Prevalence and Associated Factors of Liver Disease among Adults: A cross–sectional study at a Health facility in North-Eastern Part of Ghana
Liver diseases are linked to several causes, including viral hepatitis, misuse of drugs, and alcoholism. Most patients recently diagnosed with liver disease, develops end-stage liver diseases, such as hepatocellular carcinoma subsequent to a rise in liver related mortalities. The aim of this study was to determine the prevalence and associated factors of liver disease in adult patients at the Zebilla Government Hospital in North Eastern part of Ghana. The study employed descriptive crosssectional design and employing a systematic sampling technique, 374 participants were recruited. A structured questionnaire was administered to conduct face to face interview to solicit study data. Data was analysed with Stata (16). Both Univariate and bivariate analysis were conducted and an alpha value <0.05 indicated significant association between the dependent and independent variables. The study found a 38.8% of liver disease among participants. Participants Age (p=0.001), Sex (p=0.032), Marital status (p=0.026) and Alcohol intake (p=0.0001) associated with liver diseases. Liver disease was high among participants and factors such as age, sex and alcoholic intake associated with its occurrence. Frequent screening of liver diseases coupled with intensification of public education on risk factors of liver diseases would help decrease its emergence and associated complications. Further study is recommended to explore the economic burden of liver diseases among patients.
Introduction
Liver disease is the leading cause of liver-related deaths worldwide [1]. Despite significant interventions such as hepatitis B vaccination and advances in antiretroviral therapy in the treatment of liver disease [2], the incidence of liver disease such as non-fatty liver and alcoholic liver disease following end-stage liver-related morbidity is increasing [3]. Recent estimates suggest that approximately 1.5 billion people living with chronic liver disease are experiencing an epidemiological shift to liver complications which is attributed to concomitant increases in drug use, inappropriate alcohol use, and metabolic syndrome, despite ongoing containment measures on the incidence of liver disease [2]. Available statistics show that the world population is experiencing a dramatic increase in non-alcoholic liver disease from 8.2% to 10% within two decades [3]. Compared to obesity and type II diabetes, non-alcoholic liver disease is increasing, with prevalence increasing from 75% in 2016 to 30% in 2019 [4].
This has contributed to 4% of global deaths being attributed to liver disease, and this proportion is expected to increase due to unhealthy diets and increasing alcohol consumption [3]. Among liver diseases, alcoholic liver disease is the most common chronic liver disease and its prevalence is expected to increase due to current global alcohol consumption [5]. Recent evidence has shown that approximately 38.7% of hepatitis B virus infections and 68.4% of hepatic encephalopathy associated with liver cirrhosis in healthcare settings account for 41.3% of liver disease [2] For example, in Ghana, viral hepatitis B infection contributes to the incidence of most liver diseases and accounts for 10–12.3% of the total Ghanaian population, contributing to 3.4% of all deaths in Ghana [6, 7]. Although there are interventions to prevent and treat these diseases, they are still the leading cause of liver complications such as cirrhosis [8]. Although the liver is an important organ with multiple functions for the human body [9].
However, its disease condition impairs its functions which are attributed to causes such as viral infections, alcohol consumption, fatty foods, autoimmune diseases and drug abuse [10, 11, 12, 13, 14]. Most people with liver disease are generally asymptomatic [15]. However, when diagnosed clinically, patients with acute and chronic liver disease present with clinical signs and symptoms such as yellowish eyes and skin, dark urine, pale stools, itchy skin, and elevated liver enzymes [15]. Most patients with liver disease have liver cysts and cancer [16, 17]. In addition, patients with liver disease suffer from primary biliary cholestasis and sclerosing cholangitis, which eventually attacks the immune system and leads to decreased immunity [13]. In addition, chronic liver disease results in end-stage liver complications [18], leading to increased liver-related mortality [19]. As of 2020, a significant proportion of all hospital outpatients are diagnosed with various types of liver diseases, such as alcoholic and viral hepatitis. Of those clinically diagnosed with liver disease, a significant proportion were unaware of the liver disease and therefore were diagnosed at an advanced stage of the disease. Recent evidence has shown that there are studies on liver disease in Ghana that focus on the epidemiological characteristics and behavioral factors associated with liver disease [7, 8, 15]. However, there is paucity of data about the prevalence and associated factors of liver disease in North-Eastern part of Ghana. Therefore, this study aimed to determine the prevalence and associated factors of liver disease in adult patients seeking medical care at Zebilla Government Hospital.
Materials and Methods
Study Setting and Study Design
The Bawku West District is one of the fifteen districts in the Upper East Region of Ghana and has its capital at Zebilla. The district borders the Republic of Burkina-Faso to the north, Binduri District to the east, Talensi District and Nabdam District to the west, and East Mamprusi to the south. The district covers a land area of 1,070 square kilometers, accounting for 12% of the total land area, and is the fourth largest district in the region. Zebilla Government Hospital is a primary and referral healthcare facility for the people of Zebilla and the surrounding area. It is a health insurance registered and accredited facility that provides 24- hour service to the people of the district. Major services provided by the facility as part of its daily services are general consultations, maternal and child welfare, diagnostic services, surgical services, pediatric, mental health and public health services. This study employed a cross-sectional design and this was deemed appropriate as eligible participants for the study were assessed at a single encounter with investigators.
Study Population
This study recruited participants aged Eighteen (18+) years old and above who accessed the healthcare facility under study. Consented and eligible participants were included in the study, while non-consenting patients who were intellectually disabled due to past or current psychiatric illness were excluded. Again, participants who were seriously ill and were admitted were excluded due to their inability to answer study questionnaire.
Sample Size and Sampling Technique
The study estimated a sample size of 374 adult patients using the simple Cochran formula n=Z2×𝑝 (1−𝑝)/e² Using the Out-patient attendance register of adults as a sampling frame, a systematic sampling technique was employed to select eligible participants into the study.
Data Collection Tool and Technique
The participants data were collected using a validated and structured questionnaire. The tool was developed by the researchers after careful consideration of the objectives. The data collection tool contained information on the socio- demographic characteristics of the participants and the associated factors of liver diseases. The data collection tool was pre-tested on adult patients at Binaba Health Center as patients cared for by this facility had similar characteristics as the participants under study. After the pre-test interview, improvements were made to the questionnaire before the final document was printed. The questionnaire was administered by the researchers, assisted by trained research assistants. The personal interviews were conducted with the participants in English and in the local dialect (Kusaa). The researchers read the questions to participants who could not read in their local dialect and typed the correct answers on their behalf. Participants who could read and write answered the questionnaire themselves after having explained the study to them in detail.
Data Analysis
Study data was analyzed using STATA version 16. After checking for data completeness, accuracy and clarity of the primary data collected, the data were entered into Microsoft excel, exported to STATA 16 where categorical variables were coded, analysed and presented as proportions and percentages. The Pearson Chi-Square test was employed to determine the association between the liver disease and associated factors and alpha value < 0.05 established significant association.
Research Ethics
Permission to conduct the study was obtained from the Navrongo Research Center Ethics Committee (ID: NHRCIRB447). Approval was obtained from the management and authorities of the Municipal Health Directorate and the Management of the Government Hospital in Zebilla. Full consent was obtained by communicating the aim and rationale of the study to participants to ensure their voluntary participation. The participants were informed that participation in the study is voluntary and that they can withdraw from the study at any time. Participants were assured of confidentiality and anonymity and that under no circumstances would their identity or other important records be disclosed to third parties during and after the processes of data collection, analysis and dissemination of results.
Limitations of Study
The data collected for the study was based on self- reported from participants and as such vulnerable to recall biases due to memory distortions. Additionally, the study was limited to advance examination of participants’ liver disease such as Liver sonography and magnetic resonance imaging. Findings were also limited to adults’ patients from 18 years and above, as such generalizing findings to population below eighteen years would not be appropriate in this study.
Results
The study recruited 374 participants yielding a 97% response rate. The mean age of participants was 40±16 years. About 98/374(26.2%) of participants were between 18-27 years, 83/374(22.2%) between 28-37 years, 67/374(17.9%). About 201/374(53.7%) of the participants were females whilst 173/374(46.3%) were males. Most 209/374(55.9%) of the participants were married, 160/374(42.8%) were single. About 155374/ (41.4%) of participants had basic education, 94/374 (25.1%) secondary education, 94/374(25.1%) diploma and 29/374(7.8%) with degree qualification. Most 217/374(58.0%) were Christians whilst 144/374(38.5%) were Moslems. With regard to alcoholic intake, 111/374(29.68%) of the participants take alcohol whilst 263/374(70.32%) do not take alcohol. With the type of alcoholic intake, about 57/111(51.4%) of participants take Gin, 21/111(18.9%) drink alcoholic bitters, 13/111(11.7%) take Pito, 19/111(17.1%) drink Beer, Concerning the frequency of alcoholic intake, about 23/111(20.7%) daily take alcohol, 72/111(64.9%) sometimes drink alcohol and 16/111(14.4%) most of the times take alcohol (Table 1).
| Variable | Category | N=374 | Percentage (%) | |
|---|---|---|---|---|
| Age (years) | ||||
| 18-27 | 98 | 26.2 | ||
| 28-37 | 83 | 22.2 | ||
| 38-47 | 67 | 17.9 | ||
| 48-57 | 55 | 14.7 | ||
| 58-67 | 51 | 13.6 | ||
| 68-77 | 20 | 5.3 | ||
| Sex | ||||
| Male | 173 | 46.3 | ||
| Female | 201 | 53.7 | ||
| Marital status | ||||
| Married | 209 | 55.9 | ||
| Single | 160 | 42.8 | ||
| Co-habiting | 5 | 1.3 | ||
| Education | ||||
| Basic education | 155 | 41.4 | ||
| Secondary education | 94 | 25.1 | ||
| Diploma | 94 | 25.1 | ||
| Degree | 29 | 7.8 | ||
| Masters | 2 | 0.5 | ||
Table 1: Distribution of Socio-Demographic Characteristics of Participants.
Prevalence of Liver Diseases among Participants
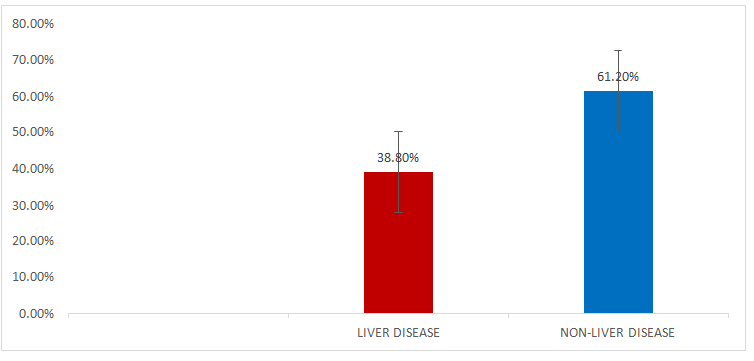
The prevalence of liver disease was determined from participant’s self-reported liver diseases and confirmed by medical practioners at the facility. About 145/374 (38.8%) of the participants had liver diseases whilst 229/374(61.2%) of the participants had no liver disease (Figure 1).
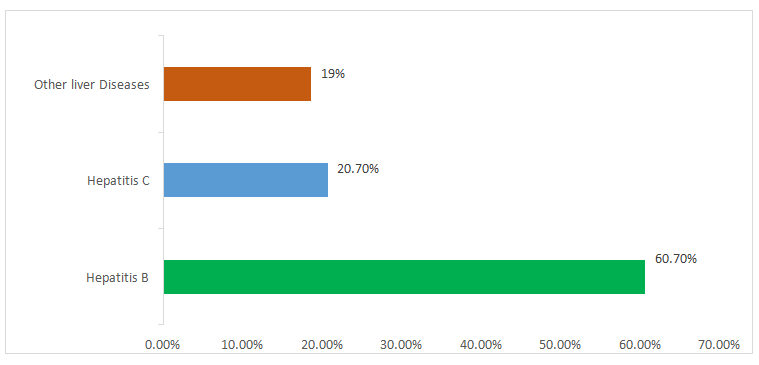
About 88/145(60.7%) of the participants with liver diseases had hepatitis B infection,30/145(20.7%) had hepatitis C and 27/145(18.6%) had other types of liver diseases such as alcoholic liver disease and fatty liver disease (Figure 2).
Associated Factors with Liver Diseases among Participants
At a 95% confidence interval, the Pearson Chi-Square test was used to determine the association between liver disease and associated factors. It was established that, Age of participants associated with liver disease (χ2=20.4, P=0.001), Sex of participants (χ2=4.9, p=0.032), Marital status of participants (χ2=7.2, p=0.026) associated with liver disease. Again, intake of alcohol associated with liver disease (χ2=24.4, p=0.0001) (Table 2).
| Liver Diseases | χ2 (p-value) | |
|---|---|---|
| Variable | Liver Disease, n (%) | Non-liver disease, n (%) |
| Age (Years) | 20.4(0.001) | |
| 18-27 | 47(32.4) | 51(22.3) |
| 28-37 | 43(29.7) | 40(17.5) |
| 38-47 | 24(16.6) | 43(18.8) |
| 48-57 | 13(9.0) | 42(18.3) |
| 58-67 | 13(9.0) | 38(16.6) |
| 68-77 | 5(3.4) | 15(6.6) |
| Sex | 4.9(0.032) | |
| Male | 57(39.3) | 116(50.7) |
| Female | 88(60.7) | 113(49.3) |
| Marital Status | 7.23(0.026) | |
| Married | 71(49.0) | 138(60.3) |
| Single | 70(48.3) | 90(39.3) |
| Cohabiting | 4(2.8) | 1(0.4) |
| Religion | 1.34(0.51) | |
| Islam | 54(37.2) | 90(39.3) |
| Christian | 84(57.9) | 133(58.1) |
| Others | 7(4.8) | 6(2.6) |
| Highest level of education | 4.52(0.34) | |
| Basic education | 54(37.2) | 101(44.1) |
| Secondary education | 38(28.4) | 56(24.5) |
| Diploma education | 36(26.2) | 58(25.3) |
| Degree | 16(11.0) | 13(5.7) |
| Masters | 1(0.7) | 1(0.4) |
| Alcoholic intake | 22.4(0.001) | |
| Takes alcohol | 24(16.6) | 91(39.7) |
| Do not take alcohol | 121(83.4) | 138(60.3) |
| Frequency of alcoholic intake | 1.18(0.55) | |
| Daily | 5(20.0) | 18(20.9) |
| Sometimes | 18(72.0) | 54(62.8) |
| Most times | 2(8.0) | 14(16.3) |
Table 2: ** Factors associated with liver diseases among participants.
X2: Chi-square, *: p<0.05 statistically significant Table 2: Factors associated with liver diseases among participants.
Discussion
This study determined the prevalence and associated factors of liver disease in adult patients at a healthcare facility in north-eastern Ghana. A prevalence of 38.8% of liver diseases was established and factors such as age, sex, marital status and alcohol consumption were associated with the disease prevalence. Comparing the current prevalence of 38.8% with other results, [20] reported a higher prevalence of 72.2% of liver disease which differed from the current study outcome. In China, a 38.7% prevalence of liver disease in patients seeking medical assistance was reported, and this was consistent with recent study outcome [21]. In Japan, the outcome of a cross-sectional study of patients assessing health care was reported and it was documented that 28.7% had liver disease, which did not collaborate well with the current study prevalence [22].
The report of a prospective study conducted to determine the predictors of in-hospital mortality from hepatic encephalopathy in patients found that 31.7% of patients had liver disease, which did not agree well with the results of this recent study [2]. The possible reasons for the differences in the study results could be attributed to the differences in the study methods and the behavioral patterns of the participants with regard to alcohol consumption and poor eating habits. There is evidence that the high burden of liver disease is the cause of metabolic disorders such as abnormal lipid metabolism leading to lipidemia, a factor that contributes to insulin resistance after the early onset of diabetes mellitus [23, 24] and thus contributes to the risk of diabetes mellitus and hypertension, secondary to chronic kidney disease [25, 26, 27]. There is evidence that alcoholics are significantly associated with liver disease, and this was consistent with the results of the present study [28]. Similarly, patients who consume alcohol were found to develop liver disease [29] and this was consistent with the current study report. A significant association between alcoholism and the incidence of liver disease has been reported in Ethiopia, which also agrees well with recent survey results [3, 30]. Additionally, [31] documented an association between alcohol consumption and the manifestation of liver disease, which supported the current study result. A similar finding has been reported that alcohol consumption is associated with the incidence of liver disease [32].
In Ghana, there is evidence that alcohol consumption correlates well with the occurrence of liver disease which supported the findings of the present study [33]. Similarly there was a strong association between alcohol consumption and the occurrence of liver disease which also was consistent with this present study [34]. The age of the participants was found to be related to liver disease. A cross-sectional study found that age is associated with liver disease which supported current survey results. Similarly found a strong association between age and liver disease, which also correlated well with the results of the present study [35]. In Ghana, a prospective study reported that there was no association between liver disease and age, and the results did not agree with this current study. In contrast, showed that age is associated with risk of liver disease and the results were therefore consistent with the results of the present study [34]. This recent study showed an association between gender and the incidence of liver disease. Gender was well associated with risk of liver disease [35]. In conclusion, it should be recognized that increases in alcohol consumption with respect to aging increases the risk of liver disease and progression to chronic liver disease, leading to higher healthcare and administrative cost, a burden on family members to provide supportive care, and lost work time, resulting in financial losses and decreased productivity in a nation.
Conclusion and Recommendations
Participants’ self-assessment of liver disease was high; therefore prompt intervention to decrease prevalence is desirable. In addition, factors such as alcohol consumption, gender, age, and marital status of the participants showed a significant association to liver disease. There should be an effective alliance between health policy makers and stakeholders of health to expand policies and protocols for mandatory screening of patients presenting for treatment in health care facilities. In addition, health promotion programs on liver disease, risk factors and complications should be intensified by local health authorities through local radio stations. Non-governmental organisations and community health officials should work together to organize screening for liver disease for residents of the community while helping those infected with liver disease to secure better healthcare. The study is also recommended for additional qualitative investigations into the burden of patients with diagnosed liver disease.
Acknowledgements
The authors wish to appreciate the support and approval of management and staff of the facility. We are also most grateful to participants who fully consented to partake in the study and to anyone who in diverse ways contributed to the success of this study.
Conflict of interest
The authors declare that no competing interest existed among them
Funding
The authors self-financed this paper
Data and material availability
Data and materials for the study are available upon request from the corresponding author
Approval and consent to participate
The study was approved by the management of the municipal health directorate and the local leaders of the selected communities before its commencement. Eligible participants voluntarily agreed to participate without coercion.
Authors Contributions
PA and MOP: conceived the topic and drafted the introduction. MOP, EDK and MD: Developed the methodology. MOP, PA and EDK: analysed the study data. DS, EK and II wrote the discussion. MOP, II and BKIA: drafted the manuscript and reviewed it. All authors proof read the paper and accepted it for submission.
References
-
Asrani SK, Devarbhavi H, Eaton J, Kamath PS (2019) Burden of liver diseases in the world. Journal of Hepatology 70(1): 151-171.
-
Duah A, Nkansah A, Osei Poku F, Duah F, Addo BP (2021) Sociodemographic characteristics, complications requiring hospital admission and causes of in-hospital death in patients with liver cirrhosis admitted at a district hospital in Ghana. PloS one 16(6): e0253759.
-
Xiao J, Wang F, Wong NK, Zhang, R, Sun R, Li, et al. (2019) Global liver disease burdens and research trends: analysis from a Chinese perspective. Journal of Hepatology 71(1): 212-221.
-
Lu, FB, Zheng, KI, Rios RS, Targher G, Byrne CD, et al. (2020) Global epidemiology of lean non‐alcoholic fatty liver disease: a systematic review and meta‐analysis. Journal of Gastroenterology and Hepatology 35(12): 2041-2050.
-
Rehm J, Shield KD (2019) Burden of alcohol use disorders and alcohol liver disease. Biomedicines 7(4): 99.
-
Helegbe GK, Tanko F, Aryee PA, Lotsu SA, Asaarik MJ, et al. (2020) High hepatitis b seroprevalence, low knowledge, and poor attitude towards hepatitis b virus infection among market women in Bolgatanga Metropolis in the Upper East Region of Ghana. Journal of Tropical Medicine.
-
Ofori Asenso R, Agyeman AA (2016) Hepatitis B in Ghana: a systematic review & meta-analysis of prevalence studies (1995-2015). BMC infectious diseases 16(1): 1-15.
-
Adjei CA, Naab F, Donkor ES (2017) Beyond the diagnosis: a qualitative exploration of the experiences of persons with hepatitis B in the Accra Metropolis, Ghana. BMJ Open 7(11): e017665.
-
Tunnage J, Yates A, Nwoga C , Singoei V, Owuot J (2021) Hepatitis and tuberculosis testing are much less common than HIV testing among adults in Kisumu, Kenya: results from a cross-sectional assessment. BMC Public Health 21(1): 1143.
-
Namjou B, Lingren T, Huang Y, Parameswaran S, Cobb BL, et al. (2019) enrichment analyses of non-alcoholic fatty liver disease identify new trait-associated genes and pathways across eMERGE Network. BMC medicine 17: 1-19.
-
Leise MD, Poterucha JJ, Talwalkar JA (2014) Drug- induced liver injury. In Mayo clinic proceedings. Elsevier 89(1): 95-106.
-
Lee D, Chiavaroli L, Ayoub Charette S, Khan TA, Zurbau A, et al. (2022) Important food sources of fructose- containing sugars and non-alcoholic fatty liver disease: a systematic review and meta-analysis of controlled trials. Nutrients 14(14): 2846.
-
Sgamato C, Rocco A, Compare D, Minieri S, Marchitto SA, (2023) Autoimmune liver diseases and SARS-CoV-2. World Journal of Gastroenterology 29(12): 1838.
-
Ray G (2022) Management of liver diseases: Current perspectives. World Journal of Gastroenterology 28(40): 5818.
-
Ntiamoah A, Essel Cobbinah D, Asenso Nyarko T, Yeboah R, Asare DA (2021) Prevalence of liver lesions in small ruminants (sheep and goats) slaughtered at the Kumasi abattoir, Ghana. Animal Research International 18(3): 4159-4165.
-
Zabaleta N, Torella L, Weber ND, Aseguinolaza G (2022) mRNA and gene editing: Late breaking therapies in liver diseases. Hepatology 76(3): 869-887.
-
Palit S, Mukherjee S, Niyogi S, Banerjee A, Patra D (2018) Quinoline-Glycomimetic Conjugates Reducing Lipogenesis and Lipid Accumulation in Hepatocytes. Chem Bio Chem 19(16): 1720-1726.
-
Tu T, Block JM, Wang S, Cohen C, Douglas MW (2020) The lived experience of chronic hepatitis B: a broader view of its impacts and why we need a cure. Journal of Virues 12(5): 515.
-
Amponsah Dacosta E (2021) Hepatitis B virus infection and hepatocellular carcinoma in sub-Saharan Africa: Implications for elimination of viral hepatitis by 2030. World Journal of Gastroenterology 27(26): 6025.
-
Park SH (2020) Personal Protective Equipment for Healthcare Workers during the COVID-19 Pandemic. Infect Chemother 52(2): 165-182.
-
Guo W, Qin P, Li XN, Wu J, Lu J, et al. (2021) Free triiodothyronine is associated with hepatic steatosis and liver stiffness in euthyroid Chinese adults with non- alcoholic fatty liver disease. Frontiers in endocrinology 12: 711-956.
-
Eguchi Y, Hyogo H, Ono M, Mizuta T, Ono N, et al. (2012) Prevalence and associated metabolic factors of non- alcoholic fatty liver disease in the general population from 2009 to 2010 in Japan: a multicenter large retrospective study. Journal of Gastroenterology 47: 586-595.
-
Pei K, Gui T, Kan D, Feng H, Jin K (2020) An overview of lipid metabolism and nonalcoholic fatty liver disease. Bio Med Research International pp: 4020249.
-
Gong Z, Tas E, Yakar S, Muzumdar R (2017) Hepatic lipid metabolism and non-alcoholic fatty liver disease in aging. Molecular and cellular endocrinology 455: 115- 130.
-
Zhao YC, Zhao GJ, Chen Z, She ZG, Cai J, et al. (2020) Non-alcoholic fatty liver disease: an emerging driver of hypertension. Hypertension 75(2): 275-284.
-
Oikonomou D, Georgiopoulos G, Katsi V, Kourek C, Tsioufis C, et al. (2018) Non-alcoholic fatty liver disease and hypertension: co-prevalent or correlated. European Journal of Gastroenterology & Hepatology 30(9): 979- 985.
-
Zou ZY, Shen B, Fan JG (2019) Systematic review with meta-analysis: epidemiology of non-alcoholic fatty liver disease in patients with inflammatory bowel disease. Inflammatory Bowel Diseases 25(11): 1764-1772.
-
Younoss ZM, Ong JP, Takahashi H, Yilmaz Y, Eguchi Y, et al. (2022) A global survey of physician’s knowledge about nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol 20(6): e1456-e1468.
-
Cerovic I, Mladenovic D, Jesic R, Naumovic T, Brankovic M, et al. (2013) Alcoholic liver disease/nonalcoholic fatty liver disease index: distinguishing alcoholic from nonalcoholic fatty liver disease. European Journal of Gastroenterology & Hepatology 25(8): 899-904.
-
Di Ciaula A, Bonfrate L, Krawczyk M, Fruhbeck G, Portincasa P (2022) Synergistic and detrimental effects of alcohol intake on progression of liver steatosis. International Journal of Molecular Sciences 23(5): 26- 36.
-
Cao G, Yi T, Liu Q, Wang M, Tang S (2016) Alcohol consumption and risk of fatty liver disease: a meta- analysis. Peer J 4: e2633.
-
Axley PD, Richardson CT, Singal AK (2019) Epidemiology of alcohol consumption and societal burden of alcoholism and alcoholic liver disease. Clinics in Liver Disease 23(1): 39-50.
-
Danquah I, Bedu Addo G, Terpe KJ, Micah F, Amoako YA, et al. (2012) Diabetes mellitus type 2 in urban Ghana: characteristics and associated factors. BMC Public Health 12: 210.
-
Mohammed BS, Aidoo M (2020) Drug treatment of patients with liver cirrhosis in a tertiary hospital in Northern Ghana: does it comply with recommended guidelines. International Journal of Hepatology.
-
Caballeria L, Pera G, Auladell MA, Tora P, Munoz L, et al. (2010) Prevalence and factors associated with the presence of nonalcoholic fatty liver disease in an adult population in Spain. European Journal of Gastroenterology & Hepatology 22(1): 24-32.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria