Longstanding Rural-Urban Disparities Exacerbated by COVID-19: The Experiences of Older Residents in West Texas: Lessons Learned
Purpose: The primary objective of this study was to examine differences in COVID-19 testing, diagnosis, symptoms, preventive measures, and healthcare resources and services between urban- and rural-dwelling older adults of the West Texas region. Methods: Data from surveys of 303 adult urban and rural residents (>40 years old) between June 2020 and January 2021 were conducted. County-level data from the Texas Department of State Health Services (TDSHS) were analyzed for the period between March 2020 and February 2021. Findings: County-level data from TDSHS revealed greater access to COVID-19 testing and higher case numbers yet lower COVID-19 fatalities among urban residents. On the contrary, rural counties had fewer overall COVID-19 cases, less access to COVID-19 testing, and higher COVID-19 fatalities. Conclusion: The COVID-19 pandemic exasperated the long-standing healthcare disparities documented between rural and urban neighborhoods, resulting in devastating consequences in rural areas suffering from poor healthcare infrastructure. Findings revealed disparities in COVID-19 experiences among urban and rural communities, which highlight the need for strategies aimed at improving healthcare access in rural areas through telemedicine and other innovative approaches.
Introduction
The COVID-19 pandemic has resulted in more than 6.3 million deaths worldwide as of June 2022 and an estimated
533 million positive cases of COVID-19 [1]. The impact of COVID-19 has been devastating and pervasive, deepening longstanding health inequities among society’s most vulnerable, including rural communities which comprise
20% of the United States (US) population [2]. However, current reporting of the pandemic’s impact is limited by state-level aggregations [3] subsequently overlooking the urban-rural (i.e., county-level) differences. This oversight limits our understanding of the effects and responses to the COVID-19 pandemic while further widening the health disparity between individuals living in rural and urban settings. Therefore, this study bridges this gap by assessing and comparing rates of COVID-19 vaccination, COVID-19 prevalence, availability/utilization of healthcare resources, and services between urban- and rural-dwelling residents of the South Plains Texas Region.
Prior to the COVID-19 pandemic, evidence revealed disproportionate access to healthcare services, greater likelihood of medical and mental health comorbidities, and higher rates of poverty among rural dwellers [4]. These urban-rural disparities have resulted in persistent challenges in promoting the health and well-being of rural communities throughout and following the COVID-19 pandemic [5]. For example, rural residents face higher risks of severe illness and mortality from COVID-19 as they are likely older in age, have higher rates of underlying chronic diseases and disabilities, and have less access to healthcare [6]. Given that medical complications due to COVID-19 increase with age (i.e., 80% of mortality related to COVID-19 was among adults 60 or older) elderly rural dwellers are particularly at risk [6]. Incidence and mortality rates of COVID-19 in rural communities (crude mortality rate was 185.50) during 2020 also began to exceed the rates among urban (crude mortality rate was 123.70) communities-rural counties had 61.85 additional deaths due to COVID-19 per 100,000 population [7, 8]. Despite the overwhelming risk of COVID-19-related mortality among rural dwellers, there is a paucity of research comparing the effects of COVID-19 in West Texas between urban and rural communities.
Healthcare Infrastructure and Transportation Challenges
The literature has prominently documented the disparate access to healthcare services, particularly specialized care, among rural communities [9]. One empirically supported reason is transportation hurdles that rural communities face. More specifically, they are more likely to travel for extended periods to reach healthcare facilities, often through hazardous terrain, causing many rural dwellers to postpone their healthcare appointments, even when sick [10, 11]. Indeed, a previous study found among adults who received the COVID-19 vaccine in rural counties (38.9%), a large proportion (14.6%) traveled to nonadjacent counties for vaccination (i.e., farther from their county of residence). Whereas in urban areas, 45.7% received the COVID-19 vaccine and only 10.3% of persons in urban counties travel to receive the COVID-19 vaccine in nonadjacent counties [12]. These reports indicate COVID-19 testing sites may be difficult to travel to or even inaccessible to rural communities compared to urban communities.
Furthermore, research has documented that rural areas during the COVID-19 pandemic suffered from overcrowded hospitals, widespread hospital closure, and a lack of healthcare professionals. The CDC [5] reported 170 hospitals in rural America have closed since 2005, 700 more after the COVID-19 pandemic are at risk for closure, and a shortage of 600,000 healthcare professionals in rural communities [13], further limiting the availability of healthcare services for individuals in rural areas. As rural communities grapple with how to navigate the lack of access to proper healthcare, which impacts their ability to protect from and receive treatment for COVID-19, they may experience a greater level of distress due to this lack of access to proper healthcare. A systematic review has found rural dwellers, compared to urban dwellers, are more likely to experience psychological distress due to COVID-19 [14]. These results reflect poorer access to resources, lower SES status, education, and increased medical comorbidity among rural communities.
Poorer Health Status and Vaccine Hesitancy in Rural Communities
The CDC [15] reports that individuals in rural communities are more likely to die from the five leading causes of death given their older age, high rates of cigarette use, high blood pressure, obesity, lack of physical activity, high rates of poverty, and lack of access to healthcare. As rural populations are older and thus more likely to be immunocompromised, they are at the greatest risk for COVID-19-associated morbidity and mortality. One of the most efficient ways to prevent COVID-19 hospitalizations is through vaccinations [12]. COVID-19 vaccine hesitancy is the reluctance or unwillingness to be vaccinated and has been documented most notably in rural communities due to feelings of fear, misinformation/disinformation, lack of community health literacy, and medical distrust [10]. Therefore, it is important to understand the vaccination rates of rural versus urban community dwellers.
Prior evidence suggests rural communities are less likely to engage in preventive health behaviors [16]. One study found that rural dwellers reported negative attitudes toward the effectiveness of performing preventive behaviors, and had lower levels of information appraisal skills (i.e., less likely to evaluate the relevance and salience of health-related information) [17]. Misinformation is a persistent challenge to engaging in preventive health behaviors as it may lead to taking ineffective and potentially harmful remedies, ignoring healthcare guidelines, and engaging in behavior that increases the transmission of the virus [18]. Given that rural communities tend to have higher rates of individuals with low socioeconomic status (SES) and education, they may be more likely to trust health information from sources that are lower in accuracy and quality [10].
Knowledge Gaps
The COVID-19 pandemic taught us that challenges during a pandemic are predominantly around reducing the rate of COVID-19 transmissions in rural communities, which precedes the vaccination uncertainty. Rural communities lack the adequate health infrastructure needed to support a large capacity of COVID-19 patients. They are also isolated from specialized healthcare systems, have fewer opportunities to provide medical literacy pertaining to COVID-19, and have a staffing shortage of healthcare workers to serve the population. The exodus of medical staff, because of the COVID-19 pandemic, remains a significant barrier to broadening the scope of care and further impaired critical care to rural areas. The COVID-19 pandemic has magnified the inequalities in healthcare that prevail among rural-urban communities. Unfortunately, as a result, the healthcare infrastructure in rural communities was not prepared to tackle the enormity of the COVID-19 pandemic or to protect those most at risk. Without research examining these disparities, it will lead to a continuation and increase of these disparities. We must learn from the pandemic to improve overall healthcare in rural areas and to prepare for the possibility of future pandemics.
Therefore, it is vital to understand urban and rural residents’ experiences during the pandemic to inform public health efforts in these areas. In the wake of the pandemic communities were faced with reduced access to care, overpopulated hospitals and shortage of healthcare workers, a widening digital divide, and unequal access to lifesaving treatments and vaccinations to fight against the virus. As society defines its path forward from the COVID-19 pandemic, we must reflect on the devasting and pervasive impacts of the pandemic. To improve the health and well- being of communities living in rural counties-we must understand how poor healthcare infrastructure impacts the ability to receive vaccinations and COVID-19 tests. It is through this critical deliberation can we examine previous inadequacies to confront the systemic barriers to access to healthcare and inform future reforms. To date, few studies have explored critical urban-rural differences in West Texas on residents’ experiences and access to health care. Therefore, the proposed study elucidates the availability of resources and services between rural and urban communities. This information will inform prevention and treatment strategies to ameliorate the impact of COVID-19 strains and future pandemics. More specifically, this study
- Assessed and compared the rates of COVID-19 vaccination, COVID-19 prevalence, and symptomology between urban- and rural-dwelling residents of the South Plains Texas Region;
- Examined COVID-19 prevention measures between urban- and rural-dwelling residents; and
- Evaluated availability/utilization of health care resources and services. Using county-level data, these results depicted COVID-19 trends in testing, cases, and fatalities across urban and rural counties in West Texas.
Methods
Participants
Participants residing in rural counties were recruited from Project FRONTIER (Facing Rural Obstacles to Healthcare Now Through Intervention, Education & Research), a longitudinal epidemiological study on cognitive aging in rural South Plains communities. Three hundred and three participants consented to take a one-time survey over the phone (see Table 1 for demographic characteristics). Out of the 303 participants surveyed, the majority (70.06%, n = 212) were female, and ages ranged from 44 and 95 (M = 70.06, SD = 11.22). About 38.94% (n = 118) of participants reported being Hispanic/Latino(a), 60.07% (n = 182) reported being White/Non-Hispanic, 25.41% (n = 77) reported being White and Hispanic/Latino(a), and 1.32% (n = 4) reported being Black. The mean reported number of persons in the household was 2.24 (SD = 1.19; range: 1 to 8 persons per household).
The Urban population from Lubbock, TX totaled 46.53% of the entire sample (n = 141). The rural population included 29.70% (n = 90) from Parmer County, 11.88% (n = 36) from Cochran County, 10.56% (n = 32) from Bailey County, and 1.32% (n = 4) from Hockley County. Many participants had health insurance: 66.22% had public insurance (n = 198), 22.74% had private insurance (n = 68), and 11.04% were uninsured (n = 33). Nearly 1 in 5 participants (n = 61; 20.40%) had a high school degree or GED equivalent, while 40 participants (13.38%) had a bachelor’s degree, and 36 participants (12.04%) had a graduate degree. In comparing the urban (i.e., Lubbock) to the four rural counties (i.e., Bailey, Cochran, Hockley, and Parmer)—participants residing in the urban county were older, predominately White/Non- Hispanic, reported higher levels of education, and greater access to public/private health insurance than the combined rural counties subsample (see Table 1).
| Variable | Total Sample (n=303) | Lubbock Co. Subsample (n=141) | Bailey, Cochran, Hockley, and Parmer Co. Subsample (n=162) | |||
|---|---|---|---|---|---|---|
| N (%) | Mean (SD) | N (%) | Mean (SD) | N (%) | Mean (SD) | |
| Age (years) | 70.06 (11.22) | 73.57 (8.90) | 67.01 (12.13) | |||
| Sex | ||||||
| Male | 91 (30.03) | 43 (30.50) | 48 (29.63) | |||
| Female | 212 (69.97) | 98 (69.50) | 114 (70.37) | |||
| Race | ||||||
| White, Not Hispanic/ Latino | 182 (60.07) | 127 (90.07) | 55 (33.95) | |||
| White, Hispanic/Latino | 77 (25.41) | 13 (9.22) | 64 (39.51) | |||
| Black or African American | 4 (1.32) | 0 | 4 (2.47) | |||
| Other | 40 (13.20) | 1 (0.71) | 39 (24.07) | |||
| Hispanic/Latino Ethnicity | ||||||
| Yes | 118 (38.94) | 10 (7.09) | 108 (66.67) | |||
| No | 185 (61.06) | 131 (92.91) | 54 (33.33) | |||
| Highest level of education | ||||||
| Some elementary, middle school | 53 (17.73) | 0 | 53 (33.33) | |||
| Some high school | 27 (9.03) | 4 (2.86) | 23 (14.47) | |||
| High school graduate/ GED | 61 (20.40) | 30 (21.43) | 31 (19.50) | |||
| Bachelor’s degree | 40 (13.38) | 30 (21.43) | 10 (6.29) | |||
| Graduate degree | 36 (12.04) | 31 (22.14) | 5 (3.14) | |||
| Health insurance status | ||||||
| 33 (11.04) | 2 (1.44) | 31 (19.38) | ||||
| Public insurance | 198 (66.2) | 118 (84.89) | 80 (50.00) | |||
| Private insurance | 68 (22.74) | 19 (13.67) | 49 (30.63) |
Table 1: Participant demographics for total sample and by Lubbock County subsample vs. 4-rural counties subsample.
Seventy-three participants (24.25%) reported having none of the conditions described above. Table 1: Participant demographics for total sample and by Lubbock County subsample vs. 4-rural counties subsample.
Seventy-five participants (24.92%) reported having heart disease as their only medical condition, while 102 participants (33.88%) reported having heart disease in combination with another chronic condition (e.g., cancer). Twenty-four participants (7.92%) had asthma with another chronic condition; 10 participants (3.30%) had a chronic lung disease (i.e., chronic obstructive pulmonary disease or emphysema), and 52 participants (17.16%) reported having an autoimmune disorder (i.e., rheumatoid arthritis or Crohn’s disease) along with other conditions.
Data and Design
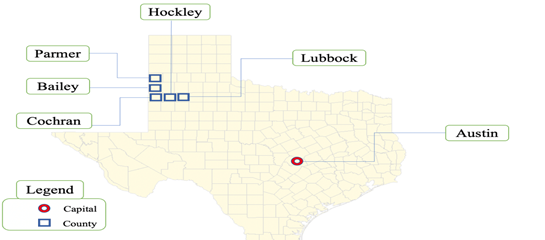
While Rurality and urbanicity are multidimensional constructs (Pedersen et al., 2020), we have differentiated the two based on micropolitan and metropolitan areas [19]. Micropolitan (micro) areas include 10,000-49,999 persons, whereas metropolitan (metro) areas include urban areas with 50,000 or more persons. The rural population is represented by four rural counties: Bailey County (population 7,000), Cochran County (population 2,853), Hockley County (population 23,021), and Parmer County (population 9,605).
Participants residing in urban areas were recruited from Lubbock County (population 310,569) through a previous study on health and aging at the Texas Tech University Health Sciences Center Garrison Institute on Aging (TTUHSC GIA). See Figure 1 for the residential breakdown. This study employed data from two sources:
- A telephone survey to assess COVID-19-related experiences among residents in Lubbock County (urban county) and four rural counties (Bailey, Cochran, Hockley, and Parmer counties); and
- Publicly available, county-level data on COVID-19 acquired from the Texas DSHS. Surveys were conducted in either English or Spanish in accordance with each participant’s language preference.
Data were captured using Qualtrics software and exported as a Microsoft Office Excel spreadsheet for analysis in SAS (Version 9.4). County-level COVID-19 data on the selected counties of interest were downloaded as Excel spreadsheets from the Texas Department of State Health Services (Texas DSHS) website between March 4, 2020 and February 4, 2021. COVID-19 trends in testing, cases, and fatalities across urban and rural counties in West Texas, were carried out using Texas DSHS. This research was approved by the Institutional Review Board at the TTUHSC.
Measures
Demographic Information
Gender, age, race, ethnicity, and county of residence were collected. Household composition, health insurance status, and educational attainment were also captured.
Health Status
Participants were asked about their diagnosed medical conditions, if they smoke cigarettes (i.e., Do you smoke cigarettes?), and vaping behaviors (i.e., Do you use any other tobacco products, including vaping, but not including cigarette smoking?).
COVID-19 Questionnaire
Participants were asked if they tested for COVID-19, and if diagnosed with COVID-19, the approximate dates of diagnosis and duration of symptoms, for themselves and any other person(s) in their household who had been diagnosed with COVID-19. All participants were asked if they had direct contact with anyone who tested positive for COVID-19 in the past 24 hours. Participants were also asked about the presence of COVID-19 related symptoms (i.e., fever, dry cough, shortness of breath, decreased sense of smell/taste, nausea or vomiting, sore throat, muscle or joint aches, diarrhea/ gastrointestinal problems, or other symptoms) experienced by the participant and anyone else in the household in the past 7 days. Assessment of healthcare utilization was examined (i.e., “Have you sought care from a healthcare provider either in-person, over the phone, or via telemedicine?”). Mental health was assessed using two items: “Over the past 7 days, approximately how often have you been bothered by the following problems: a) feeling nervous, anxious, or on edge; and b) felt depressed?” Response categories were not at all, several days, more than half the days, and nearly every day. An open-ended question was asked for participants to share their thoughts on the COVID-19 situation and any challenges they have faced.
Preventive Health Behaviors
Participants were asked if they received a flu vaccine during the 2019/2020 year, and whether they exercised the following behaviors:
- Washing hands for 20 seconds,
- Wearing a mask in public,
- Social distancing (6 ft. apart), and
- Staying at home and limiting outdoor activities.
Access to Technology
Participants were asked, “Which electronic devices do you have easy access to?” Response choices included: smart cellphone, non-smart cellphone, landline telephone, iPad or tablet, laptop computer, desktop computer, and other.
Data Analysis Plan
A map of the five-county study area was created (see, Figure 1). Participant demographics were summarized for the total sample, and by urban vs. rural subsamples (Table 1). COVID-related indicators are described in Table 2 for the total sample and by urban vs. rural subsamples. Differences between “urban residents” and “rural residents” were assessed using two-independent sample _t-_tests (statistical significance assessed at: p < 0.05). Analyses were conducted in SAS version 9.4. A thematic analysis was conducted on participants’ responses to the final open-ended question pertaining to their experiences related to the COVID-19 pandemic. Themes were identified when a majority of participants endorsed that concept. Qualitative results (themes and representative quotes) are presented in Table 3.
| Variable | Total Sample (n=303) | Lubbock Co. Subsample (n=141) | Bailey, Cochran, Hockley, and Parmer Co. Subsample (n=162) |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Had been tested for COVID-19 | |||
| Yes | 73 (24.09) | 54 (38.30) | 19 (11.73) |
| No | 230 (75.91) | 87 (61.70) | 143 (88.27) |
| COVID-19 Results | |||
| Negative | 38 (52.05) | 30 (55.56) | 8 (42.11) |
| Positive | 31 (42.47) | 23 (42.59) | 8 (42.11) |
| Awaiting results | 4 (5.48) | 1 (1.85) | 3 (15.79) |
| Felt nervous, anxious, or on edge over the past 7 days | |||
| Not at all | 276 (92.93) | 129 (93.48) | 147 (92.45) |
| Several days | 15 (5.05) | 8 (5.80) | 7 (4.40) |
| More than half the days | 3 (1.01) | 0 | 3 (1.89) |
| Nearly every day | 3 (1.01) | 1 (0.72) | 2 (1.26) |
| Felt depressed over the past 7 days | |||
| Not at all | 278 (94.56) | 129 (94.85) | 149 (94.30) |
| Several days | 11 (3.74) | 6 (4.41) | 5 (3.16) |
| More than half the days | 2 (0.68) | 0 | 2 (1.27) |
| Nearly every day | 3 (1.02) | 1 (0.74) | 2 (1.27) |
| Received Flu Vaccine | |||
| Yes | 228 (77.55) | 120 (87.59) | 108 (68.79) |
| No | 66 (22.45) | 17 (12.41) | 49 (31.21) |
| Theme | Representative Quotes | Respondent Characteristics | |
| Social Isolation | “Ready for it to be over. I like to hug and shake hands and with this virus, it has eliminated that.” | Male, age 70-80, Parmer Co., Interviewed June 2020 | |
| “I wish it was over so everyone could be happy again.” | Male, age 70-80, Parmer Co., Interviewed June 2020 | ||
| “I don’t like not being able to go out, not even to go and sit down at a place and eat. I miss that.” | Female, age 80-90, Lubbock Co., Interviewed August 2020 | ||
| Safety Precautions | “I make sure that I wear my mask and keep my distance. Taking the precautions that the doctors have told us will keep us safe!” | Male, age 60-70, Lubbock Co., Interviewed September 2020 | |
| “I wish people would do what they are told to do. I think we would be in a better place.” | Female, age 80-90, Parmer Co., Interviewed July 2020 | ||
| “The young people think they are invincible and are making this worse. They need to take precautions and keep this virus from making it worse.” | Male, age 60-70, Cochran Co., Interviewed August 2020 | ||
| “Wearing a mask is worse for our health. We wear a mask only where they are required. With the masks we breathe in more bacteria. Washing hands is just good hygiene, no one should have to tell you to wash your hands.” | Female, age 70-80, Cochran Co., Interviewed September 2020 | ||
| “Everybody needs to stop partying and follow the COVID-19 rules” | Male, age 50-60, Cochran Co., Interviewed August 2020 | ||
| “Wear your mask! This is real.” | Female, age 60-70, Hockley Co., Interviewed November 2020 | ||
| COVID-19 Vaccine | “Just hope they find a vaccine soon.” | Female, age 60-70, Lubbock Co., Interviewed November 2020 | |
| “I would pray that everyone who can - get the vaccine.” | Female, age 80-90, Lubbock Co., Interviewed December 2020 | ||
| “I would be hesitant to take the vaccine right now.” | Male, age 80-90, Lubbock Co., Interviewed November 2020 | ||
| “I think they aren’t distributing the vaccine fast enough or else we are not the information needed to go get the vaccine.” | Female, age 80-90, Lubbock Co., Interviewed January 2021 |
Table 2: COVID-19-related indicators for the total sample and by Lubbock County subsample vs. 4-rural counties subsample.
Results
Before analysis was conducted, county-level data were downloaded as Excel spreadsheets from the DSHS website, and line graphs were drawn to illustrate trends in:
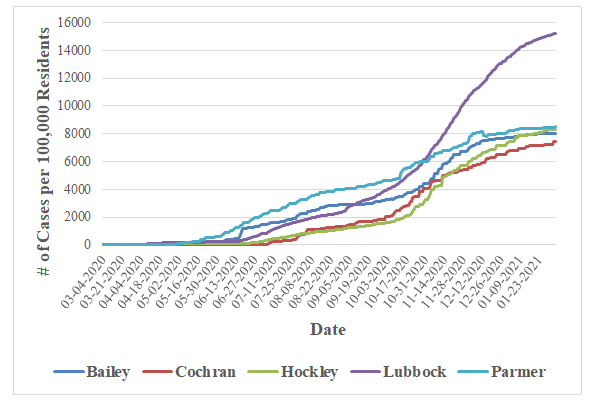
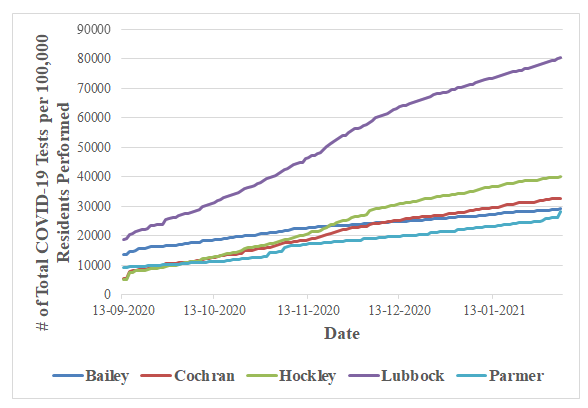
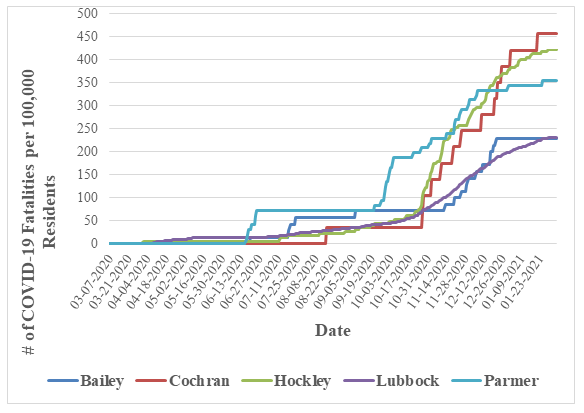
Cumulative COVID-19 cases per 100,000 residents (Figure 2), Cumulative COVID-19 tests performed per 100,000 residents (Figure 3), and Cumulative COVID-19 fatalities per 100,000 residents (Figure 4) across the five selected counties of interest.
County-Level Data of COVID-19 Cases, Testing, and Fatality
As shown in Figure 2, the number of COVID-19 cases per 100,000 residents increased the most for Lubbock County residents, most notably around October 2020 into January 2021. The number of COVID-19 cases per 100,000 residents decreased among rural county residents but was less than the overall cases of Lubbock County residents. In January 2021, the COVID-19 cases for rural counties averaged around 8,000 (per 100,000 residents) while for Lubbock County residents averaged around 15,000 (per 100,000 residents) cases. Figure 3 depicts total number of COVID-19 tests per 100,000 residents. As shown in Figure 3, in January 2021, the number of COVID-19 tests administered was around 80,000 (per 100,000 residents) for Lubbock residents and averaged around 20,000 to 40,0000 (per 100,000 residents) for rural county residents. Parmer and Bailey residents were the least likely to be tested for COVID-19 (30,000 total COVID-19 tests per 100,000 residents) and Hockley residents were the most likely among rural counties to receive the COVID-19 test (40,000 total COVID-19 tests per 100,000 residents). Figure
4 depicts the total number of COVID-19 fatalities per 100,000 residents. In January 2021, as shown in Figure 4, Lubbock and Bailey had the lowest number of fatalities (~200 per 100,000 residents), while rural counties Parmer (350 per 100,000 residents), Hockley (~400 per 100,000 residents), and Cochran (~450 per 100,000 residents) had the highest number of fatalities.
Health Behaviors and COVID-19 Experiences
A little over a quarter of participants (n = 79, 26.07%) were previous smokers, while 21 participants (6.93%) reported being current smokers. A majority of participants (n = 196, 64.68%) had never smoked. Only one participant (0.33%) reported currently vaping or using tobacco products, while two participants (0.66%) reported vaping or using tobacco products in the past.
Participants reported on their history of COVID-19 testing, symptoms, and preventative behaviors. At the time surveyed, a total of 230 participants (75.90%) reported not having been tested for COVID-19 (75.91%), while 73 had been tested (24.09%) for COVID-19 (see Table 2). Among those tested, 31 were diagnosed with COVID-19 (42.47%), while 38 (52.05%) were negative for COVID-19, and 4 participants were awaiting results. The majority of participants (n=299; 98.70%) diagnosed with COVID-19 reported symptoms that lasted for 10-14 days, with the exception of 4 people (1.30%) for whom the symptoms lasted for a month or longer. Among those reporting diagnosed cases of COVID-19 among household members, the majority (n=290; 95.71%) of household members’ symptoms lasted for about 2 weeks. However, at the time surveyed, only 13 participants (4.36% of the total sample) to their knowledge had come in direct contact in the past 24 hours with a person who had recently tested positive for COVID-19. Lubbock participants reported having been tested (n=54; 38.30%) and testing positive (n=23; 42.59%) for COVID-19 more often than the combined counties subsample (testing: n=19; 11.73%; p <.001) suggesting greater access to testing in Lubbock (Table 2).
When participants (overall sample) were asked if they experienced any of the following symptoms in the past 7 days: a significant number of people did not experience any fever (n = 301, 99.34%), dry cough (n = 285, 94.06%), shortness of breath (n = 286, 94.39%), decreased smell/taste (n = 293, 96.70%), nausea or vomiting (n = 299, 98.68%), sore throat (n = 294, 97.03%), muscle or joint aches (n = 279, 92.08%), or diarrhea/gastrointestinal problems (n = 294, 97.03%). Several participants (n = 7, 16.28%), experienced other symptoms not listed, including headache, arthritis, lack of energy, and tiredness. No differences were reported between Lubbock and rural counties subsamples (p >.05). Only 28 participants (18.67%) visited a doctor, nurse, or health care professional in-person to take care of their symptoms. Moreover, 15 participants (10.34%) called a doctor, nurse, or health care professional to take care of some of their symptoms. Lastly, only 3 participants (2.05%) had been referred to tele Health medicine.
Overall, the total sample of participants from both Lubbock and rural counties tested for COVID-19 at a low rate. However, Lubbock participants were more likely to have been tested and tested positive for COVID-19 than participants from rural counties. No differences were found among the symptoms of COVID-19 between participants from the Lubbock and rural counties.
Anxiety and Depression
Total Sample
In the total samples, 15 (5.05%) felt nervous, anxious, or on edge several days in the past 7 days, only 3 participants (1.01%) reported these feelings more than half the days, and only 3 participants (1.01%) experienced these feelings nearly every day. When asked about the frequency with which they felt depressed, 11 participants (3.74%) reported these feelings more than half of the day, while 3 participants (1.02%) felt depressed nearly every day.
Rural Sample
Among rural county residents, 7 (4.40%) felt nervous, anxious, or on edge several days in the past 7 days, only 3 participants (1.89%) reported these feelings more than half the days, and only 2 participants (1.26%) experienced these feelings nearly every day. When asked about the frequency with which they felt depressed, 5 participants (3.16%) reported feelings for several days, only 2 participants (1.27%) reported these feelings more than half of the days, while 2 participants (1.27%) felt depressed nearly every day.
Urban Sample
Among urban county residents, 8 (5.80%) felt nervous, anxious, or on edge several days in the past 7 days, no participants reported these feelings more than half the days, and only 1 participant (0.72%) experienced these feelings nearly every day. When asked about the frequency with which they felt depressed, 6 participants (4.41%) reported feelings several days, only 2 participants (1.27%) reported these feelings more than half of the days, while 2 participants (1.27%) felt depressed nearly every day. Overall, a small number of participants from the total sample experienced anxiety and depression. No significant differences were found between the rural and urban samples for anxiety and depression.
COVID-19 Vaccination and Perception
COVID-19 Vaccination Rates
In the total sample, 228 (77.55%) had received the flu vaccine for the year 2019/2020. Participants enrolled in Lubbock reported having received the flu vaccine more often (n = 120, 87.59%) than the combined rural counties subsample (n = 108, 68.79%) (See Table 2). The vast majority of overall participants took the recommended safety precautions against COVID-19 as advised by the CDC guidelines [8]: maintaining hand hygiene (n = 295, 97.68%), wearing masks in public (n = 291, 96.04%), social distancing (6 ft apart) (n = 291, 96.68%), and staying home and limiting outdoor activities (n = 285, 94.06%). No differences were noted between urban and rural subsamples (p >.10).
Qualitative Perceptions Towards Preventative Behaviors
As shown in Table 3, the thematic analysis revealed themes that were consistent with participants expressing personal responsibility in following safety recommendations put forth by the CDC as ways to keep themselves and their communities safe. They expressed frustration at others for not following safety precautions, one participant stated, “young individuals are perpetrators of COVID-19 spread.” Divergent opinions regarding mask wearing arose, with one participant quoting that masks worsen health outcomes.
Qualitative Perceptions Towards the COVID-19 Vaccine
Participants’ viewpoints regarding whether they would receive the vaccine were mixed-some quoting they would receive it, others feeling more hesitant. One individual felt that information about the vaccine was not adequately distributed. However, this appeared to be the minority experience.
Qualitative Responses on COVID-19 Challenges
Participants frequently mentioned feeling social isolation regarding COVID-19, missing the activities they could do before the pandemic, physical contact with others, and wanting the pandemic to end. Overall, the majority of participants received the flu, however, Lubbock County dwellers were more likely to receive the flu than rural county dwellers. Most participants followed CDC guidelines, with no differences between the Lubbock and rural subsample. Also, most participants felt isolated as a result of the pandemic distancing requirements and a small number demonstrated vaccination/mask hesitancy.
Discussion
This is the first study to explore urban-rural differences in COVID-19 experiences, including mental health, among residents of the South Plains Texas region. The urban subsample was derived from Lubbock County (population 310,569). The rural population is represented by four rural counties: Bailey County (population 7,000), Cochran County (population 2,853), Hockley County (population 23,021), and Parmer County (population 9,605). Among our sample of 303 adult participants, we found nearly a quarter of participants tested for COVID-19 in 2019/2020. Among those tested, approximately 42% tested positive for COVID-19. Surprisingly, the results indicated that most individuals in rural and Lubbock took precautions to prevent the COVID-19 pandemic but testing for COVID-19 was significantly higher in Lubbock compared to rural areas in rural West Texas. This may be due to the expansive measures taken by the City of Lubbock Health Department (CLHD) to distribute large vaccines early during the pandemic with an average of 3,000 people a day [21]. The campaign partnered with Citibus, the city’s public transportation, to provide commuters with free transportation to the CLHD. However, given this campaign was being disseminated in Lubbock, these results indicate a possible barrier to testing for persons in rural Texas during the COVID-19 pandemic.
There were quite a few similarities between participants from rural and Lubbock County regarding adherence to safety precautions (e.g., mask-wearing, social distancing). These results were surprising as past research [22] has indicated that persons in rural areas were less likely to adhere to safety precautions during the COVID-19 pandemic. This could be due to the majority of the sample being older and at higher risk for testing positive for COVID-19 and fearful of negative outcomes affecting older adults at a higher rate following a COVID-19 diagnosis. Also, most of the participants, even in rural areas (over 85%) reported they had at least a high school education indicating the sample might be more educated and, therefore, follow CDC guidelines and have the ability to identify misinformation. Further, even though individuals in both Lubbock, Texas and the rural counties endorsed adhering to safety precautions, they endorsed frustrations with being/feeling socially isolated from others, concerns about safety precautions (e.g., pro- and anti- mask wearing sentiments; believing the mask spreads bacteria), vaccine distribution (i.e., several participants were anxiously awaiting the vaccine), and access to COVID-19 information about the vaccine. However, these concerns and feelings of isolation by the majority of participants did not appear to lead to mental health symptoms in this sample.
Even though there were similarities regarding adherence to safety precautions and mental health symptoms there were some differences between urban and rural county residents as participants from rural Texas were likely less likely to have received a flu vaccine-a preventive measure to protect against the severe effects of the COVID-19 illness. The divergent experiences between residents of the Lubbock County and rural subsample are likely due to the following:
- Greater access to healthcare among the urban sample compared to the surrounding rural areas,
- Larger community spread of COVID-19 in the urban sample given the population density, and
- Higher reported health insurance in the urban sample compared to residents in surrounding rural counties.
The results therefore suggest greater access to testing, care, and treatment in the urban versus rural sample. County-level data also confirmed differential access to health care and treatment as Lubbock County led testing, incidence, and fatalities of COVID-19 compared to rural areas. Lubbock County residents, despite having the highest rate of COVID-19 cases, had the greatest number of residents tested for COVID-19, and the lowest fatality rates. On the contrary, rural residents had the lowest number of COVID-19 cases, the lowest number of residents tested for COVID-19, and the highest COVID-19 fatalities.
This research highlights disparities in COVID-19 experiences among urban and rural communities in access to testing. Our findings coincide with robust findings that have detailed differential COVID-19 trends in urban and rural areas [3, 23, 24]. Altogether, these findings call for the need to better address healthcare access in rural areas through telemedicine and other innovative approaches. One of the ways prior studies improved access to accurate health information is through tailored health communication approaches [25], which enhance information appraisal, increase motivation to process information, and promote behavioral change. One of the more accessible ways to implement tailored health communication strategies is by working with local health professionals in rural communities, like primary care providers and nurse practitioners, who can then disseminate pivotal and reliable information about local health departments [26].
Limitations
We acknowledge the potential for selection bias and/ or sample bias due to our different recruitment strategies in Lubbock, Texas, and the surrounding rural communities. Participant recruitment in the rural counties took place previously within the context of Project FRONTIER, an epidemiological study initiated in 2006 to investigate cognitive decline and associated risk factors longitudinally among a multi-ethnic sample of adults in rural West Texas. Recruitment efforts for the project included distributing flyers, providing community presentations (in English and Spanish), mailouts, and door-to-door solicitation with the purpose of recruiting a multi-ethnic (Hispanic/Latino and non-Hispanic/Latino) sample aged 40 and above. Conversely, in Lubbock, TX we relied on a convenience sample of older adult participants. Recruitment efforts for this program include posting announcements at TTUHSC, advertisements in the Golden Gazette (a local free monthly newspaper targeting older adults), and reminder postcards. Lubbock, TX study participants also included older adults who participated in the Retired and Senior Volunteer Program. Recruitment strategies and program activities are conducted solely in English. Thus, the Lubbock County subsample tended to be older and racially homogenous (predominantly White, non-Hispanic, or Latino) as compared to the rural counties subsample. As a result, future studies should attempt to create equal demographic distributions between both urban and rural samples.
Conclusion
This study is the first to explore the COVID-19 experiences between urban and rural communities living in West Texas. Our findings detail the differential COVID-19 trends of urban and rural areas in access to testing [25]. Altogether, these findings call for the need to better address healthcare access in rural areas through telemedicine and other innovative approaches. The COVID-19 pandemic has had far-reaching impacts on the lives of individuals around the world, especially older adults in the South Plains Texas region. Future work should seek to pinpoint the COVID-19 risk factors that increase one’s susceptibility to worse health outcomes and lingering symptomology. It will be important, as the COVID-19 pandemic continues and future pandemics are likely, to learn about vaccine uptake, acceptance, hesitance, as well as short- and long-term side effects of the vaccine in urban and rural populations. While there has been an increasing awareness of rural health disparities in the past several years, the same challenges that were elucidated in the 20th century still remain prevalent today [9]. We urge researchers to not only identify public health concerns but to begin developing public health solutions and monitoring health changes, especially to decrease the rural disparities regarding unequal access to healthcare. Solutions should focus on including community members in health promotion and partnering with organizations as health partners to ensure the accurate spread of information, and work with dwellers that face transportation and digital hurdles, to increase the scope of care.
Statement Regarding Research Ethics and Patient Consent
Written informed consent was obtained from all participants prior to enrollment. Individuals who were not deemed to be cognitively functional were excluded from the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgements
We would like to thank our data collectors (Veronica Lopez, Susan Thompson, and Cordelia Aguirre) and Project FRONTIER participants for their involvement in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Garrison Institute on Aging, which is supported by TTUHSC institutional funds and the Garrison Family Foundation.
Research Ethics and Patient Consent
Written informed consent was obtained from all participants prior to enrollment. Individuals who were not deemed to be cognitively functional were excluded from the study.
Research Data
Data are available from the Project FRONTIER (https:// www.ttuhsc.edu/centers-institutes/garrison-aging/project- frontier.aspx) for researchers who meet the criteria for access to de-identified Project FRONTIER data.
References
-
WHO (2022) Weekly epidemiological update on COVID-19.
-
Bureau UC (2020) One in Five Americans Live in Rural Areas.
-
CDC (2020) COVID-19 Stats: COVID-19 Incidence, by Urban-Rural Classification-United States.
-
Barbier BE, Hochard JP (2014) Poverty and the Spatial Distribution of Rural.
-
CDC (2020) COVID-19 Archived Webpage. Cent Dis Control Prev.
-
CDC (2020) Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)-United States.
-
Grome HN, Raman R, Katz BD, Fill MM, Jones TF, et al. (2022) Disparities in COVID-19 Mortality Rates: Implications for Rural Health Policy and Preparedness. J Public Health Manag Pract 28(5): 478-485.
-
Probst JC, Crouch EL, Eberth JM (2021) COVID-19 risk mitigation behaviors among rural and urban community- dwelling older adults in summer, 2020. J Rural Health 37(3): 473-478.
-
Ziller E, Milkowski C (2020) A Century Later: Rural Public Health’s Enduring Challenges and Opportunities. Am J Public Health 110: 1678-1686.
-
Alcendor DJ (2021) Targeting COVID Vaccine Hesitancy in Rural Communities in Tennessee: Implications for Extending the COVID-19 Pandemic in the South. Vaccines 9: 1279.
-
Peters DJ (2020) Community Susceptibility and Resiliency to COVID‐19 Across the Rural‐Urban Continuum in the United States. J Rural Health 36: 446- 456.
-
Murthy BP, Sterrett N, Weller D, Zell E, Reynolds L, et al. (2021) Disparities in COVID-19 Vaccination Coverage Between Urban and Rural Counties-United States, December 14, 2020–April 10, 2021. MMWR Morb Mortal Wkly Rep 70(20): 759-764.
-
WHO (2022) The Americas has a shortfall of 600,000 health professionals, affecting access to health in rural and underserved areas - PAHO/WHO | Pan American Health Organization.
-
Wang Y, Kala MP, Jafar TH (2020) Factors associated with psychological distress during the coronavirus disease 2019 (COVID-19) pandemic on the predominantly general population: A systematic review and meta- analysis. Plos One 15: e0244630.
-
CDC (2016) CDC Newsroom.
-
Matthews KA, Croft JB, Liu Y, Lu H, Kanny D, et al. (2017) Health-Related Behaviors by Urban-Rural County Classification-United States, 2013. MMWR Surveill Summ 66: 1-8.
-
Chen X, Chen H (2020) Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int J Environ Res Public Health 17: 4437.
-
Lee JJ, Kang KA, Wang MP, Zhao SZ, Wong JYH, et al. (2020) Associations Between COVID-19 Misinformation Exposure and Belief With COVID-19 Knowledge and Preventive Behaviors: Cross-Sectional Online Study. J Med Internet Res 22(11): e22205.
-
USDA (2019) USDA ERS-What is Rural?.
-
Texas COVID-19 data.
-
CDC (2021) Lubbock, Texas and Citibus Mobilize to Vaccinate Minority Communities.
-
Callaghan T, Lueck JA, Trujillo KL, Ferdinand AO (2021) Rural and Urban Differences in COVID-19 Prevention Behaviors. J Rural Health 37(2): 287-295.
-
CDC (2020) Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19)-United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep 69(12): 343-346.
-
Mueller JT, McConnell K, Burow PB, Pofahl K, Merdjanoff AA, (2021) Impacts of the COVID-19 pandemic on rural America. Proc Natl Acad Sci 118: 2019378118.
-
Rimer BK, Kreuter MW (2006) Advancing Tailored Health Communication: A Persuasion and Message Effects Perspective. J Commun 56(S1): S184-S201.
-
Everett CM, Schumacher JR, Wright A, Smith MA (2009) Physician Assistants and Nurse Practitioners as a Usual Source of Care. J Rural Health 25(4): 407-414.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria