study and collect data was also sought from Fortportal Regional Referral Hospital administration. Privacy of the young women was maintained throughout the study and the participants’ confidentiality was highly considered.
Results
Introduction
This chapter deals with the analysis of the findings and presents them as per objective and in the form of narratives, tables, graphs and charts. A total of 418 young women aged 15 – 24 years attending FRRH took part in the study. 418 questionnaires were administered, returned and analyzed thereby giving a response rate of 100%.
Socio-Demographic Characteristics of Women Aged 15–24 Years Attending FRRH
A total of 418 young women aged 15 – 24 years attending FRRH participated in the study with a 100% response rate. Majority were in age category 20-24 years were 320 (76.6%) and the rest 98(23.4%) were 15-19 years. Majority of the respondent 82.5% had attained secondary education and below while, 17.5% of the respondents had attained beyond secondary school level of education. A higher proportion of the respondents were married 261(62.4%), not married had a representation of 138(33%), while divorced and separated were 19(4.5%). Respondents with a single child were 66.3% while those with two constituted of 31.6%. Only 2.2% had three children in Table 1 and Figure 2.
| Characteristic | Category | Frequency (N=418) | Percentage (%) |
|---|---|---|---|
| Age | 15 - 19years | 98 | 23.4 |
| 20 - 24years | 320 | 76.6 | |
| Level of education | Below Secondary | 345 | 82.5 |
| Above Secondary | 73 | 17.5 | |
| Marital Status | Married | 261 | 62.3 |
| Not Married | 138 | 33 | |
| Separated/divorced | 19 | 4.5 | |
| Number of children | 1 child | 277 | 66.3 |
| 2 Children | 132 | 31.5 | |
| 3 Children | 9 | 2.2 |
Table 1: Distribution of sociodemographic characteristics of women aged 15 – 24 years attending FRRH.
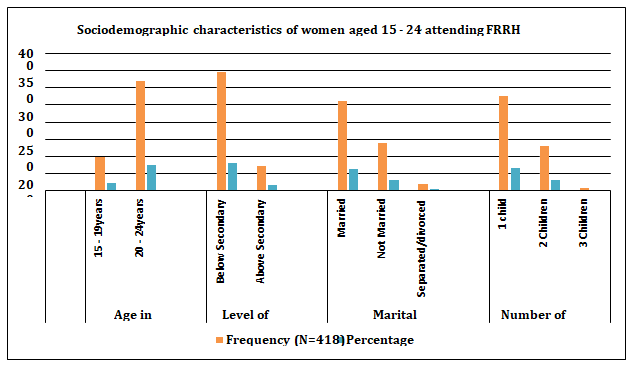
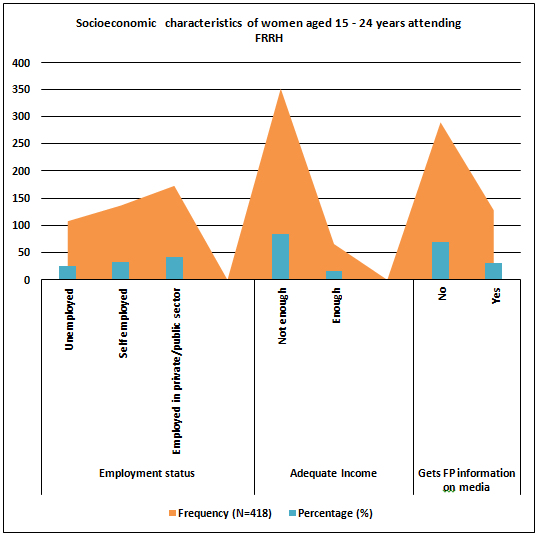
Figure 2: Column graph showing distribution of sociodemographic characteristics of women aged 15 – 24 years attending FRRH By socioeconomic stratification, the women at FRRH in the study who were employed in the private or public sector were 41.4% while 32.8% were self-employed. Majority of the women felt that their income was not enough with a representation of 84.2%, those who were comfortable with their income had a representation of 15.8%. The proportion of the women who got family planning information from the media was 30.6% while those who do not get were 69.4% as shown in Table 2 and Figure 3.
| Characteristic | Category | Frequency (N=418) | Percentage (%) |
|---|---|---|---|
| Employment status | Unemployed | 108 | 25.8 |
| Self employed | 137 | 32.8 | |
| Employed in private/public sector | 173 | 41.4 | |
| Adequate Income | Not enough | 352 | 84.2 |
| Enough | 66 | 15.8 | |
| Gets FP information on media | No | 290 | 69.4 |
| Yes | 128 | 30.6 |
Table 2: Socio-economic stratification of women aged 15 – 24 years attending FRRH.
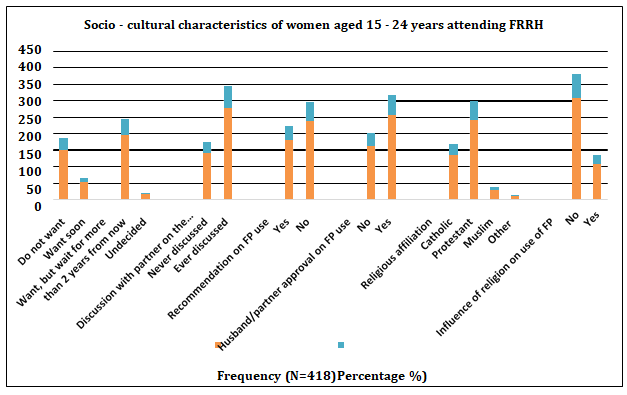
By socio-cultural characterization, majority of the women would want to have another child after a 2 year wait 47.1%, had ever discussed contraception with their partners 66.3%, 56.9% would not recommend FP while 61.2% had approval from their partners to use FP 61.2%. A combined 90.2% of the women were Catholics and protestants by religion however the majority 73.9% believed religion had no influence on FP use as shown in Table 3 and Figure 4.
| Characteristic | Category | Frequency (N=418) | Percentage %) |
|---|---|---|---|
| Want to have another child | Do not want | 151 | 36.1 |
| Want soon | 54 | 12.9 | |
| Want, but wait for more than 2 years from now | 197 | 47.1 | |
| Undecided | 16 | 3.8 | |
| Discussion with partner on the number of children | Never discussed | 141 | 33.7 |
| Ever discussed | 277 | 66.3 | |
| Recommendation on FP use | Yes | 180 | 43.1 |
| No | 238 | 56.9 | |
| Husband/partner approval on FP use | No | 162 | 38.8 |
| Yes | 256 | 61.2 | |
| Religious affiliation | Catholic | 136 | 32.5 |
| Protestant | 241 | 57.7 | |
| Muslim | 30 | 7.2 | |
| Other | 11 | 2.6 | |
| Influence of religion on use of FP | No | 309 | 73.9 |
| Yes | 109 | 26.1 |
Table 3: Socio-cultural characteristics of women attending women aged 15 – 24 years attending FRRH.
Prevalence of Family Planning Use among Women Attending Women Aged 15-24 Years Attending FRRH
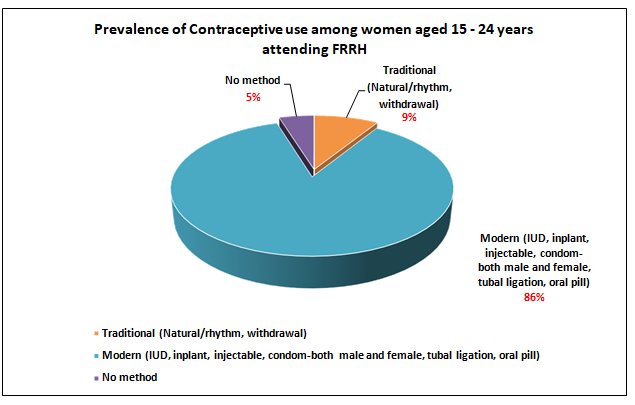
Out of 418 respondents, 20 (4.8%) were not using any family planning, while the rest 398 (95.2%) were using at least one method of family planning. Modern methods are more popular to women than traditional methods; 86.4 percent of women use at least one modern method, and only 8.9 percent know a traditional method as shown on Table 4 and Figure 5.
| Method | Frequency (N=418) | Percentage (%) |
|---|---|---|
| Traditional (Natural/rhythm, withdrawal) | 37 | 8.8 |
| Modern (IUD, inplant, injectable, condom-both male and female, tubal ligation, oral pill) | 361 | 86.3 |
| No method | 20 | 4.8 |
Table 4: prevalence and contraceptive method use among women attending women aged 15 – 24 years attending FRRH.
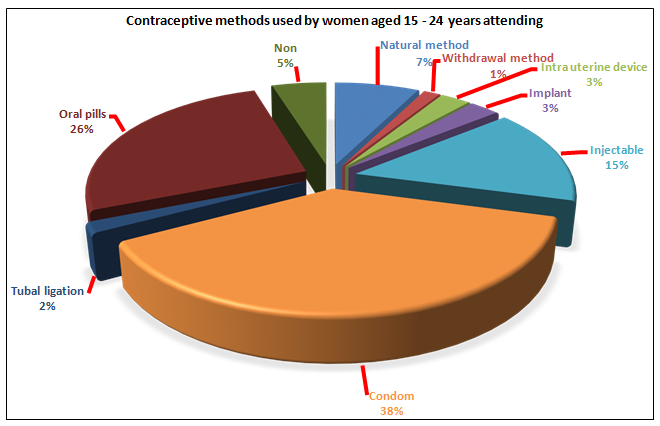
Contraceptive methods used by 15-24 years aged women attending FRRH: The most preferred contraceptive method among the women was use of condoms 38.0% followed by Oral pills 26.3% and then Injectables 15.1%. 1.4% still relied the traditional withdraw method while 4.8% didn’t opt for any method as shown in Table 5 and Figure 6.
| Contraceptive method | Frequency (418) | Percentage (%) |
|---|---|---|
| Natural method | 31 | 7.4 |
| Withdrawal method | 6 | 1.4 |
| Intra uterine device | 11 | 2.6 |
| Implant | 11 | 2.6 |
| Injectable | 63 | 15.1 |
| Condom | 159 | 38 |
| Tubal ligation | 7 | 1.7 |
| Oral pills | 110 | 26.3 |
| Non | 20 | 4.8 |
Table 5: Contraceptive methods used by 15 – 24 years aged women attending FRRH (N=418).
Socio-Demographic, Economic and Cultural Characteristics that Influence the Use of Contraceptives among Women Attending Women Aged 15 24 Years Attending FRRH
In this results section, further analysis has been conducted to explore possible relationship that will contribute to making inferences. This section shows the relationship between the socio- demographic, economic and cultural characteristics of the respondents and the use of family planning.
Socio-Demographic that Influence the Use of Contraceptives among Women Attending Women Aged 15-24 Years Attending FRRH
All the narrative to this effect is presented in Table 5. Women in age group 20-24 years seek postnatal care services more 320 (76.6%) than those in age category 15-19 years 98(23.4%). The use of a particular family planning options vary with age group. Use of oral pill increase from 23.9% in age group 15-19 years to 27.2% in age group 20-24 years, injectable increase significantly from 6.1% in 15-19years to 17.8% in 20-24 years, condom increased from 35.7% (15-19 years) to 38.8% (20-24 years). However for the other method (implant, tubal ligation, withdrawal method and injection) use of FP it decreased from 18.4% in 15-19 years to 11.6% in 20-24 years. The chi square test results indicated an association between age of the women and the contraceptive of choice (χ2 ==23.72: df =4, p=0.001).
Majority of women aged 15-24 years seeking postnatal care and using FP methods (82.5%) have education level of secondary and below. For the women with education level of secondary school and below, the most preferred family planning method is condom while the least popular the natural method (5.8%). On the other hand, other methods (27.4%) was the most popular while the natural method and the pill were the least preferred (15.1%) as shown on table 4. There was a significant association between the level of education and FP methods (χ2 =34.73, df =4, p=0.001).
The percentage of use of family planning method varied with the number of children of the respondent. Condom remained the most popular method for respondents with one child (39.4%) as well as for those with 2 or more children (35.5%). The natural method was the least used by respondents with one child (6.9%) and was also the least popular method for those with two or more children (8.5%) compared to other methods. This study found no significant association between the number of living children and contraceptive use (χ2 =7.37, df =4, p=0.12). There were two categories of marital status; not married (single, separated, divorced) 37.6% and married 62.4%. The most commonly used method of FP among both marital statuses is condom. The natural method was the least popular for the married with a proportion of 4.6% while the injectable was the least used among the not married. Among the never married group, the use of other methods had a higher proportion than other FP 31.8%. There was a statistical significant association between the marital status and FP method (χ2=33.34, df =4, p=0.001). The percentage use of FP varied with duration in marriage/ relationship of the women. The condom is the most popular method (39.5%) for those with 0-4 years in marriage while condom and oral pill are most widely used (30.3%) by respondents with 5 years and above in relationship. However there was no significant association between Marriage duration and the FP method (χ2=3.95, df =4, p=0.4) (Table 6).
| Characteristics | Category | Family planning option | Statistical Test | ||||
|---|---|---|---|---|---|---|---|
| Natural method n (%) | Others n (%) | Injectable n (%) | Condom n (%) | Oral pills n (%) | Significant at p<0.05 | ||
| Age group | 15 - 19years | 16(16.3) | 18(18.4) | 6(6.1) | 35(35.7) | 23(23.9) | χ2=23.72 df=4 |
| 20 - 24years | 15(4.7) | 37(11.6) | 57(17.8) | 124(38.8) | 87(27.2) | p=0.001 | |
| Level of education | Secondary and below | 20(5.8) | 35(10.1) | 47(13.6) | 144(41.7) | 99(28.7) | χ2=34.73 df =4 |
| Above secondary | 11(15.1) | 20(27.4) | 16(21.9) | 15(20.5) | 11(15.1) | p=0.001 | |
| Number of children | 1 child | 19(6.9) | 39(14.1) | 33(11.9) | 109(39.4) | 77(27.8) | χ2=7.37 df =4 |
| 2 or more Children | 12(8.5) | 16(11.3) | 30(21.3) | 50(35.5) | 33(23.4) | p=0.12 | |
| Marital status | Married | 12(4.6) | 19(7.3) | 47(18) | 107(41) | 76(29.1) | χ2=33.34 df =4 |
| Not married | 19(12.1) | 36(22.9) | 16(10.2) | 52(33.1) | 34(21.7) | p=0.001 | |
| Duration in marriage/ relationship | 0 - 4 years | 24(6.8) | 44(12.5) | 55(15.6) | 139(39.5) | 90(25.6) | χ2=3.97 df =4 |
| 5 years and above | 7(10.6) | 11(16.7) | 8(12.1) | 20(30.3) | 20(30.3) | p=0.4 |
Table 6: Association between demographic characteristics and Contraceptive use (N=418). Socio-Economic Characteristics that Affec
Table 6: Association between demographic characteristics and Contraceptive use (N=418). Socio-Economic Characteristics that Affect Contraceptives use among Women Attending Women Aged 15–24 Years Attending FRRH The occupation of the women was categorized into three major divisions. Out of the 418, 41.4%were employed in the public/private sector, 32.8% were self-employed and 25.8% were unemployed. In all the three occupations, condom method was the most up taken FP method 159/418(38%) whereas, the natural method was the least FP methods 31/418(7.4%) among this study group. Condom was the most widely used method for the unemployed, self-employed and employed (public and private sector) at 36.1%, 36.5% and 40.5% respectively compared to all other methods. Among the unemployed group, the least FP method was injectable (4.6%), while the natural method was the least popular among the self-employed (6.6%) and those employed in the public and private sector (4.6%). There was statistical significance association between occupation and FP methods; (χ2=34.93, df =8, p=0.001). Of the 418 respondents, 84.2% felt their income was not enough while 15.8% had enough income. Condom was also the most preferred method for women with enough income (31.8%) and for those whose income was not enough (39.2%). The natural method was the least used form of FP for both respondents without enough income (7.4%) and for those with enough income (7.6%). There was no statistical significance association between income and FP methods; (χ2=7.08, df =4, p=0.13) as shown in Table 6.
A higher proportion of the women at FRRH 290(69.4%) did not get information on contraceptive use through media while 128(30.6%) did. Among those who did not get information from media, a higher proportion were using condom, 119(39.3%), followed by oral pills 79(27.2%) and the least was the natural method 24(8.3%). on the other hand, among those who received information from media, there was no much difference in proportion with the other group that received information. Condom was the most used (35.2%) while the natural method was the least used (5.5%). There was no statistical significance association between the source of information and the Family planning option; (χ2 = 6.25, df =3, p=0.18) as shown in Table 7.
| Characteristics | Category | Family planning option | Statistical Test | ||||
|---|---|---|---|---|---|---|---|
| Natural method n (%) | Others n (%) | Injectable n (%) | Condom n (%) | Oral pills n (%) | Significant at p< 0.05 | ||
| Occupation | Unemployed | 14(13) | 27(25) | 5(4.6) | 39(36.1) | 23(21.3) | χ2=34.93 df =8 p=0.001 |
| Self employed | 9(6.6) | 13(9.5) | 24(17.5) | 50(36.5) | 41(29.9) | ||
| Employed in private/public sector | 8(4.6) | 15(8.7) | 34(19.7) | 70(40.5) | 46(26.6) | ||
| Income adequate to meet your basic needs | Not enough | 26(7.4) | 41(11.6) | 50(14.2) | 138(39.2) | 97(27.6) | χ2=7.08 df =4 p=0.13 |
| Enough | 5(7.6) | 14(21.2) | 13(19.7) | 21(31.8) | 13(19.7) | ||
| Get family planning on media | No | 24(8.3) | 31(10.7) | 42(14.5) | 114(39.3) | 79(27.2) | χ2=6.26 df =4 p=0.18 |
| Yes | 7(5.5) | 24(18.8) | 21(16.4) | 45(35.2) | 31(24.2) |
Table 7: Association between socio-economic characteristics of the 15-24 years old women attending FRRH and contraceptive use (N=
Socio-Cultural Characteristics that Affect Contraceptives Use among Women Attending Women Aged 15–24 Years Attending FRRH
All the narrative to this effect is presented in Table 7. Women practicing the catholic faith were 32.5% while 57.7% were protestant, and 9.8% were Muslims and others. The majority of the women were affiliated to protestant faith. Majority of the respondent reported their religion does not influence their use or non-use of contraceptives with a representation of 73.9%; however, the use and non- use of the contraceptives is influenced by religion with a representation of 26.1%. women affiliated to catholic and protestant faiths had even distribution in all the FP methods however among the Muslim and Hindus injectable and pills had minimal users. There was a significance association between the FP method and religion, (χ2=31.7, df =4 and p=0.001). The use of condom increased from 32.6% for those who have never discussed with their husband/partner of to
40.8% for those who have ever discussed. Use of oral pills increased from 24.1% for those who have never discussed with their husband/partner of to 27.4% for those who have ever discussed. Use of injectable was 8.5% for those who have never discussed with their husband/partner and 12.2% for those who have ever discussed. Discussion with partner on family planning is found to be a significant factor affecting its uptake among women aged 15-24 years; (χ2= 29.3, df =4, p = 0.001).
Among the women interviewed, 57.2% of their partners approved use of family planning and 42.8% did not approve. The oral pill was the most used method (48%) among those whose partners did not approve FP use, whereas condom was used by majority (59.4%) of respondents whose partners approved use of family planning. Partners approval to family planning option is statistically significant to the family planning option (χ2= 143.54, df =4, p = 0.001) (Table 8).
| Characteristics | Category | Family planning option | Statistical Test | ||||
|---|---|---|---|---|---|---|---|
| Natural method n (%) | Others n (%) | Injectable n (%) | Condom n (%) | Oral pills n (%) | Significant at p<0.05 | ||
| Religious affiliation | Catholic | 15(11) | 10(7.4) | 22(16.2) | 60(44.1) | 29(21.3) | χ2=29.14 df =8 p=0.001 |
| Protestant | 12(5) | 31(12.9) | 37(15.4) | 90(37.3) | 71(29.5) | ||
| Muslim and Others | 4(9.8) | 14(34.1) | 4(9.8) | 9(22) | 10(24.4) | ||
| Discuss with your partner on number of children to have | Never discussed | 19(13.5) | 30(21.3) | 12(8.5) | 46(32.6) | 34(24.1) | χ2=29.3 df =4 p=0.001 |
| Ever discussed | 12(4.3) | 25(9) | 51(18.4) | 113(40.8) | 76(27.4) | ||
| Does your husband/ partner approve FP use | No | 13(7.3) | 19(10.6) | 44(24.6) | 17(9.5) | 86(48) | χ2=143.54 df =4 p=0.001 |
| Yes | 18(7.5) | 36(15.1) | 19(7.9) | 142(59.4) | 24(10) |
Table 8: Association between socio-cultural characteristics of the respondents and use of family planning (N=418).
Multivariate Analysis of Factors that Influence Contraceptive Use at Bivariate Level
All those factors that were significant at bivariate level were subjected to linear logistic regression analysis in order to control for any confounders. The factors that were significant at bivariate analysis included Age, level of education, Religion affiliation, occupation, marital status, discussion with the partner, Approval from the partner to use a given FP and the desire to have another child. At multivariate analysis, Age, level of education, occupation, discussion with the partner, approval from the partner to use a given FP and the desire to have another child were significantly associated to contraceptive use among 15 – 24 years old women attending FRRH.
Linear logistic regression model of multivariate analysis after controlling all possible confounders was used to determine the factors that influence contraceptive use among 15 – 24 years old women attending FRRH. The factors that were significant at multivariate were: The age of women, Level of education, Employment status, discuss with your husband/partner on number of children to have and Want to have another child. Those factors that were not significant include, Marital Status and Religious affiliation as shown in Table 9.
| Dependent Variable | B | S.E. | Wald | df | Sig. | Exp (B) |
|---|---|---|---|---|---|---|
| a.) Agea | 0.399 | 0.426 | 0.878 | 1 | 0.034 | 1.491 |
| b.) Marital Statusb | 0 | 0 | 0.076 | 1 | 0.783 | 1 |
| c.) Level of educationc | -0.997 | 0.491 | 4.118 | 1 | 0.042 | 0.369 |
| d.) Religious affiliationd | -0.057 | 0.147 | 0.148 | 1 | 0.7 | 0.945 |
| e.) Employment statuse | 1.413 | 0.62 | 5.19 | 1 | 0.003 | 4.108 |
| f.) Discuss with your husband/partner on number of children to havef | -0.6 | 0.377 | 2.533 | 1 | 0.011 | 0.549 |
| g.) Want to have another child g | -0.466 | 0.377 | 1.526 | 1 | 0.017 | 0.627 |
| Constant | 1.532 | 2.041 | 0.563 | 1 | 0.453 | 4.626 |
Table 9: Multivariate Analysis of factors that influence contraceptive use among 15-24 years old women attending FRRH.
Where the equation of the regression was: Y= e(a+b+c+d+c+f+g) Where a, b, c, d, e, f and g are values that were significant at bivariate analysis in the table above Table 9: Multivariate Analysis of factors that influence contraceptive use among 15-24 years old women attending FRRH.
Discussion of Results
Introduction
This chapter presents the discussion of the study results as per the study objectives with a comparison to conclusions made by other scholars.
Socio Demographic, Cultural and Economic Characteristics of Women Aged 15–24 Years Attending FRRH
A total of 418 young women aged 15 – 24 years attending FRRH participated in the study with a 100% response rate. Majority 76.6% were in age category 20-24 years, had attained secondary education 82.5%, were married 62.4%), had a single child 66.3%. This socio demographic stratification of this particular class of women studied is consistent with results from similar studies in Kenya, Namibia and Nigeria. In all these studies from the three respective countries majority of the young women studied were aged 20–24 years, had given birth to at least a single child and by average had attained a secondary education [36, 43].
The consistency in the social demographic stratification of young women from all these four studies including this very one can be attributed to the similarity of population of these four countries as reported by UNFPA population report of 2018 and therefore any sampling of this group of people can easily show a justifiable consistency [18]. However a similar study in Britain reported a different demographic stratification were majority of the women was aged 15 – 19 years having given birth but with even a lower education qualification. This variation from this study can be attributed to the known fact that young women from the developed are introduced to sexual activity through education and actual indulgence at a much lower age than their sub- Saharan counterparts and is much attributed to the cultural differences [32]. Majority of the women felt that their income was not enough 84.2% even though 41.4% were employed in the private or public and 32.8% were self-employed. This finding is characteristic of the income indicators of a low income country like Uganda proven by the UDHS and [11, 46].
Prevalence of Contraceptive Use among Women Aged 15-24 Years Attending FRRH
In this we have established that 95.2% of women aged 15-24 years attending FRRH at least use one of the modern or traditional contraceptive methods known. This indicates that the prevalence of contraceptive use among women of this category in the population serviced by FRRH is 95.2%. This prevalence of contraceptive use is way higher than the current national prevalence estimates of about
60% [8]. This prevalence is also way higher than the most recent established prevalence of contraceptive use among adolescents that recorded 9.4% [9] and is also higher that the national 2020 target set at 50% of the total reproductive women [28].
This variation of this finding from the previous ones and predicted national targets can be explained by the demographic stratification of this population. As already indicated the demographics of this population, majority of them had attained at least a secondary education 82.5%. Education level has been shown to be a predictor of contraceptive use in studies in Ethiopia, Nigeria, South Africa, Kenya, Tanzania and Rwanda and rate of use has also been indicated to increase with improved education [19, 24, 30, 36, 46].
However, even though there are variation between this study findings with national figures known, consistent high prevalence rates of contraceptive use have been reported amongst women of such age group in Britain, Canada, Egypt and Malaysia. Such high rates of contraceptive use in those settings were attributed to high education levels and income that both factors where significantly associated with contraceptive access [22, 33, 35]. The most preferred contraceptive method among the women was use of condoms 38.0% followed by Oral pills 26.3% and then Injectables 15.1%. 1.4% still relied the traditional withdraw method while 4.8% didn’t opt for any method and this ranking order is consistent with other findings in Uganda, Kenya and Ethiopia [31, 36, 48].
Socio Demographic, Cultural and Economic Factors that Influence the Family Planning Option Among Women Aged 15-24 Years Attending FRRH
In a bivariate model analysis, this study was able to establish significant relationships between age of the women and the contraceptive of choice p=0.001, level of education and contraceptive methods p=0.001, marital status and contraceptive methods p=0.001, discussion with partner and contraceptive uptake p = 0.001, partner’s approval to family planning p = 0.001 and finally contraceptive method with religion p=0.001. A study in Nigeria reported conclusions of statistical significance between age of women and choice of contraception where women of higher age groups opted for more long term contraceptive options, and this was attributed to the increased engagements in income activities that limited the women’s ability to settle for pregnancies. In this study we did not explore causal explanations but it’s evident that these findings are consistent [24].
In a 2020 study in Ethiopia, Woldu BF, et al. [49] explores long term determinants of contraceptive use and established that marital status, partner’s opinion and level of education were significantly associated with contraceptive use among Ethiopian women which indicates a consistence in the findings of that study and our findings. One compounding reason provided for these relationships was knowledge as a determinant of all the three factors. In conclusions of a stakeholder scholars’ review of contraceptive uptake trends in Uganda, key among the significant determinants of contraceptive uptake were partners’ involvement in contraception choice, education level of women and marital status. Findings of this review are consistent with findings of this study [50].
Association between the Contraceptive Options and Family Planning Needs among Women Aged 15-24 Years Attending FRRH
In Linear logistic regression model; in multivariate analysis after controlling all possible confounders to determine the factors that influence contraceptive use among 15-24 years old women attending FRRH, the factors that remained significant were: The age of women, Level of education, Employment status, discussion with husband/ partner on number of children to have and need to have another child. The significant relationship outcome of all these factors is corroborated by similar findings in Ghana, Ethiopia, Nigeria and two other studies in Ugandan. This consistency in the findings of those studies and this particular one among 15 – 24 year olds at FRRH can be attributed the near similarity in the demographic characterization of the populations in all these places as they are all under sub Saharan Africa [20, 21, 27, 51, 52, 53].
Conclusions, Limitations and Recommendations
Limitations
- By the cross-sectional nature of this study, this limits a conclusion to a causal relationship and therefore interpretation of findings from this study cannot be applied to that effect.
- This was a single hospital facility based study; therefore findings of this study cannot be used to make generalized conclusions about contraceptive trends among the general population because other women in similar category may be attending other health facilities other than FRRH.
- The authors take cognizance of a recall bias possibility that can possibly affect the conclusions on contraceptive use trends and thus may lead to over or under conclusions of prevalence and significant relationships.
Recommendations
Based on the findings of this study, we thus recommend the following;
- Family planning education is integrated as a continuous Programme for all women of reproductive age willing to undertake it at FRRH.
- Partners of the women have been shown to be significant halves in determination of contraceptive use among the women. We recommend inclusive programs that integrate the male function in the equation so as to achieve effective out comes of contraceptive use.
Conclusion
The prevalence of contraceptive use among 15-24 years old women attending FRRH is 95.2% higher than the national achievement target 50% of all reproductive age women by 2020. All factors constant; age of women, their level of education, employment status, involvement husband/ partner on number of children to have and need to have another child were significant determinants of contraceptive use among this population of women attending FRRH.
References
-
WHO (2014) World’s Adolescents A second chance in the second decade. World Health Organization, pp: 3-6.
-
Manzi F, Ogwang J, Akankwatsa A, Wokali OC, Obba F, et al. (2018) Factors Associated with Teenage Pregnancy and its Effects in Kibuku Town Council, Kibuku District, Eastern Uganda: A Cross Sectional Study. Primary Health Care Open Access 8: 2.
-
Kemi B, Christian O, Alabi JA, Isola O (2015) Unplanned Parenthood: The Socio- Economic Consequences of Adolescent Child-bearing in Nigeria. Journal of Education and Practice 6(31): 15-18.
-
World Health Organization (2019) Sexual, Reproductive, Maternal, Newborn, Child and Adolescent Health Policy Survey 2018-2019. WHO, pp: 1-31.
-
UNICEF (2018) Adolescent pregnancy Key Facts. Department of Agriculture and Water pp: 15-16.
-
UNICEF (2016) The Global Strategy for Women’s, Children’s And Adolescents’ health.
-
Kaphagawani NC, Kalipeni E (2017) Sociocultural factors contributing to teenage pregnancy in Zomba district, Malawi. Global Public Health 12(6): 694-710.
-
Uganda Bureau of Statistics, United Nations Population Fund UNFPA, & AID (2019) Uganda family planning atlas. In Uganda Bureau of Statistics 1: 1.
-
Sserwanja Q, Musaba MW, Mukunya D (2021) Prevalence and factors associated with modern contraceptives utilization among female adolescents in Uganda. BMC Women’s Health pp: 1-7.
-
Campbell B, Martinelli heckadon S, Wong S (2013) UNPFA State of the World’s Population.
-
UBOS UB of S (2017) Uganda Demographic and Health Survey 2016. In Uganda Demographic and Health Survey 2016: 6.
-
Ochen AM, Chi PC, Lawoko S (2019) Predictors of teenage pregnancy among girls aged 13-19 years in Uganda: a community based case-control study. BMC Pregnancy and Childbirth 19(211): 1-14.
-
Vallerand RJ, Deshaies P, Cuerrier JP, Pelletier LG, Mongeau C (1992) Ajzen and Fishbein’s Theory of Reasoned Action as Applied to Moral Behavior: A Confirmatory Analysis. Journal of Personality and Social Psychology 62(1): 98-109.
-
Dennis ML, Radovich E, Wong KLM, Owolabi O, Cavallaro FL, et al. (2017) Pathways to increased coverage : an analysis of time trends in contraceptive need and use among adolescents and young women in Kenya, Rwanda, pp: 1-13.
-
Nsubuga H, Sekandi JN, Sempeera H, Makumbi FE (2016) Contraceptive use, knowledge, attitude, perceptions and sexual behavior among female University students in Uganda : a cross-sectional survey. BMC Women’s Health pp: 1-11.
-
United Nations (2019) United Nations: Contraceptive Use by Method. UN, pp: 28.
-
Mokomane Z, Khan N (2009) Towards a 10- year review of the population policy implementation in South Africa (1998-2008): Sexual and reproductive health and rights, South Africa. Department of Social Development.
-
UNFPA (2018) United Nations Population Fund Annual Report.
-
Hlongwa M, Thompson TM, Makhunga S, Hlongwana K, Desapriya E (2020) Evidence on factors influencing contraceptive use and sexual behavior among women in South Africa: A scoping review. Medicine 99(12): e19490.
-
Tibaijuka L, Odongo R, Welikhe E, Mukisa W, Kugonza L, et al. (2017) Factors influencing use of long-acting versus short-acting contraceptive methods among reproductive-age women in a resource- limited setting. BMC Women’s Health 17(1): 1-13.
-
Mathewos S, Mekuria A (2018) Teenage Pregnancy and Its Associated Factors among School Adolescents of Arba Minch Town, Southern Ethiopia. Ethiopian Journal of Health Sciences 28(3): 287-298.
-
IPPF, UNFPA (2012) Key Factors Influencing Contraceptive Use in seven Middle-Income Countries of Eastern Europe and Central Asia. Pp: 1-4.
-
Aina I, Pelemo AA (2019) The Use of Contraceptives in Nigeria: Benefits, Challenges and Probable Solutions. Journal of Law, Policy and Globalization 86: 1-12.
-
Ujah OI, Ocheke AN, Mutihir JT, Okopi JA, Ujah IAO (2017) Postpartum contraception: determinants of intention and methods of use among an obstetric cohort in a tertiary hospital in Jos, North Central Nigeria. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 6(12): 5213-5218.
-
Tran NT, Yameogo WME, Langwana F, Gaffield ME, Seuc A, et al. (2018) The maternal and newborn health thematic fund: Case studies on strengthening midwifery services to avert maternal and newborn deaths. UNFPA 18(1): 122.
-
Nabugoomu J, Seruwagi GK, Hanning R (2020) What can be done to reduce the prevalence of teen pregnancy in rural Eastern Uganda?: Multi-stakeholder perceptions. Reproductive Health 17(1): 1-12.
-
Celik LDC (2016) Access to contraceptives in Uganda: Approachability, acceptability, and users’ abilities. Pp: 1-33.
-
Ministry of Health (2015) Uganda Family Planning Costed Implementation Plan 2015-2020.
-
Tuyishime E, Källestål C, Selling K (2016) Factors Associated with the Prevalence of Contraceptive Use among Women of Reproductive Age in Rwanda: A Cross- Sectional Study using Demographic and Health Survey Rwanda 2010. International Journal of Women’s Health 135(15): 23-44.
-
Mahande MJ, Shayo E, Amour C, Mshana G, Msuya S (2020) Factors associated with modern contraceptives use among postpartum women in Bukombe district, Geita region, Tanzania. Plos One pp: 1-14.
-
Bellizzi S, Mannava P, Nagai M, Sobel HL (2020) Reasons for discontinuation of contraception among women with a current unintended pregnancy in 36 low and middle- income countries. Contraception 101(1): 26-33.
-
Staveteig S, Maliick L, Winter R (2015) Uptake and discontinuation of long acting reversible contraceptives in low-income countries. DHS Analytical Studies, pp: 1-59.
-
Kopp DM, Rosenberg NE, Stuart GS, Miller WC, Hosseinipour MC, et al. (2017) Patterns of contraceptive adoption, continuation, and switching after delivery among Malawian women. Plos One 12(1): 1-12.
-
Ontiri S, Ndirangu G, Kabue M, Biesma R, Stekelenburg J, et al. (2019) Long-acting reversible contraception uptake and associated factors among women of reproductive age in rural Kenya. International Journal of Environmental Research and Public Health 16(9): 1-11.
-
Gunawardena N, Fantaye AW, Yaya S (2019) Predictors of pregnancy among young people in sub-Saharan Africa: A systematic review and narrative synthesis. BMJ Global Health 4(3): 1-8.
-
Mayhew SH, Colombini M, Kimani JK, Tomlin K, Warren CE, et al. (2017) Fertility intentions and contraceptive practices among clinic-users living with HIV in Kenya: A mixed methods study. BMC Public Health 17(1): 1-15.
-
Joshi AK, Tiwari DP, Poudyal A, Shrestha N, Acharya U, et al. (2020) Utilization of family planning methods among postpartum mothers in Kailali District, Nepal. International Journal of Women’s Health 12: 487-494.
-
Sendo EG (2021) Utilization and Associated Factors of Emergency Contraception among Female College Students in Addis Ababa, Ethiopia. Quality in Primary Care 29(1): 1-7.
-
National Population Council (2018) The State of Uganda Population Report 2018. Journal of Chemical Information and Modeling 53(9): 1689-1699.
-
Sensoy N, Korkut Y, Akturan S, Yilmaz M, Tuz C, et al. (2018) Factors Affecting the Attitudes of Women toward Family Planning. Family Planning.
-
Communities at the Centre (2019) Communities at the Centre. Global Aids Update, pp: 121-138.
-
Freddy RK (2019) Factors influencing the use of modern contraceptive methods among rural women of child bearing age in the Democratic Republic of the Congo. Journal of Family Medicine and Primary Care 8(8): 2582- 2586.
-
Indongo N (2020) Analysis of Factors Influencing Teenage Pregnancy in Namibia. Medical Research Archives 8(6).
-
Mcleod SA (2019) Sampling Methods. Simply Psychology, pp: 1-5.
-
United Nations Inter-agency Group for Child Mortality Estimation (2020) In: You D, Hug L, et al. (Eds.), United Nations Children’s Fund, World Health Organization, World Bank Group, & United Nations. Population division. A neglected tragedy : the global burden of stillbirths.
-
Ahinkorah BO, Kang M, Perry L, Brooks F, Hayen A (2021) Prevalence of first adolescent pregnancy and its associated factors in sub-Saharan Africa: A multi- country analysis. Plos One 16(2): 1-16.
-
Tesfa E, Gedamu H (2018) Factors associated with utilization of long term family planning methods among women of reproductive age attending Bahir Dar health facilities, Northwest Ethiopia. BMC Research Notes 11(1): 1-7.
-
Ashebir W, Tadesse T (2020) Associated Factors of Postpartum Modern Contraceptive Use in Burie District, Amhara Region, Ethiopia. Journal of Pregnancy 2020: 1-9.
-
Woldu BF, Ermolo TL, Lemu LG, Gejo NG (2020) Long- acting reversible contraception utilization and associated factors among women in extended postpartum period in Hossana town, southern Ethiopia: cross sectional study. Contraception and Reproductive Medicine 5(1): 1-6.
-
Report on review of the family planning costed implementation plan (fp-cip) in uganda. USAID, pp: 1-93.
-
Garko B, Umeh G, Nuhu I (2019) Access to contraceptives for adolescents in northern Nigeria-a cross-sectional study from three secondary health facilities in Kaduna metropolis, Kaduna. Gates Open Research.
-
Paschal AA, Matthew AA (2015) Factors influencing the uptake of family planning services in the Talensi District, Ghana. Pan African Medical Journal pp: 1-9.
-
Tebeje B, Workneh D (2017) Prevalence, Perceptions and Factors Contributing to Long Acting Reversible Contraception Use among Family Planning Clients, Jimma Town, Oromiya Region, South-West Ethiopia. Journal of Women’s Health Care 6(1): 1-10.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria