Paradigm Shift in Protective Barrier Covering Implements for the Endemic Phase of Corona Virus and Routine Airborne Pollutants: The Game Changer Approach - Phase Three Category
This article presented a possible protective solution to the diverse health problems associated with human beings inhaling routine anthropogenic airborne particulates and micro-organisms by introducing some regular user friendly barrier covering implements i.e. narrows it down to zero pollutant inhaled for each person’s health care protection via the introduction of cosmetic-style barrier coverings, for the individual sense organs (i.e. nose-mouth-eye). Comprehensively, the atmosphere air is a mixture of several gases, consisting of three main components (78% nitrogen, 21% oxygen, and 1% argon), water vapor, trace gases such as the noble gases (neon, helium, krypton, and xenon); greenhouse gases (carbon dioxide, methane, nitrous oxide, and ozone); and the other gases such as hydrogen, iodine, carbon monoxide, ammonia, nitrogen dioxide, and sulfur dioxide, etc.
Introduction
Earth’s atmosphere can be divided (called atmospheric stratification) into five main layers: troposphere, stratosphere, mesosphere, thermosphere, and exosphere (Figure 1). The altitudes of the five layers are as follows: • Troposphere: 0 to 12 km (0 to 7 miles) above sea level i.e. from Earth’s surface.
- Stratosphere: 12 to 50 km (7 to 31 miles) above sea level.
- Mesosphere: 50 to 80 km (31 to 50 miles) above sea level.
- Thermosphere: 80 to 700 km (50 to 440 miles) above sea level.
- Exosphere: 700 to 10,000 km (440 to 6,200 miles) above sea level. Essentially, the air composition, temperature, and atmospheric pressure vary with altitude. And within the atmosphere, air suitable for use in “photosynthesis” by terrestrial plants and breathing of terrestrial animals is found only in Earth’s “troposphere”.
![Figure 1: Depicts the atmospheric stratification, to emphasize that the air composition under investigation is within the troposphere only [1-3].](/fulltextimages/11046/fig_1.png)
Figure 2 shows the common modeling of dry air composition as a uniform gas with properties averaged from the individual ten listed components. Normal air, Figure 3 (as presented by different investigators), also contains a variable amount of water vapor (H2O), which on average is around 1% at sea level and 0.4% over the entire atmosphere. Water vapor accounts for roughly 0.25% of the atmosphere by mass. “The concentration of water vapor (a greenhouse gas) varies significantly from around 10 parts/million (PPM) by mole fraction in the coldest portions of the atmosphere to as much as 5% by mole fraction in hot, humid air masses, and concentrations of other atmospheric gases are typically quoted in terms of dry air (without water vapor)” and they include the “noble gases”, neon, helium, krypton, and xenon and some “greenhouse gases”, methane, nitrous oxide, and ozone.
In general, nitrogen (N2 = 78.084%), oxygen (O2 = 20.9476%) and argon (Ar = 0.934%) are the three main components of the atmosphere. The trace gases includes the noble gases neon (Ne = 0.001818%), helium (He = 0.000524%), krypton (Kr = 0.000114%), and xenon (Xe = 0.0000087%), as well as some greenhouse gases carbon dioxide (CO2 = 0.04%), methane (CH4 = 0.0002%), nitrous oxide {N2O - 0.5 parts/million (PPM)} and ozone {O3 = 0.000007% i.e. 0 to 0.07 parts/million (PPM)} and the other gases such as hydrogen (H2 = 0.00005%), Iodine {I2 = 0.000001% i.e. 0.01 parts/million (PPM)}, Carbon monoxide {CO - 0 to trace (PPM)}, ammonia {NH3 - 0 to trace (PPM)}, nitrogen dioxide {NO2 =
0.000002% i.e. 0.02 parts/million (PPM)}, and sulfur dioxide - SO2 - 1.0 parts/million (PPM). Usually, the composition of air varies from one place to the next and even varies depending on whether it is day or night. Similarly, air pollution varies according to geographical location and also where it occurs in the air column. Pollutants include chemicals and industrial pollutants such as chlorine and its compounds, fluorine and its compounds, elemental mercury vapor, sulfur dioxide, and hydrogen sulfide. Other components of the atmosphere include spores, particulates like dust and ash (e.g. volcanic ash), and biological matter, like pollen and bacteria and salt from sea spray.
![Figure 2: Dry air composition averaged from the individual ten listed components [1,4,5].](/fulltextimages/11046/fig_2.png)
![Figure 3: Normal air composition that includes water vapor and pollutants which varies from one place to the next [6-9].](/fulltextimages/11046/fig_3.png)
Basically, the atmosphere (troposphere region) gets supplied every minute with more natural or anthropogenic (caused by human) particles or particulates {also known as atmospheric aerosol particles, atmospheric particulate matter, particulate matter (PM) or suspended particulate matter (SPM)}, a mixture of solid particles and liquid droplets. Some particles, such as dust, dirt, soot, or smoke, are large or dark enough to be seen with the naked eye. Others are so small they can only be detected using an electron microscope. Usually, particulate matter (PM) refers to inhalable particles, composed of sulphate, nitrates, ammonia, sodium chloride, black carbon, mineral dust or water, etc. which can be of different size and is generally defined by their aerodynamic diameter, with PM2.5 and PM10 (a.k.a. coarse particles) as the most common two categories in the regulatory framework and relevant for health. Precisely:
- PM10 :- are inhalable particles, with diameters that are generally 10 micrometers (μm) and smaller (i.e. 10000 nm or less); and
- PM2.5:- are fine inhalable particles, with diameters that are generally 2.5 micrometers (μm) and smaller (2500 nm or less).
Furthermore the PM2.5, category can be distinguished between fine particles, with a diameter of 2.5 μm or less (i.e. 2500 nm or less); and ultrafine particles (UFP), with a diameter of 100 nm or less (less than or equal to 0.1 micrometer); and “soot” (consists of agglomerated nanoparticles with diameters between 6 and 30 nm). Soot form during incomplete combustion from precursor molecules {such as hydrocarbons- acetylene, naphthalenes, benzenes, aliphatics (alkanes, alkenes and alkynes); local field burning, house fires, cooking, oil lamps, candles, etc.) and it is a powder-like form of “amorphous carbon”. Gas-phase soot contains polycyclic aromatic hydrocarbons (PAHs) also known as “mutagens” and are classified as a “known human carcinogen” by the International Agency for Research on Cancer (IARC)[10].
The term “aerosol” commonly refers to the particulate/ air “mixture”, as opposed to the particulate matter alone. Research studies in the 1960s and 1970s distinguished between coarse particles (sometimes called droplets) and fine particles (sometimes called aerosols). According to aerosol science, whenever liquid hangs in air it is technically an aerosol, but other disciplines use the word “droplet” to mean a coarse particle five micrometers or larger (5– 100 μm), and reserve “aerosol” for fine particles smaller than five micrometers in effective diameter (<5 μm).
A micron is a metric unit of measurement where one micron is equivalent to one one-thousandth of a millimeter [1 micron (1μ) = 1/1000 mm] or 1 micron (micrometer) = 1/1,000,000 of a meter.
- one micron is one-millionth of a meter
- 1 micron = 10-6 m (i.e. 1 microns unit number 1.00 refers to 1 µm, one micrometer)
- 1 micron = 1000 nano meter (i.e.1000nm) Figure 4 shows the size comparisons of PM particles with single hair from the human head, revealing that the average human hair of about 70 micrometers in diameter is 30 times larger than the largest fine particle of 2.5 micrometers in diameter. While Figures 5 & 6 shows the size chart in microns of very few sources (about 40) of the most common particles (contaminants-well over 100 sources) that are around us all the time. There are 25,400 microns in one inch, while the eye of a needle is 1,230 microns. This dot (.) is approximately 1/64 of an inch wide and equals 615 microns [11, 12, 13].
![Figure 4: Size comparisons of PM particles with average human hair (Comparison of nanomaterials sizes) [14,15].](/fulltextimages/11046/fig_4.png)
![Figure 5: Shows types and size distribution in micrometers (μm), of atmospheric particulate matter and differentiates between particles that are visible to the naked eye, visible with a microscope and those that are visible with an electron microscope [16].](/fulltextimages/11046/fig_5.png)
![Figure 6: Names and sizes of some common airborne particles [17].](/fulltextimages/11046/fig_6.png)
Essential background hints- building blocks for this investigation:
- Approximately 98-99% of all particles by count are in the size range of 5 microns or less.
- The majority of harmful particles are 3 microns or less in size.
- The average person breathes in about 16,000 quarts of air per day. Each quart contains some 70,000 visible and invisible particles. That’s over a billion particles per day that our lungs have to filter out!
- Visible particles constitute only about 10% of indoor air!
- Although in general the molecular size of viruses that have proven to be harmful or deadly to humans range between 0.005 to 0.3 microns (i.e. 5 to 300 nm), the average for coronary viruses in particular is about 0.125 microns i.e. 125 nm (though it varies between 0.06 micron and 0.14 micron in diameter i.e. 60 nm and 140 nm). Smaller viruses exist according to scientists, but whether they are a risk to mankind or not, have yet to be determined.
- Several different types of experimental measurements reported molecular size of oxygen O2 as 0.0005 microns (0.5 nm), CO2 0.00065 microns (0.65 nm) and stated that O2 has a slightly smaller diameter than N2 {the difference is size between O2 and N2 is very small, only about 0.3 times 10 to the -10th meters (0.00000000003 meters)}. This means the size of oxygen molecule is 250 times smaller than Corona virus.
- A N95 mask has pore size of 0.1 micron (100 nm). Pore size also varies up to 300 nm. A mask with pore size of 100 nm or 0.1 micron can easily allow oxygen molecules (0.5 nm or 0.0005 microns) and other gases (e.g. CO2 0.00065 microns or 0.65 nm and N2) but not particulate matters {fine particles that has the size of less than 2.5 micrometer/microns (0.00025 cm) i.e. 2500 nm or less} and corona virus (0.125 microns or 125 nm) as well. This simply means that molecule of oxygen, nitrogen and carbon dioxide, will freely get through the mask to enable the body receive the oxygen it needs.
- Viruses are never naked in air or on any dry surface. They are contained in water based droplets (of size larger than 1 micron i.e. 1000 nm). Such droplets are actively filtered by masks. Simply put when we cough or sneeze, viral particles are contained in fluid droplets, and it’s the droplets that make it possible to trap the virus i.e. the droplets make it possible for masks to have some effect, never 100%.
- When fine particles successful pass through your nostril and enter your lung, it will be deposit on the alveoli and causing long term effect. Some individual who have constant exposure without protection can even suffer from cardiac pulmonary disease causing sudden lung and health failure. Different areas may have different sizes of fine particle sizes.
- A good grade N95 mask can filter fine particles efficiently.
- Literally, the term endemic simply connotes that it is a constant presence/prevalent in a particular area of the world or in a particular population, hence it could be applicable to pollutant, virus or bacteria. On the other hand, a pandemic is a surge in cases of a particular illness that has spread to multiple parts of the world, while, an epidemic is a surge in cases that are confined to a smaller area, such as “food-borne” illness outbreak in a few states or the “2014 Ebola outbreak”.
- Practically speaking, many experts now see COVID-19 becoming endemic in a way that’s similar to the seasonal flu pattern such as influenza or cold viruses, and respiratory syncytial virus (RSV), (Figure 7). That is, “its endemic when it doesn’t disrupt everyday life,” i.e. doesn’t disrupt health care, transportation, businesses or our other usual routines. Living with COVID-19 means that, we may have more surges (possibly fueled by new corona-virus variants) occasionally, maybe, for the next several years. But those waves likely won’t be as disruptive as the delta and omicron surges have been due to the increasing overall level of immunity- both from vaccination and infection (i.e. proportion of the population that has some level of immunity will be higher and higher).
![Figure 7: Structure of RSV (respiratory syncytial virus) [18].](/fulltextimages/11046/fig_7.png)
According to Azzari C [19], “each year, it is estimated that more than 177,000 older adults are hospitalized and 14,000 of them die in the United States due to RSV. The disease burden of RSV in children is also staggering. Globally, there are an estimated 33 million cases of RSV annually in children less than 5 years of age, with about 3 million hospitalized and up to approximately 120,000 dying each year from complications associated with the infection.” RSV and COVID-19 are both respiratory infections and share many similar symptoms. Both conditions can cause fever, cough, runny nose, and sneezing. Upset stomach, vomiting, or diarrhea may also occur in babies with COVID-19 [20].
Currently (as of April 2023), no licensed vaccine against RSV exists (i.e. there is no cure or vaccine for RSV), hence the medical world has been limited to offering only supportive care, such as oxygen and fluids, for those with the illness. Very recently, an advisory panel to the U.S. Food and Drug Administration (FDA) recommended RSV vaccines from Pfizer and GSK [21].
Furthermore, on July 17, 2023 the FDA approved a monoclonal antibody injection to help prevent RSV for children up to age 2. Unlike a vaccine that prompts the body to make its own antibodies, the injection works by delivering antibodies against RSV directly into the bloodstream. Figure 8 shows the image sizes illustrative that compares the corona virus, relative to other small molecules like, influenza, a red blood cell, PM2.5 particle and size of particles filtered by masks.
![Figure 8: Compares the sizes of particles filtered by facemasks (with holes: 0.007 μm) and Corona virus size (0.1 μm) [22].](/fulltextimages/11046/fig_8.png)
Sources of Air Pollutants-airborne contaminants. Figure 8: Compares the sizes of particles filtered by facemasks (with holes: 0.007 μm) and Corona virus size (0.1 μm) [22].
Sources of Air Pollutants-Airborne Contaminants: Some particulates occur naturally, originating from volcanoes, dust, storms, forest and grassland fires (wildfires), living vegetation and sea spray. And human activities also generate significant amounts of particulates. These particles come in many sizes and shapes and can be made up of hundreds of different chemicals. Some are emitted directly from a source, such as construction sites activity, unpaved roads, fields, smokestacks or fires (smoke released from fireplaces, wood stoves and outdoor burning), sea spray and natural wind-blown dust from erosion. But most particles form in the atmosphere as a result of complex reactions of chemicals such as sulfur dioxide and nitrogen oxides, which are pollutants emitted from power plants; industries/ factories (i.e. Steel and cement production); automobiles (i.e. transportation sector- vehicles/cars/trucks, boats/ ships, trains, airplanes); animals and agricultural spaces, pollen and more. For example, “Burning of fossil fuels in (e.g., aircrafts, motor vehicles especially diesel engines), and biomass (e.g. wood), construction (activities of building refurbishment or demolition), road-works, using heavy equipments, emission from the production of building materials, metal-working (e.g., welding), wood-working, glass reprocessing, agricultural activities (e.g., ploughing and soil tilling), power plants, waste/trash incineration, road dust from tire and road wear, wet cooling towers in cooling systems, various industrial processes such as mining operations, smelting and oil refining, petroleum well sites and equipment, petrochemical and chemical plants, power electric plants, boilers or steam generators, process furnaces, coal processing units, disasters (both natural or caused by humans, e.g., earthquakes, wars), microplastics (gaining attention as a type of airborne PM), etc. Similarly, when human beings breathe, talk, eat, cough, sneeze or sing, particles are emitted across a range of sizes, both coarse and fine. Anthropogenic aerosols currently account for about 10
percent of the total mass of aerosols in the atmosphere.
Hence, particle pollution is produced by a wide variety of natural and manmade sources. This implies that both ambient (outdoor environments) and household (indoor) air pollution can come from similar processes such as incomplete combustion of fuels or chemical reactions between gases. However, the specific source of the combustion process can vary. For example, household activities such as boiling water for bathing or cooking or preparing animal fodder, space heating and water heating with dirty technologies, brewing beverages, and lighting with kerosene, emits a range of health harmful pollutants indoors (household air pollution exposures), while activities such as high temperature combustion in traffic and transportation (e.g. vehicles, aviation, shipping, etc.), industrial activities and power generating facilities, construction sites, waste burning, fires or fields, etc. contribute to ambient air pollution [23].
![Figure 9: Schematic of some anthropogenic (human sources) of PM e.g. transport smokes [24,25].](/fulltextimages/11046/fig_9.png)
Usually, the greatest source of particulate matter around the home is generally the combustion of polluting fuels (e.g. firewood and other biomass), while in the ambient; the finer particles are derived from primary sources (e.g., combustion of fuels in power generation facilities, industries or vehicles) and secondary sources (e.g., chemical reactions between gases). Soot in very low concentrations is capable of darkening surfaces or making particle agglomerates, such as those from ventilation systems, appear “black”. Soot is the primary cause of “ghosting”, the discoloration of walls, floors and ceilings as a result of some form of “pyrolysis” such as coal burning, internal-combustion engines, power-plant boilers, hog-fuel boilers, ship boilers, exhaust emissions from vehicles, central steam-heat boilers, waste incineration, local field burning, house fires, cooking, oil lamps, candles, forest fires, fireplaces, and furnaces [16]. Soot also tends to form in “chimneys” in domestic houses. If a large deposit collects, it can ignite and create a chimney fire. Regular cleaning by a chimney sweep should eliminate the problem.
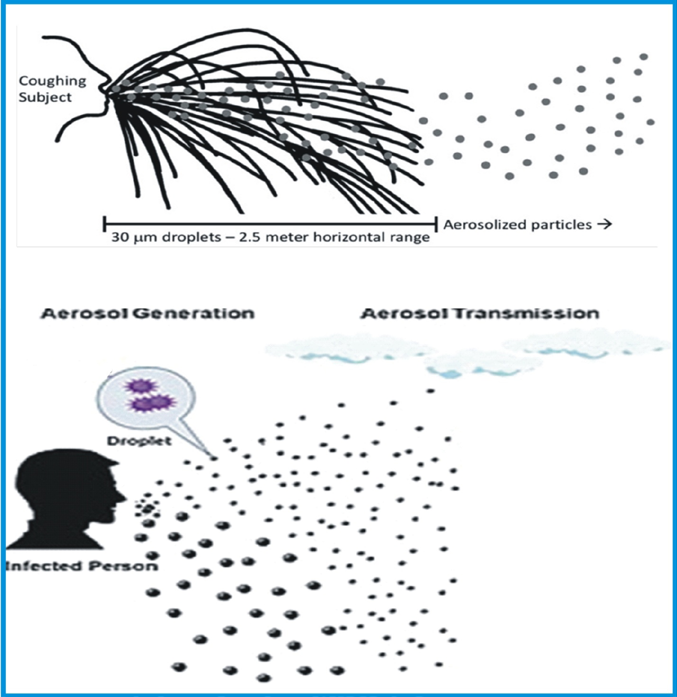
Figure 9, depicts some anthropogenic (human sources) of PM e.g. transportation and Figure 10 illustrates the coughing subject that produces respiratory particles of various sizes; larger droplets tend to follow a ballistic trajectory (black lines), whereas aerosolized particles (gray dots) become suspended in air to varying degrees, extending their range. Simply put, droplets are generally large, and gravity drags them down to land on objects, rather than staying in the air. So they don’t travel very long distances.
Health Hazards of Breathing Air Containing High Levels of Pollutants
Several research investigations globally revealed that urban air quality (a.k.a. ambient or outdoor) and indoor air pollution are two of the world’s worst toxic pollution problems. Precisely, they presumed that more than 99% of the global population lives in areas where the air pollution is above the World Health Organization (WHO) air quality guidelines. Specifically, (WHO), reported that 9 out of 10 people worldwide breathe air containing high levels of pollutants [26].
NOTE: The Air Quality Index (AQI) is an index for reporting daily air quality. It tells how clean or polluted your outdoor air is, and it focuses on health effects that may be experience within a few hours or days after breathing polluted air. Practically, the pollutants in the form of particulate matters (PM), smog, dust, carbon monoxide (CO), ozone (O3), nitrogen dioxide (NO2) and sulfur dioxide (SO2), etc. have the ability to penetrate deep into the lungs and brain from the blood streams, causing health problems. “The size of particles is directly linked to their potential for causing health problems. Fine particles (PM2.5) pose the greatest health risk. These fine particles can get deep into lungs and some may even get into the bloodstream. Soot, particularly diesel exhaust pollution, accounts for over one-quarter of the total hazardous pollution in the air. Exposure to these particles can affect a person’s lungs and heart. Coarse particles (between PM10 to PM2.5) are of less concern, although they can irritate a person’s eyes, nose, and throat [27]. In general, both long-term and short-term exposure to particulate matter is associated with morbidity and mortality from cardiovascular and respiratory diseases, while long-term exposure has been further linked to adverse perinatal outcomes and lung cancer. Overall, the associated health problems include respiratory effects such as irritation of the airways, coughing or difficulty breathing, aggravated asthma attacks and bronchitis, “heart disease” {e.g. cardiovascular effects such as cardiac arrhythmias and heart attacks (ischaemic heart disease, nonfatal heart attacks, irregular heartbeat), cerebrovascular (stroke)}, “lung disease” (decreased lung function), and “premature death” in people with heart or lung disease [28, 29]. WHO estimated that 7 million premature deaths annually are linked to air pollution, with most deaths in developing countries [26], while researcher in Catalonia concluded that the mortality rate from air pollution is eight times larger than the mortality caused by car accidents each year and proclaimed that, on a local level, 3500 deaths a year are caused by air pollution in Catalonia [30]. Furthermore, other researchers stated that worldwide exposure to PM2.5 contributed to 4.1 million deaths from heart disease and stroke, lung cancer, chronic lung disease, and respiratory infections in 2016 and that, ambient particulate matter ranks as the sixth leading risk factor for premature death globally. Again in specific terms, (WHO) reported that, about 4.2 million deaths are attributed to ambient air pollution each year while 3.2 million people die prematurely from household air pollution every year [26], because around 2.4 billion people cook and heat their homes with polluting fuels (e.g. firewood and other biomass).
Furthermore, according to IAAC Blog [31], “In the UK, eliminating all anthropogenic PM2.5 (a practical impossibility) would increase life expectancy from birth by approximately six months, averaged across the whole population-roughly double the impact from elimination of all road accidents or passive smoking. Those with pre-existing respiratory conditions, as well as the young and elderly are at greater risk. PM mass concentrations in many nations are substantially higher than those in the UK, particularly in the developing world; burning wood, coal or biomass for domestic heating and cooking is a substantial source of personal exposure to PM in many such areas”.
NOTE: Hence, since human beings cannot stop breathing in air from the atmosphere and the supply of PM into the atmosphere cannot be stopped (because almost all the sources are fundamental necessary process engagements for human survival). The only feasible remedy is to wedge PM from the entrance point with an aesthetically designed barrier covering/mask (possibly with bio-cellulose, hydro- gel, nano-materials), that make it look natural instead of concealing face of the wearer as in the case of the present designs, etc. In general pollutants that are harmful to the human health fall into three major categories i.e. air, water, and soil pollution. Figure 11 depicts the human respiratory system through which air pollutants and contaminants basically access the human body.
![Figure 11: The human respiratory system through which air pollutants and contaminants basically access the human body [32,33].](/fulltextimages/11046/fig_11.png)
The respiratory system is the network of organs and tissues that help in breathe i.e. absorb oxygen from the air so human organs can work. It also cleans waste gases, such as carbon dioxide, from the blood. The airways (mouth and nose) pull air from outside and deliver air to the lungs, pharynx (throat) is the tube that delivers air from the mouth and nose to the trachea (windpipe) i.e. passage connecting the throat and lungs. Bronchial tubes are the tubes at the bottom of the windpipe that connect into each lung i.e. the two organs that remove oxygen from the air and pass it into the blood and the bloodstream delivers oxygen to all organs and other tissues (e.g. brain). Muscles (diaphragm) and bones help move the inhaled air into and out of the lungs i.e. pull in air and push it out [34, 35, 36, 37].
Figure 12 reflects that different sizes of pollutant have specific areas in the body, where they settle to harm the body. While Figure 13 further distinguished between the short term and long term effects as well as established that the problem cuts across all the ages.
![Figure 12: Show that different sizes of pollutant have specific areas in the body, where they settle to harm the body [32,33,38].](/fulltextimages/11046/fig_12.png)
![Figure 13: List of short term and long term effects as well as revealed that the problem cuts across all the ages [32,33,39].](/fulltextimages/11046/fig_13.png)
Figures 14 & 15 addressed the specific health issues associated with specific source of particular pollutant, such as exposure to asbestos, smog, coal power emissions, fine dusts, Viruses and bacteria, and soldering fumes, etc. For instance, figure 15b: The schematic description of how COVID-19 respiratory droplets enter the body by landing on the nose or mouth and entering through the lungs. Related symptoms include fever, cough, and dyspnoea.
![Figure 14: The health issues associated with exposure to asbestos, smog, coal power emissions, and fine dusts [32,33,40].](/fulltextimages/11046/fig_14.png)
![Figure 15: How COVID-19 droplets can enter the respiratory of the body and its effect [32,33,41,42].](/fulltextimages/11046/fig_15.png)
Existing Prevention and Control Measures to Avoid the Inhalation of Pollutants
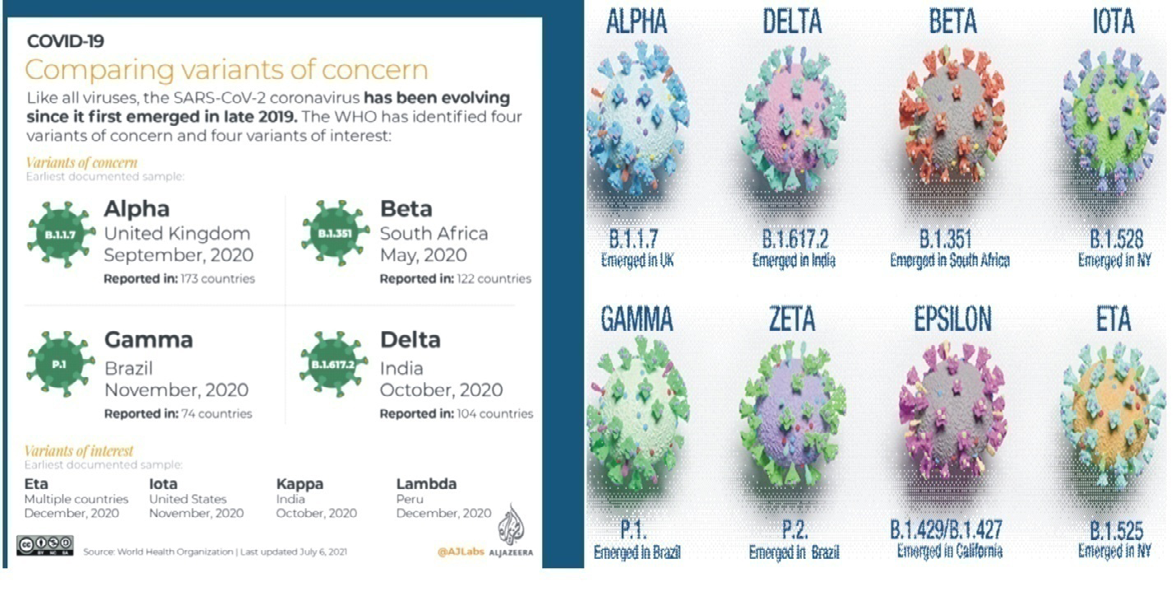
Presently, the principal public health method of preventing and controlling the hazardous effects of air- borne pollutants such as microorganisms (viruses e.g. SARS- CoV-2 and its different variants, Figure 16), particulate matters (PM), smog, soot (a.k.a. black carbon), dust, etc. are pharmaceutical interventions (particularly vaccination) and non-pharmaceutical interventions (include the use of face masks and other personal protective equipment-PPE, such as face shields, goggles, etc.).
One of the defining features that make a variant different from other variants is enhanced transmissibility. Also, epidemiological analysis, which looks at things like the distribution of infection and the severity of illness, can often provide rapid assessments of changes to virus characteristics [43]. Although experiment shows that the body gets the oxygen it needs, when breathing through a face mask/barrier covering. However, prolonged wearing of face masks and respirators can lead to numerous health issues, and other logistical, physiological, psychological, social and economic complications [44, 45, 46, 47, 48, 49].
Health Challenges and Discomfort Associated with Wearing Barrier Face Covering: Face Masks and Respirators
A barrier face covering, as described in American Society for Testing and Materials” (ASTM F3502-21), is a product worn on the face specifically covering at least the wearer’s nose and mouth, with the primary purpose of providing “source control” and to provide a degree of particulate filtration to reduce the amount of inhaled particulate material. By this simple definition, it incorporates the uses of both (surgical and non-surgical respirators) and (surgical and non-surgical face masks). Originally born out of the useful knowledge of protecting wounds from surgeons’ breath and predominantly bacterial droplet contamination, the mask is now a visibly popular everyday used item by the general public globally due to the COVID-19 pandemic. For the general public, one reason for wearing a facial covering is to help protect others from you when you cough, sneeze or even talk and spray viral droplets into the air. Usually, many people who become infected can unknowingly spread the COVID-19 virus because they have few or no symptoms (asymptomatic means having Covid-19 but not showing any symptoms at all).
Notably, “Masks, when used by the general public, are considered by scientists to pose a risk of infection because the standardized hygiene rules of hospitals cannot be followed by the general public. On top of that, mask wearers (surgical, N95, fabric masks) exhale relatively smaller particles (size 0.3 to 0.5 μm) than mask-less people and the louder speech under masks further amplifies/increased this fine aerosol production by the mask wearer (nebulizer effect)”.
Hence, “from an infection epidemiological point of view, masks in everyday use offer the risk of self-contamination by the wearer from both inside and outside, including via contaminated hands. In addition, masks are soaked by exhaled air, which potentially accumulates infectious agents from the nasopharynx and also from the ambient air on the outside and inside of the mask” (in particular, serious infection-causing bacteria, fungi and also viruses) [50, 51].
Conclusively therefore, although undoubtedly essential in protecting the health of staff and patients, as well as the general public, there are numerous logistical, physiological, psychological, social and economic complications associated with wearing the present designed/configured barrier face coverings. This includes
- The continued/repeated re-inhaling of some fractions of the wearer’s previously expelled breath, possibly contaminated with some fractions of the odor/gas from the mouth, in the confined space within the barrier face covering. Simply put, by prolonged use of particulate barrier face covering, the normal human airway breathing process is disrupted thereby inhaling excessive (re-breathing our own exhaled) carbon dioxide (CO2) instead of fresh oxygen, which may lead to a variety/different health issues.
- Uncomfortable eyes and variable vision due to mask associated dry eye (MADE) and foggy eyeglasses issues.
- Discomfort and irritation around the region of the nose and mouth, such as red marks.
- It makes breathing seem harder i.e. more difficult especially if the face masks are heavily contaminated.
- The quality and the volume of speech between two people wearing masks are considerably compromised and they may unconsciously come closer [52, 53, 54, 55].
Effects of carbon dioxide (CO2) re-breathing: According to the National Institutes of Health (NIH), inhaling high levels of carbon dioxide (CO2) may be pretty dangerous and life- threatening. Precisely, “it is dangerous in an atmosphere when it is greater than about 10%.” Based on their design and configuration, prolonged wearing of face masks and respirators can lead to CO2 re-breathe due to increased concentration of CO2 within the masks (i.e. carbon dioxide build up in the mask over time) beyond atmosphere normal level of between 300 and 700 PPM. A recent study measured the carbon dioxide concentration in the breathing zone while wearing a surgical mask, a KN95 and a cloth mask and the detected carbon dioxide concentrations ranged from 2150 ± 192 to 2875 ± 323 PPM. Medically, When CO2 levels are elevated in the body it is known as “hypercapnia (carbon dioxide toxicity), which can lead to increased blood pressure, headaches, muscle twitches, rapid heart rate, chest pain, confusion, and fatigue, vertigo, double vision, inability to concentrate, tinnitus (hearing a noise, like a ringing or buzzing, that’s not caused by an outside source), seizures, or suffocation due to displacement of air.” As well as increased respiratory rate, lassitude, sleepiness, convulsions, dyspnea. Figure 17 shows the signs and symptoms produced at specific larger gas-phase concentrations of CO2 e.g. headache, sweating, dizziness, or narcosis. In extreme cases, if left untreated, hypercapnia can lead to organ damage and even have long standing effects on the brain. Actually, there is a wide variation in the physiological response to exposures at certain CO2 by different individuals.
Carbon dioxide levels and potential health problems are indicated below:
- 250-350 PPM: background (normal) outdoor air level.
- 350-1,000 PPM: typical level found in occupied spaces with good air exchange
- 1,000-2,000 PPM: level associated with complaints of drowsiness and poor air
- 2,000-5,000 PPM: level associated with headaches, sleepiness, and stagnant, stale, stuffy air; poor concentration, loss of attention, increased heart rate and slight nausea may also be present.
- 5,000 PPM: This indicates unusual air conditions were high levels of other gases also could be present. Toxicity or oxygen deprivation could occur. This is the permissible exposure limit for daily workplace exposures.
![Figure 17: Signs and symptoms of carbon dioxide toxicity [52].](/fulltextimages/11046/fig_17.png)
Fundamentally, carbon dioxide is known as an asphyxiant, which is a substance that bonds with the blood in place of oxygen. Unlike most simple asphyxiants (which do not have any inherent toxicity of their own), CO2 poisoning have been linked to central nervous system damage and permanent deterioration of respiratory functions. Thus it is considered to be a gas with acute systemic respiratory effects. Basically, if the blood becomes saturated with too much CO2, it develop the condition known as hypercapnia, which affect the pH level of the blood, turning it more acidic. This condition is called acidemia and, if prolonged, causes acidosis, which is injury to the body’s cells by a rise in acidity that leads to faltering functions of the heart. Some possible outcomes of this interference with the heart include low blood pressure and cardiac arrhythmia (cardiovascular effects). These conditions are the result of temporary or permanent nerve damage brought on by acidemia (high acidity), and include delirium, hallucinations, seizures, respiratory failure, coma or death. Usually, as an asphyxiant, carbon dioxide displaces breathable oxygen and impairs pulmonary gas exchange. If
the oxygen content of the air a human breathe is insufficient, they slowly suffocate (asphyxiation) due to selective oxygen depletion until they experience permanent damage or death.
Uncomfortable Eyes Issues: Figure 18, illustrates the causes and solutions of mask associated dry eye (MADE). The main cause is due to the present configuration of particulate face masks which makes it to be loosely fitting and enables the exhaled air go into the eyes of the wearers. This continuous flow of the exhaled air over the eye generates tear from the eyes, which gradually dries the eye as well as develop fogs on eyeglasses. People with existing dry eye disease report worsening symptoms-a problematic occurrence for the tens of millions of people worldwide who already struggle with the issue. Note: Ab-initio, there are many causes of dry eye disease, including issues relating to eye and systemic health conditions, age, gender or medications. Excessive use of digital devices, poor indoor air quality and pollution all result in symptoms. Situations that increase how quickly the tear film evaporates, such as air-conditioned offices or automobile air-blowers, can quickly and significantly dry the eye’s surface, leading to more pronounced symptoms. Concurrently, previously asymptomatic patients are flagging uncomfortable eyes and variable vision for the first time, particularly when reading or using digital devices for a long period of time. Secondly the exhaled air that goes into the eyes generates an uncomfortable feeling and an impulse to touch the eyes. Thus, if wearers’ hands are contaminated, it leads to wearer infecting him-self or her-self.
![Figure 18: Causes and solutions of mask associated dry eye (MADE) [53].](/fulltextimages/11046/fig_18.png)
Thermo-Physiological Discomfort and Irritation
Most often the severity of thermo-physiological responses/effects of wearing barrier face covering such as feeling unfit, tight, itchy, fatigued, odorous and salty; microclimates and skin temperatures inside of the barrier face covering (such as heart rate and thermal stress , breath resistance) depends on whether the wearer is wearing face mask or N95 respirator. Usually, the overall perceptions of discomfort are significantly lower when wearing face mask than when wearing the N95 respirator.
On the contrary, in terms of perception of humidity, there is significantly higher absolute humidity outside the surface of face mask than outside the surface of N95 respirators, while in reverse; there is significantly lower absolute humidity inside the surface of face mask than inside the surface of N95 respirators. Notably, “Mandated face mask use for health care providers, secondary to COVID-19, creates an additional communication barrier for older adults with cognitive, communication, and/or hearing challenges. Face masks can soften a speaker’s voice, conceal vocal tone, and hide facial expressions that relay essential non-verbal information. An inability to understand health care information or words of support can lead to frustration, anxiety, and decreased quality of life” [54, 55].
Evolution of Mask
In general, “mask is a form of disguise or concealment usually worn over or in front of the face to hide the identity of a person and by its own features to establish another being. This essential characteristic of hiding and revealing personalities or moods is common to all masks. As cultural objects they have been used throughout the world in all periods since the Stone Age (about 30,000 BCE to 3,000 BCE) and have been as varied in appearance as in their use and symbolism.” It varies from the simplest of crude “false faces” held by a handle to complete head coverings designed with ingenious movable parts, made by selecting and combining available materials/substances such as woods, metals, shells, fibers, ivory, clay, horn, stone, feathers, leather, furs, paper, cloth, and corn husks. On the other hand, the “surface treatments have ranged from rugged simplicity to intricate carving and from gaudy adornments to polished woods and mosaics.” This includes carnival/masquerade masks/ dance masks, tribal masks, anonymous masks, pest control- pesticides spraying masks, athletic face mask (worn during sports and workouts), comedy and tragedy masks, maiden spirit masks, death masks, et cetera (Figure 19).
![Figure 19: Typical samples of the various types of masks used throughout the world [56-61].](/fulltextimages/11046/fig_19.png)
Evolution of the Surgical/Medical Mask
Plague has been a reoccurring feature in human life for centuries starting from the 6th century (named the Plague of Justinian after emperor Justinian 1). Again, in the Late Middle Ages (from the 5th to 16th century), Europe experienced the deadliest disease outbreak in history when the Black Death, the infamous pandemic of bubonic plague, hit in 1347, killing one-third of the European human population. Several other plagues resurfaced throughout the Renaissance (between the late 13th and the early 17th century), up-till in the mid-19th century i.e. in the second half of the 19th century (1800s) and from the early 20th century (1900s) to the influenza in 2009 (21st century), as well as the present COVID-19 (2019 to date) [62, 63, 64, 65, 66, 67].
![Figure 20: The first historical attempt used to keep physicians safe from contagion while treating plague victims using Beaked mask [62-67].](/fulltextimages/11046/fig_20.png)
Finding qualified physicians during the earlier plagues to treat victims were difficult, so unskilled “doctors” (often with no formal medical training) would volunteer to fulfill this role. These plague doctors were also known as ‘empirics’. Being a plague doctor was both unpleasant (constantly being surrounded by death) and risky (the plague was relatively easy to contract, and chances of survival were slim). “As an example of the risk involved in being a plague doctor, it is recorded that of eighteen plague doctors in Venice, only one was left by 1348, in the midst of the destruction of the plague.” Due to the risk of contracting the plague, these doctors had to shield/guard themselves in every possible way from infection i.e. from polluted air, by wearing a uniform of sorts, which included a beaked mask, (Figure 20) (i.e. usually, plague doctors wore a costume that consisted of a wide-brimmed hat, a waxed robe, and a wooden cane pointer with mask that had glass eye openings, two small slits under the nostrils, and a long, cone-shaped beak that sat in front of the plague doctor’s nose). “This beak would be filled with aromatics including amber, myrrh, dried rose and carnation petals, spices, herbs, straw, and sometimes even a sponge soaked in vinegar. The idea was that when the plague doctor inhaled, he would only inhale pleasant, clean air that was not noxious, and therefore unlikely to infect him with the plague.” Fundamentally therefore, the origin of surgical mask also referred to as medical mask could be traced to the use of beaked masks that plague doctors wore during the 17th- century (1600s) plague epidemic i.e. late Renaissance. “At the time, disease was believed to spread through miasmas (also commonly called bad air)-bad smells that wafted through the air. Thus another reason the beak was stuffed with herbs, spices and dried flowers, is to ward off the odors believed to spread the plague.” That is, the beak shape would allow enough time for the herbs to attack plague-filled air before doctors breathed it in [64, 65, 66].
Subsequently, the introduction of mouth and nose coverage (mouth protection, face veils, face masks, mouth bandages) for doctors use during surgical operations, can be followed back to the turn-of-the- 1800-1900 (i.e. 19th to 20th-century). Starting with the one-layered mask made of gauze it advanced to the two-layered mouth protection made of gauze then to multilayer face mask made of gauze that can be found in the surgical operating teachings of the British surgeon B.G.A. Moynihan (1865–1936), (Figure 21).
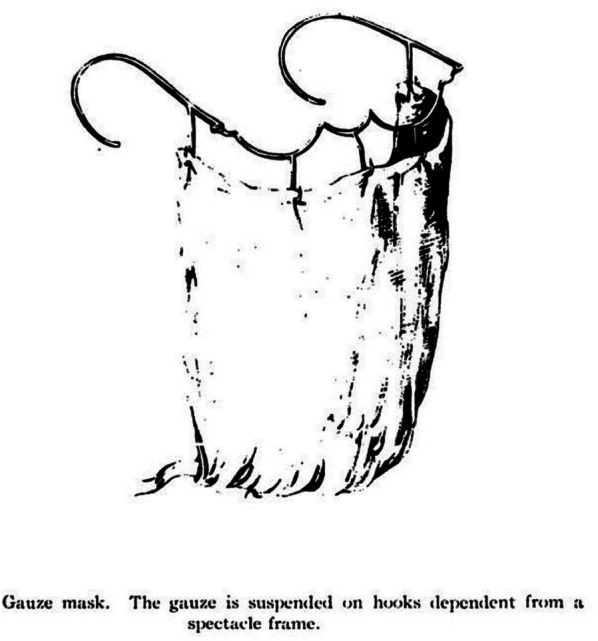
Figure 22 shows the design of masks worn by doctors to perform plague inhalation experiments in 1916 and during the pandemic flu (i.e. Spanish flu) in 1918 and other images that reflects on the various events during the pandemic. The “Spanish flu”, also known as the Great Influenza epidemic or the 1918 influenza pandemic, was an exceptionally deadly global influenza pandemic caused by the H1N1 influenza A virus. Although the United States and the other nations at war initially suppressed news of the flu (neutral Spain freely reported it, hence the misnomer “Spanish flu”). The earliest documented case was March 1918 in Kansas, United States, with further cases recorded in France, Germany and the United Kingdom in April. Two years later, nearly a third of the global population, or an estimated 500 million people, had been infected in four successive waves. Estimated death ranged from 17 million to 50 million, or possibly as high as
100 million, making it one of the deadliest pandemics in human history” [68, 69, 70]. Furthermore, figure 23 shows the modern era precursor to surgical mask wore today, that was used first in the operating rooms of Germany and the USA in the 1920s, to prevent the migration of microorganisms residing in the nose and mouth of members of the operating team to the open wound of the patient (i.e. protecting wounds from surgeons- breath and predominantly bacterial droplet contamination) [71, 72, 73]. Continuously, as technology developed new materials and designs, their filtering efficiencies gradually improved, leading to the distinction between surgical masks and surgical N95 respirators in use presently, Figure 24 [74, 75]. Precisely, in 1918, advanced masks like the N95s that healthcare workers use today were a long way off. Then surgical masks were made of gauze, and many people’s flu masks were made of gauze too. Red Cross
volunteers made and distributed many of the masks then.
![Figure 22: Design of masks worn by doctors during the pandemic flu in 1918 and other images that reflects on the various events during the pandemic [68-70].](/fulltextimages/11046/fig_22.png)
![Figure 23: The precursor to modern surgical mask being used in the operating rooms of Germany and the USA in the 1920s [71-73].](/fulltextimages/11046/fig_23.png)
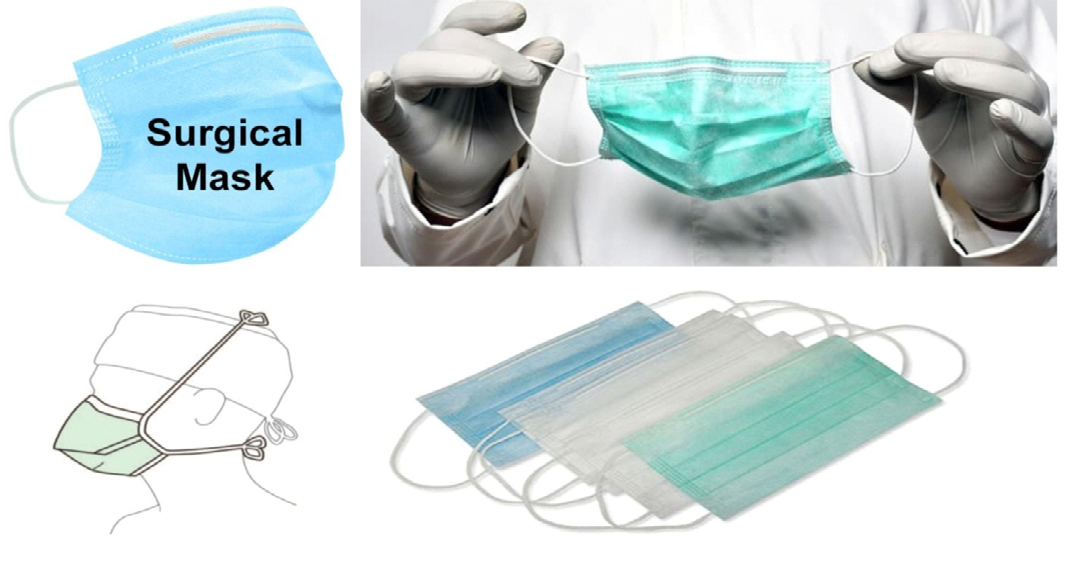
![Figure 24: Typical example of the present day surgical masks and surgical N95 respirators [74-77]. Existing Configuration of Face Barrier Coverings: In the day to day language “Face Barrier Coverings” i.e. the devices that are worn on the face, which covers at least the nose and mouth, with the primary purpose of providing source control and to provide a degree of particulate filtration to reduce the amount of inhaled particulate material are collectively referred to as mask or face mask. In reality, they are simply distinguished as particulate respirators and particulate face masks or technically distinguished as surgical respirators; non- surgical respirators, medical/ surgical face mask, and non- surgical/medical face mask (i.e. cloth/homemade face mask). They differ by their configuration type and effectiveness of filtering infectious particles and wedging droplets via inhalation and exhalation. In all, the basic, “regulatory standards require that the face barrier covering should not permit blood or other potentially infectious materials to pass through to or reach the wearer’s skin, eyes, nose, mouth, or other mucous membranes under normal conditions of use and for the duration of time that the protective equipment will be used.” Furthermore, particulate respirators are distinguished as either valve- respirators or non valve- respirators. The valve- respirators make it easier to exhale air which makes them more comfortable to wear, because it leads to less moisture build-up inside the respirator. However, “the problem with valve respirators is that they “do not” filter the wearer’s exhalation, only the inhale. This one-way protection puts others around the wearer at risk.](/fulltextimages/11046/fig_24.png)
Figure 24: Typical example of the present day surgical masks and surgical N95 respirators [74, 75, 76, 77]. Existing Configuration of Face Barrier Coverings: In the day to day language “Face Barrier Coverings” i.e. the devices that are worn on the face, which covers at least the nose and mouth, with the primary purpose of providing source control and to provide a degree of particulate filtration to reduce the amount of inhaled particulate material are collectively referred to as mask or face mask. In reality, they are simply distinguished as particulate respirators and particulate face masks or technically distinguished as surgical respirators; non- surgical respirators, medical/ surgical face mask, and non- surgical/medical face mask (i.e. cloth/homemade face mask). They differ by their configuration type and effectiveness of filtering infectious particles and wedging droplets via inhalation and exhalation. In all, the basic, “regulatory standards require that the face barrier covering should not permit blood or other potentially infectious materials to pass through to or reach the wearer’s skin, eyes, nose, mouth, or other mucous membranes under normal conditions of use and for the duration of time that the protective equipment will be used.” Furthermore, particulate respirators are distinguished as either valve- respirators or non valve- respirators. The valve- respirators make it easier to exhale air which makes them more comfortable to wear, because it leads to less moisture build-up inside the respirator. However, “the problem with valve respirators is that they “do not” filter the wearer’s exhalation, only the inhale. This one-way protection puts others around the wearer at risk.
Similarly, there are two main distinguished categories of the particulate face masks. The surgical masks sometimes referred to as medical or procedure masks are disposable masks commonly used in healthcare settings and the reusable/washable fabric masks often referred to as cloth/homemade masks or non- surgical/medical masks. Procedural masks are traditionally characterized by surgical ties behind the head while cloth/homemade fabric masks are characterized by an ear loop attachment, (Figure 25).
The respirator and medical mask filters in current use are typically composed of mats of non-woven fibrous materials, such as wool felt, fiberglass paper, or polypropylene, while those for the non-medical/cloth/homemade face masks are typically composed of textiles that are likely to filter well and be breathable such as woven cotton (at least 100 threads per inch); flannel (either cotton or poly-cotton blend- at least 90 threads per inch; tea towel material; cotton T-shirt material; etc. which are mostly made of at least two layers; three or four may be even better.
The first layer (closest to the mouth and nose) should be made of cotton or another moisture-wicking fabric to absorb droplets from the exhaled breath. The middle layer should be made of polypropylene (a non-woven material e.g. melt- blown, spun-bond or spun-lace). The outer layer should be made of a fabric that will repel moisture, such as polyester or a polyester-cotton blend. Conventionally, surgical masks and procedural masks are generally speaking a 3-ply (three layers) design, with 2 sheets of “non-woven” fabric sandwiching a “melt-blown” layer in the middle, (Figure 26). It’s the melt-blown layer that provides the filtering capability while the non-woven layers provide the moisture resistant. Usually N95 respirators block 95% of airborne particles >0.3, while the overall filter capacity of face barrier covering i.e. their non-oily particulate matter filtration efficiency ranges from 80% to 99.97% (ability to remove all particles that are 0.3 microns in diameter or larger).
![Figure 26: Typical 3-ply (three layers) design surgical masks and procedural masks [75,78].](/fulltextimages/11046/fig_26.png)
In general, the overall filtering materials for making face masks and respirators fall into two major categories- woven materials e.g. woven cotton fabric and non-woven materials. “Traditional materials for clothing and furniture have a woven or knitted structure. Non-woven materials, by contrast, have a random arrangement of fibers, like spaghetti on a plate (a fabric or structure in the category of non-woven textile materials). The non-woven is made of either natural fibers or synthetic thermoplastics. There are many types of non-woven polypropylene. The most common are spun- bond, melt-blown and spun-lace materials.” Non-woven materials such as the spun-bond polypropylene are formed from there randomly oriented fibers (petro-chemicals) which are compressed and melted together in a pattern of small, closely spaced welds, called point bonds. “The polypropylene can be cleaned using “a hot wash with detergent”. It can be washed with the mask or separately. It should not be tumble dried: it should be removed from the mask and hung or laid flat to dry before reinserting. Do not iron it: it is plastic and will melt”.
Figure 27 depicts the charts for a fair comparison of the effectiveness of the different types of materials used for making face barrier coverings (particulate respirators and particulate face masks). And Figure 28 presented the top 5 DIY (do it yourself) ultimate mask materials based on several studies [79, 80]. Hence, all these barrier face coverings may be made from a variety of materials that are not flammable. It also revealed that layering of the material made a difference i.e. multiple layers of the same fabrics and for sandwiches of different materials. For example, a two-layer T-shirt mask with a sewn edge (which prevents stretching), prevented 79 per cent of mouth bacteria reaching the environment during coughing. In the same experiment, a modern disposable medical mask performed in the same range at 85 per cent. Similarly, a four-layer cotton mask and a mask made of a sandwich of cotton and flannel both reduced mouth bacteria in particles of all sizes reaching the environment during talking by 99 per cent and mouth bacteria in fine particles by 89 per cent. This is all good evidence that cloth face coverings can prevent respiratory secretions from reaching the environment. Every coarse or fine particle trapped in a mask is not available to hang in the air or fall to a surface and contaminate it, which translates to the slogan “my mask protects you, your mask protects me”. (Figure 28).
![Figure 27: Percentage effectiveness of the different types of materials used for making particulate respirators and particulate face masks [81].](/fulltextimages/11046/fig_27.png)

Notably, the current designs of many of the cloth masks in use are usually made with several types of reusable gauze or woven cotton and are likely producing dual levels of filtration to the person wearing them. That is, they have the ability to protect against inhaled particles and also resist fluids and limit the dispersion of exhaled properties. Hence the phrase/ slogan, “my mask protects me and you, your mask protect you and me”, (Figure 29). The cloth/homemade or non- surgical masks come in many styles and fabrics, (Figure 30). Some have straps that tie behind the head or loop around the ear to hold it tight. On the other hand, some have a curved vertical seam in the center; to make the mask bow out and give the wearer room to breathe. While others have multiple horizontal folds that enable the wearer to adjust the fit up or down easily, (Figure 31).
![Figure 29: Shift in mask design from “one way protection” to “two way protection” [82].](/fulltextimages/11046/fig_29.png)


There are multiple types of face barrier coverings currently in stock and the exact specifications may vary as follows:
- Non-Woven Fabric Outer Layer
- High-Density Filter Layer
- Soft Absorbent Inner Layer
- Adjustable Metal Nose Clip (a bendable nose strip to help prevent air from leaking out of the top of the mask)
- Latex-Free and Fiberglass-Free
- Ear Loops
- Soft Lining and Breathable
- Bacterial Filtration is over 99%
- One Size Fits All etc. (figures 30 and 31).
- Alternative face masks for special situations and transparent medical mask (Figure 32).
- Zipper face mask (to enable eating and drinking with masks), (Figure 33).
- New 3D-printing face masks and nasal illness defender mask, (Figure 34).
Alternative face masks for special situations are either clear masks or cloth masks with a clear plastic panel that may be helpful when interacting with certain groups of people, such as:
- People who are deaf or hard of hearing
- Young children or students learning to read
- Students learning a new language
- People with disabilities
- People who need to see the proper shape of the mouth for making appropriate vowel sounds (for example, when singing) The FDA recently approved a transparent medical mask. These transparent medical masks should be reserved for use by healthcare workers and patients who require them. If you use this type of mask, make sure
- You can breathe easily
- Excess moisture does not collect on the inside of the mask


![Figure 34: New 3D-printing face masks and nasal illness defender mask [83-86].](/fulltextimages/11046/fig_34.png)
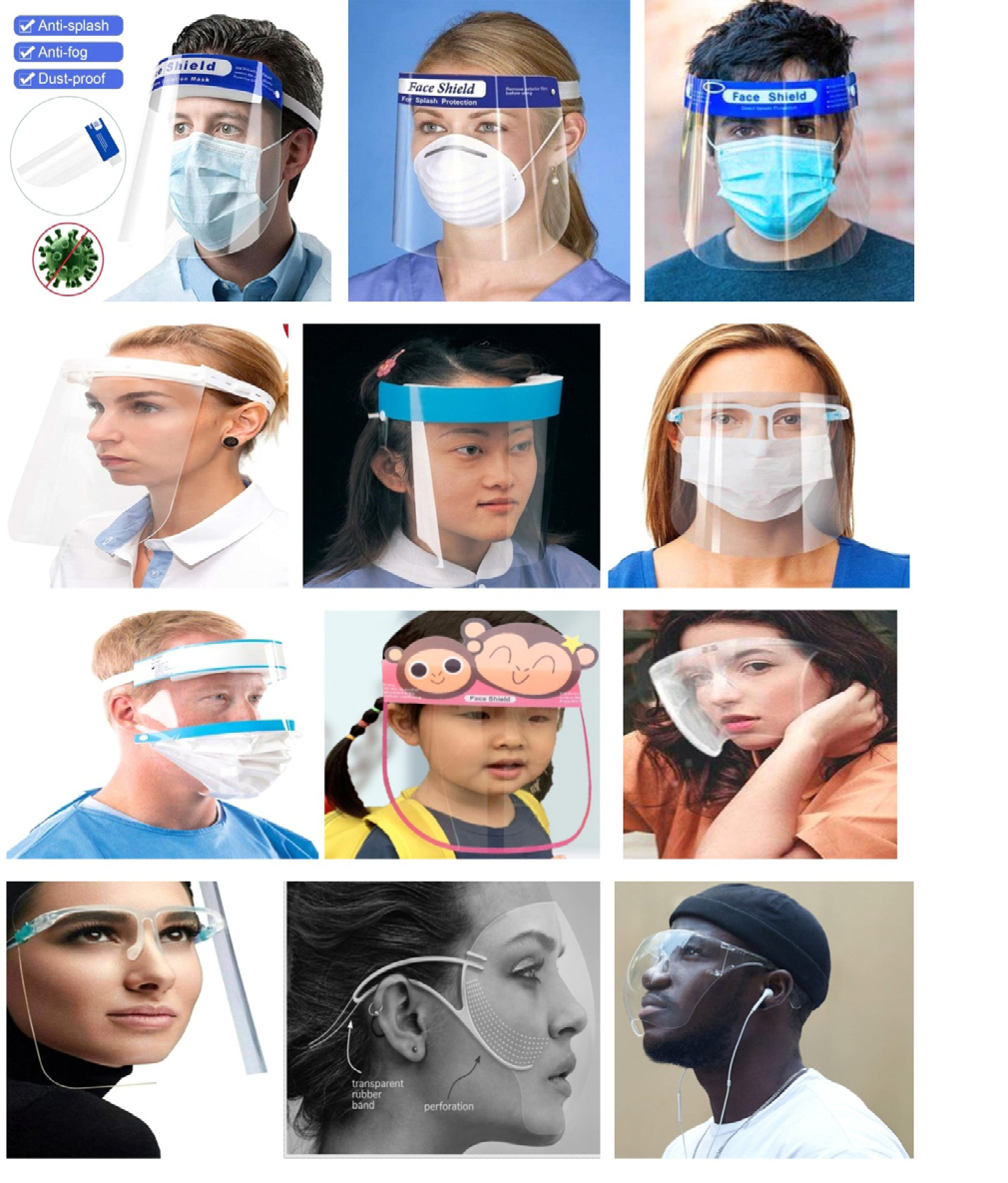
Figure 35: Different types of the conventional transparent full length face shields (covers eye, nose and mouth). The most common complimentary face barrier covering is the face shield, which is simply a curved plastic or Plexiglas panel attached to a headband that can be worn over the face to protect the eyes as well as the nose and mouth i.e. the wearer’s entire face (or part of it), (Figures 35 & 36), from hazards such as flying objects and road debris, chemical splashes (in laboratories or in industry), or potentially infectious materials (in medical and laboratory environments). It is designed to fit securely (i.e. no gap) between the headband and the forehead as well as wrap around the sides of the face and extends below/beyond the chin. Study suggested that, when face shields was tested against an influenza-infused aerosol from a distance of 18 inches away, it reduced exposure by 96% during the period immediately after a cough and also reduced the surface contamination of a respirator by 97%. Hence it protects the wearer. Because the face shield is away from the wearers face, when he cough or sneeze, those droplets can still get out more than with face mask. Therefore, it is idle to wear a particulate face mask or respirator underneath the face shield and maintain physical distancing, to minimize infecting others with the droplets escaping from the opening at the bottom of the face shields. Comparatively, face mask or respirator absorbs droplets when the wearer coughs or sneezes while face shields do not. Hence it should be sanitized/sterilize frequently with an antibacterial wipe, alcohol pad or soap and water. Notably, viruses live on plastics a lot better than it survives on porous materials such as cloth, paper or cardboard. On the alternative, Figure 37 shows the complimentary use of eyeglasses with face mask.


![Figure 38: Other partial covering of the face for some specific purposes [87].](/fulltextimages/11046/fig_38.png)
Figure 39 shows that the conventional comedian’s fake nose, mustache and mouth, are simply independently molded large representative of human nose, mustache, mouth that can be coupled together at will to satisfy particular exercise, while the splash optics eyeglasses usually incorporate nose covering.

Proposed Nasal-Mouth Masks, Respirators and Face Shields Combinations
The proposed IJN (a.k.a. AIBE) models of barrier face coverings are designed to prevent/alleviate most of the numerous health, logistical, physiological, psychological, social and economic complications associated with wearing the present types of face barrier coverings, as well as become the customary/regular personal protective equipment (PPE) wear for both ambient (outdoor environments) and household (indoor) air pollution.
The different conceptual models are aimed at combining non-full face masks i.e. semi-face masks such as nose filters/ masks, mouth covers/masks or mouth shields and the eye protectors/covers or shields, for multipurpose usage; for example
- To fight COVID-19, i.e. as personal protective equipment/ device for the purposes of preventing the on-going air- borne virus infections and its endemic phases, their likes (measles, chickenpox, tuberculosis, etc.), and any other type of future outbreaks of virus disease from assessing human body through the sense organs (nose, mouth and eye);
- For prevention against inhaling dust or other air borne particles and chemicals in polluted environment i.e. work places, in public gatherings e.g. classrooms in schools and universities, churches and Islamic centers, barracks, markets, political rallies, senates and house of assembles, amusement parks, wedding and entertainment halls, in transit transportations such as airplanes, ships, trains, buses and taxi, etc. as well as in private homes;
- Some are customized design that can accommodate the use of inhaler for asthma patients, straw for drinking, zip/ clip for eating solid food, etc. Simply put, it is configured to separately protect the different sense organs i.e. nose, mouth and eyes as nature intended, thereby eliminate or control most of the health issues associated with re-breathing CO2, mask associated dry eye “MADE”, bacteria phenomena, red marks/bruised face and other inconveniences/irritation on the face (around the nose, mouth and eye) experienced with wearing the existing models of surgical/medical masks, cloth/homemade masks, surgical/non-surgical respirators and face shields.
Of special benefit and interest is the fact that it is configured as an ornamental wear, to be used as a regular make-up dressing gadget much like the wrist watches, ear rings, sun glasses, ankle bangles or anklets, beads, neck-lace or neck chains, etc., such that it serves dual purposes. Firstly it protects the wearer 24/7 from inhaling any form of air borne particulates and pollutants (including viruses, bacteria, smoke, dusts, etc.) and secondly serves as beautifying cosmetics (e.g. used in place of cosmetic surgery or enable an individual to appear in any shape of nose he desires at any time, such as pointed, flat, round, etc.), because it can be configured much like human complexion. Some could be aromatized to produce pleasant refreshing sweet-smells or fragrant if desired in any particular environment or situation (i.e. aromatherapy).
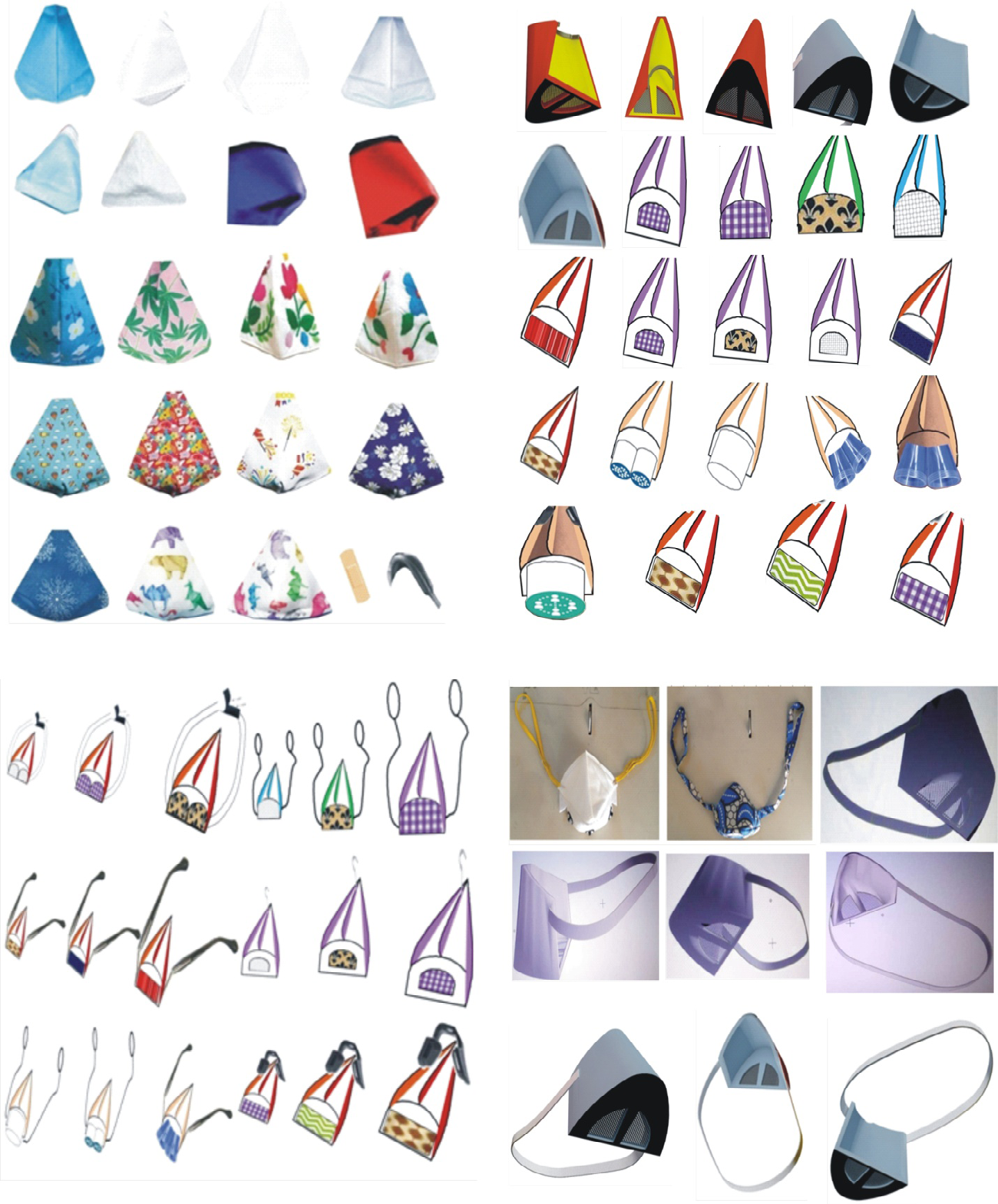
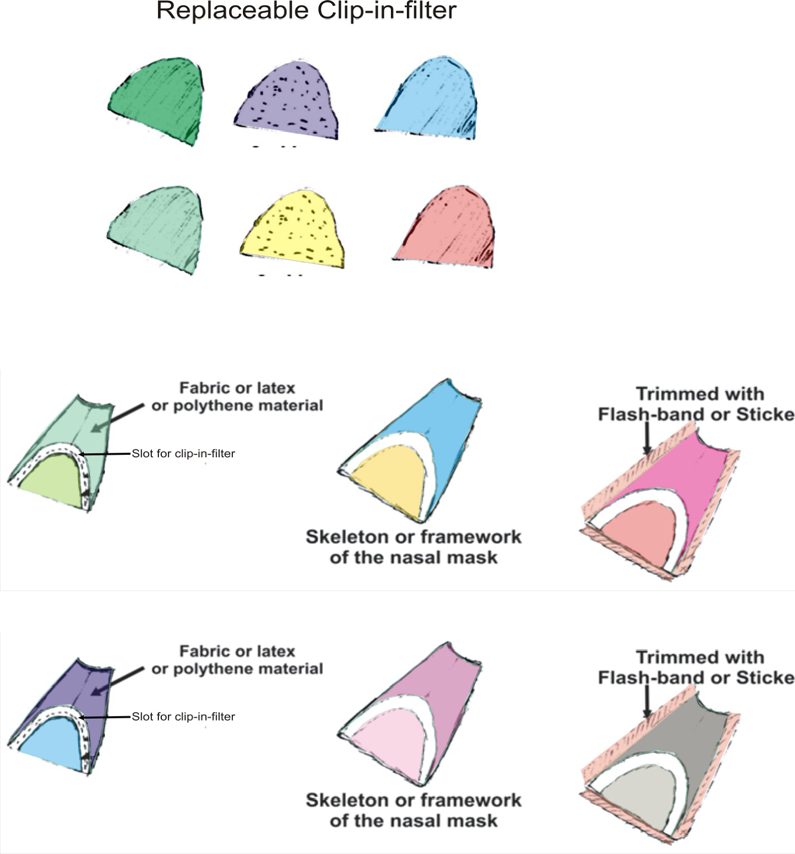
It is produced/fabricated with the same types of materials used in producing the existing models, as recommended by the World Health Organization (WHO), such as cotton fabrics, polypropylene, plastics, rubber or latex, polyurethane, or their combination, plus standard ear loops, stickers, flash bands, plasters, clips, hooks, Velcro, buckle, belt, or rope to secure it tightly on the nose, mouth or eye or fasten it behind the head. The IJN models of semi-face barrier coverings/masks, is aimed at making, the wearing of air-borne pollutants protective gadgets part of human beings regular dressing mode with little or no discomfort or concealing face recognition issues. The designs as reflected in the following figures 40 to 51 are not the perfect real finished fittings rather it illustrates the ideal concepts.
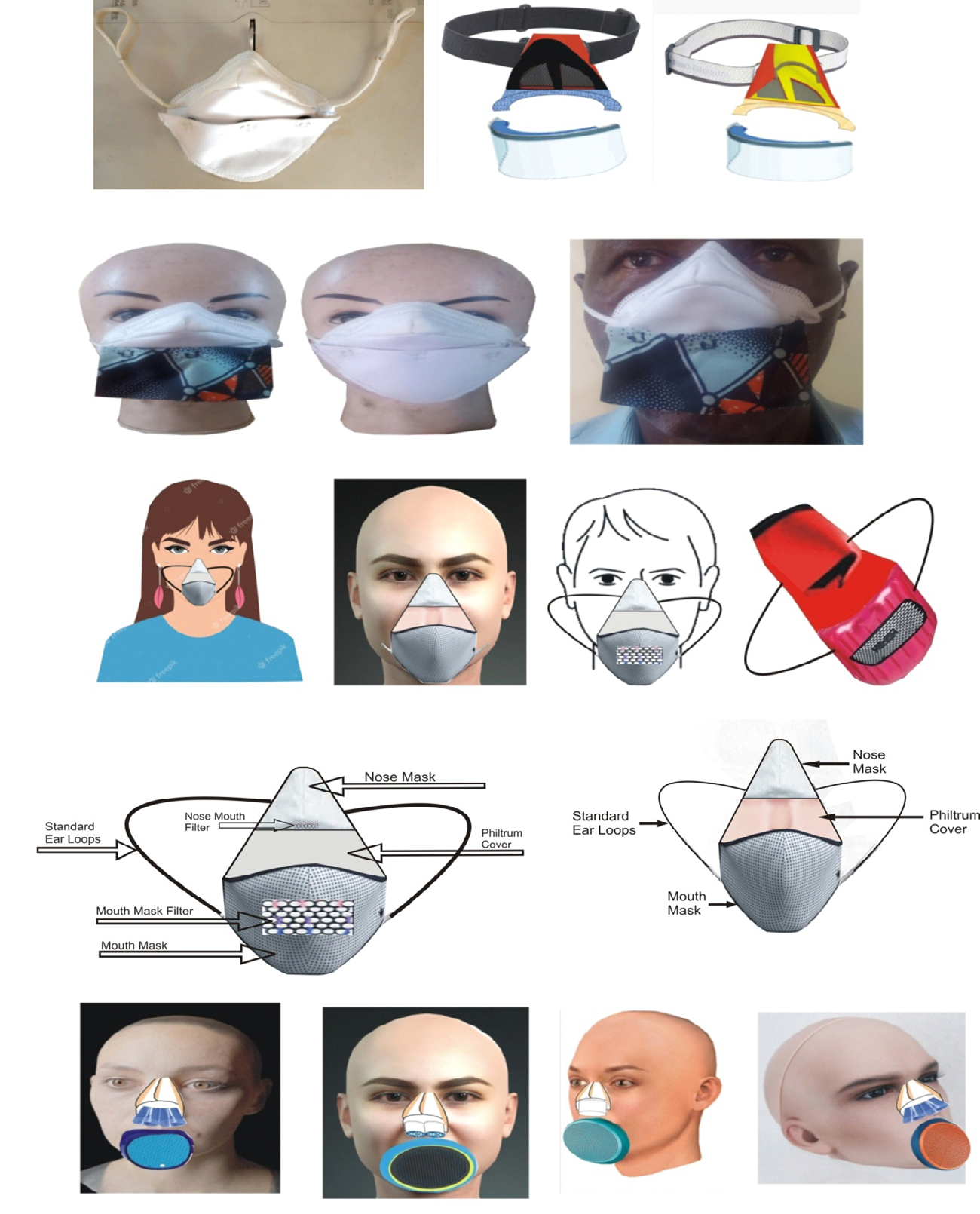
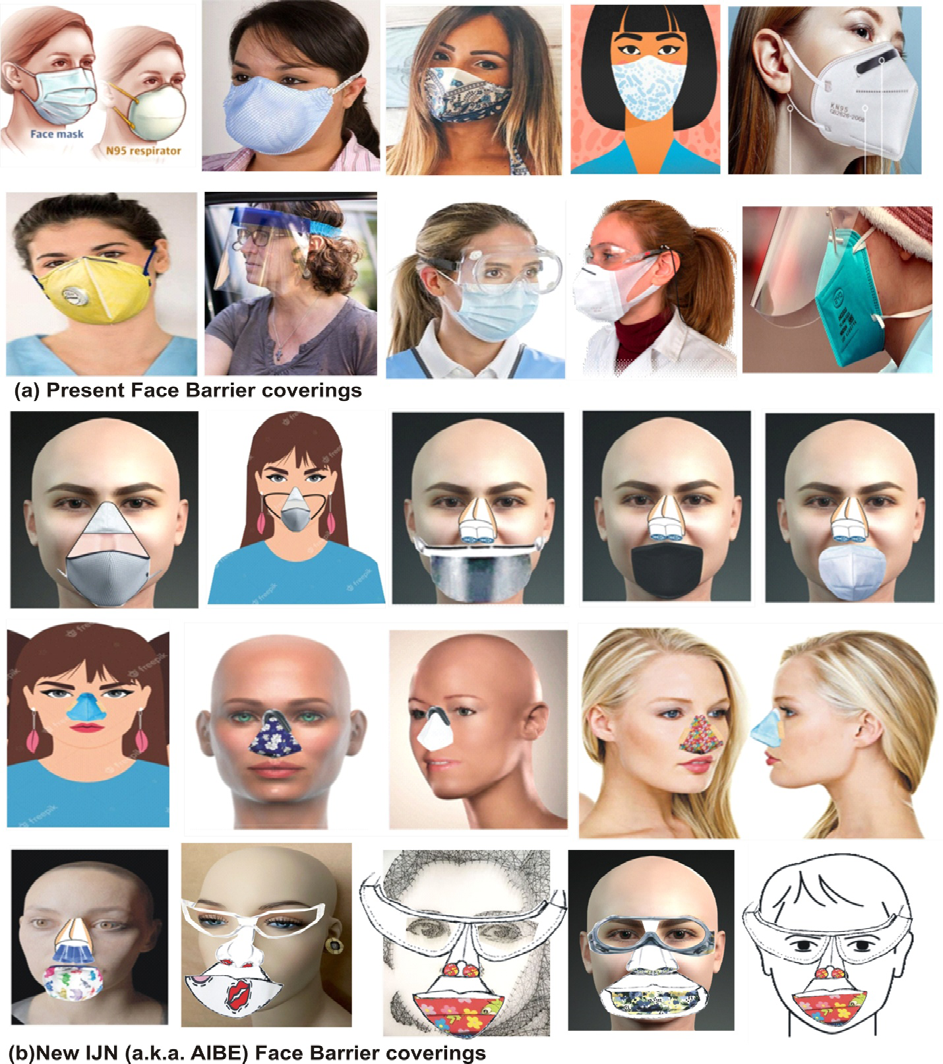
Specifically, figures 40 to 42 distinguished the different nose/nostril design models and their applications; figures 43 and 44 distinguished the different mouth design models and their applications; figures 45 and 46 presented the different configured combined nose and mouth applications; figures 47 and 48 presented the different configured complete face frame for eyes, nose and mouth applications; figures 49 and 50 illustrated the modes of replacing the disposable nose and mouth filters design options; while figure 51 displayed side-by-side typical samples of wearers of the present face barrier coverings and wearers of the proposed IJN (a.k.a. AIBE) face barrier coverings (Courtesy azuberths research complex Owerri, Nigeria).
Notably, nose/nostril protections models (complete or brief sizes) can be contoured or fabricated to the size of any desired nose type or shape with disposable or washable materials. As depicted in figures 40, it could be used by any of the following techniques, clipping on the nose, using ear handle, hooking it onto the frame of an eyeglasses, elastic rope, Velcro belt or button etc. All of which can be adjusted to perfectly fit the wearer, e.g. adults and children, Figure 41. Furthermore, Figure 42 depicts the designs and applications of the elastomeric material nose mask with reusable/ exchangeable filter elements (cartridges or filters), that may be selected to provide the needed level of filtration (80 to 99.97) i.e. rubber wear latex prosthetics nose masks. It mimics the rhinoplasty (also known as nose job or cosmetic surgery) used to alter the nose shape into any other preferred shape. They are carefully sculpted or textured like skin and the edges are tissue thin for invisible blending. On the other hand, the sole mouth masks, mouth shields, mouth covers and mouth pads as depicted in Figure 43, could be used by any of the following techniques, plasters or flash bands, by using ear elastic rope, Velcro belt or button etc. adjustable to perfectly fit the wearer, and also with mouth clips or lips clips for eating solid food or drinking liquids, which are made with either zip or flip-up cover like button. In Figure 43a the cap is designed such that it could be flipped-up to eat while a straw is used through the nub for drinking in public, while Figure 43b is mouth shaped net cup/cover and Figure 43c is zipping system. Figure 44 presented the different techniques of using the mouth masks design configurations.
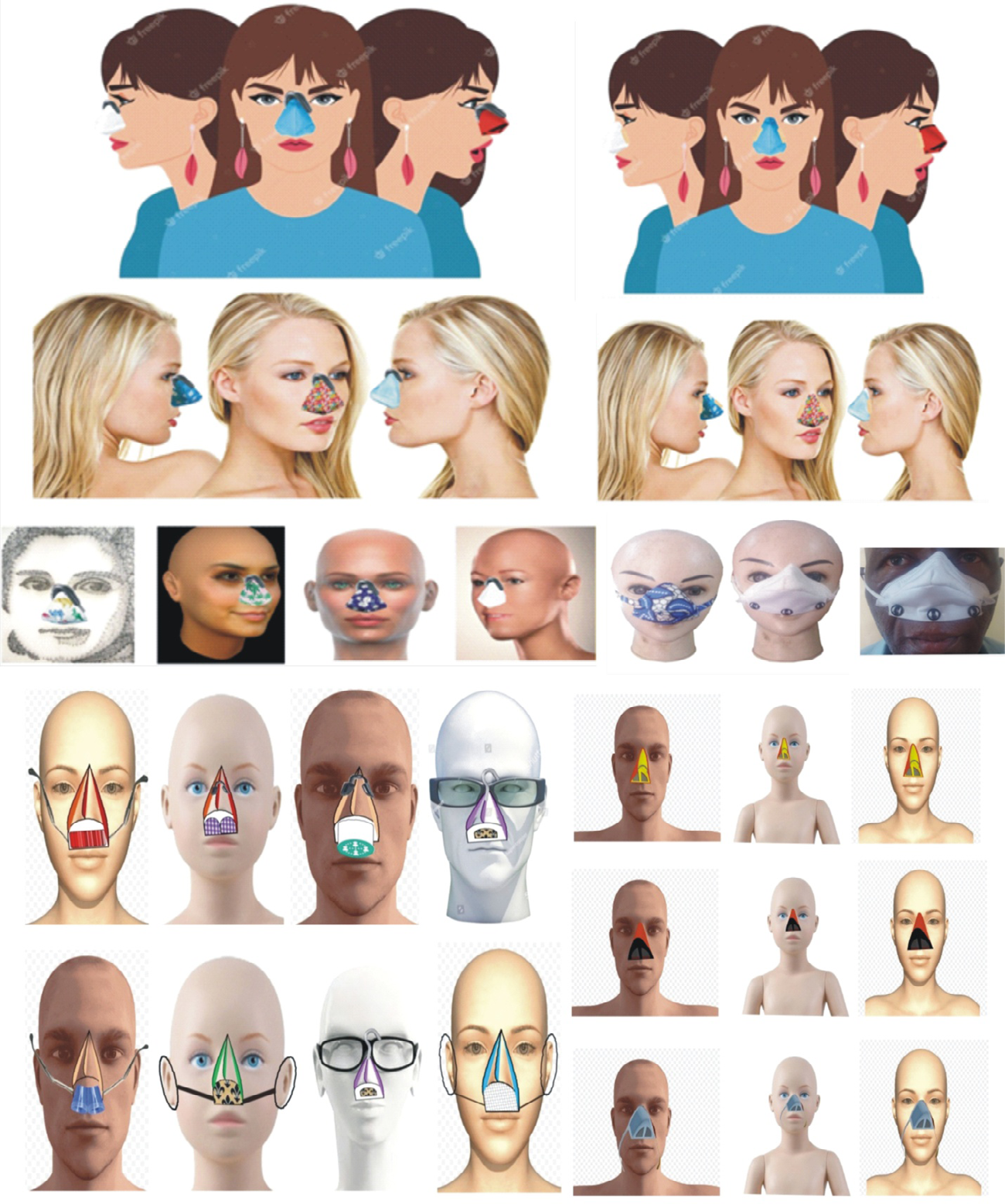


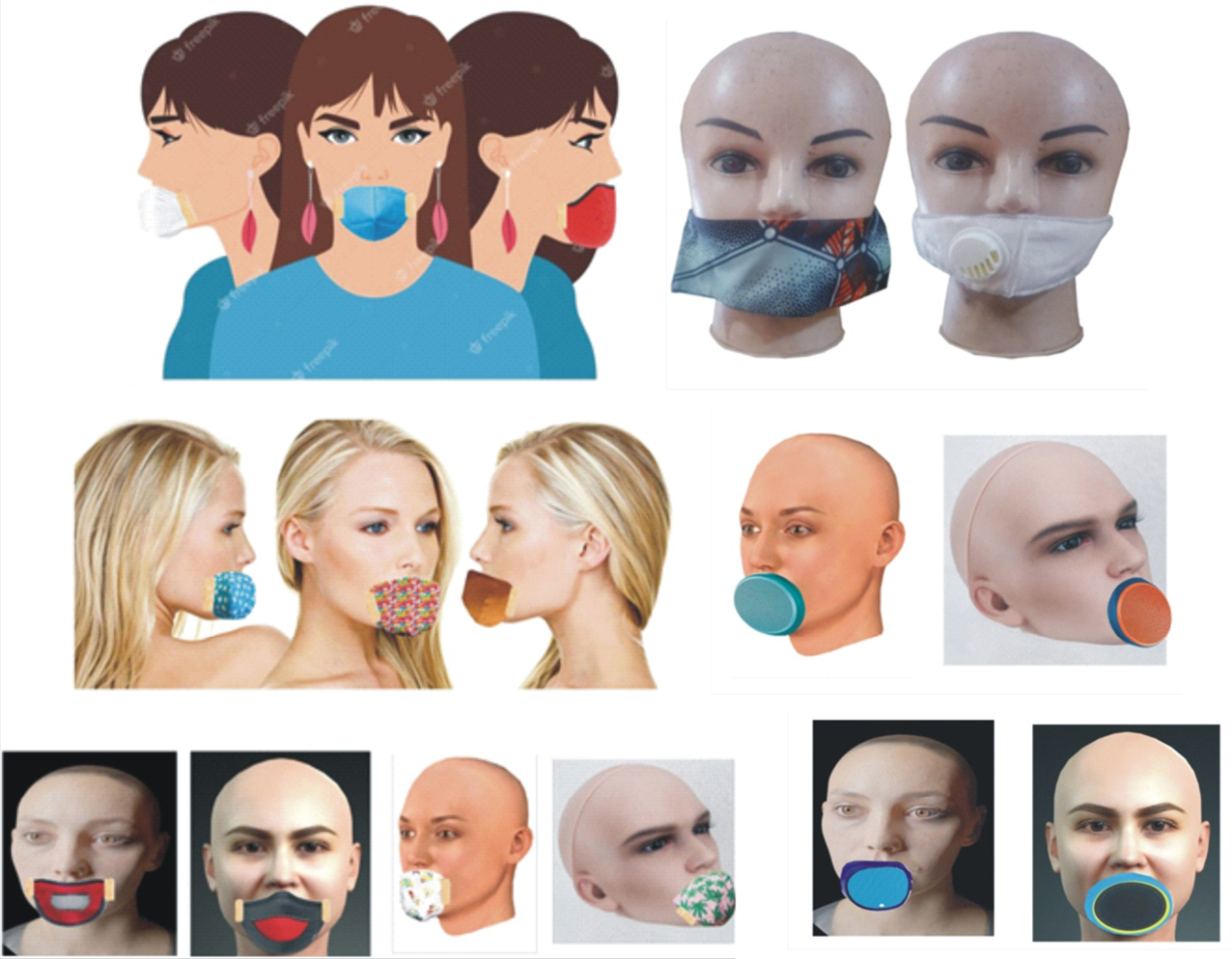
The configuration of Figures 45 & 46 depicts a modified full face masks (nasal filter and mouth cover combination) which, depending on the situation, at any time enables the wearer to wear only the nasal filter or only the mouth cover. Precisely, in one option the two are attached together with button or Velcro, hence the wearer can chose when to detach or attach any of the two for his or her convenience. In another option, they are two separate gadgets, in which the nose clip only secures the nasal filter while the plaster only secures the mouth cover. Alternatively, the nose frames option allows the wear to fit different fabrics to match the dress wore i.e. uniform for any purpose/function.

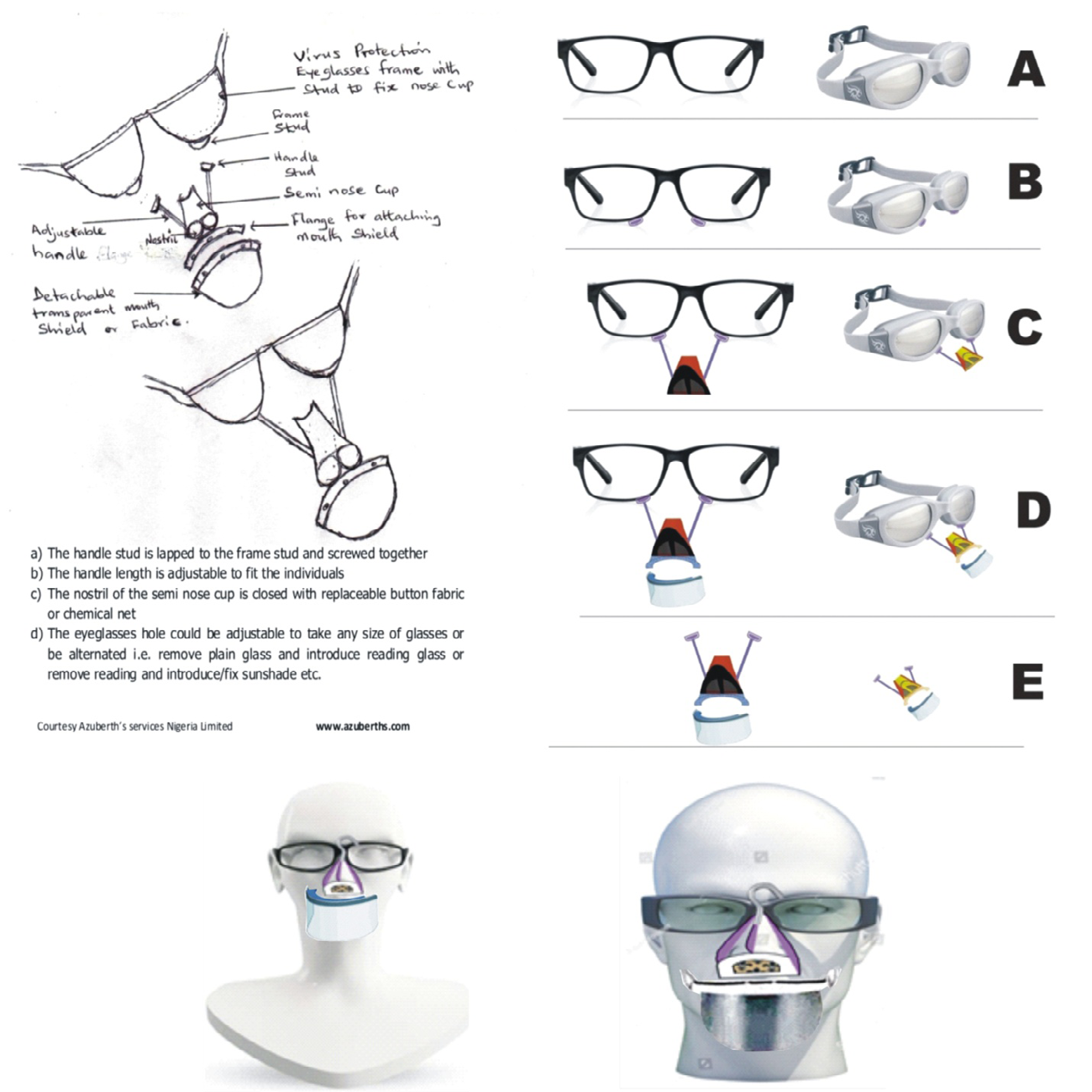
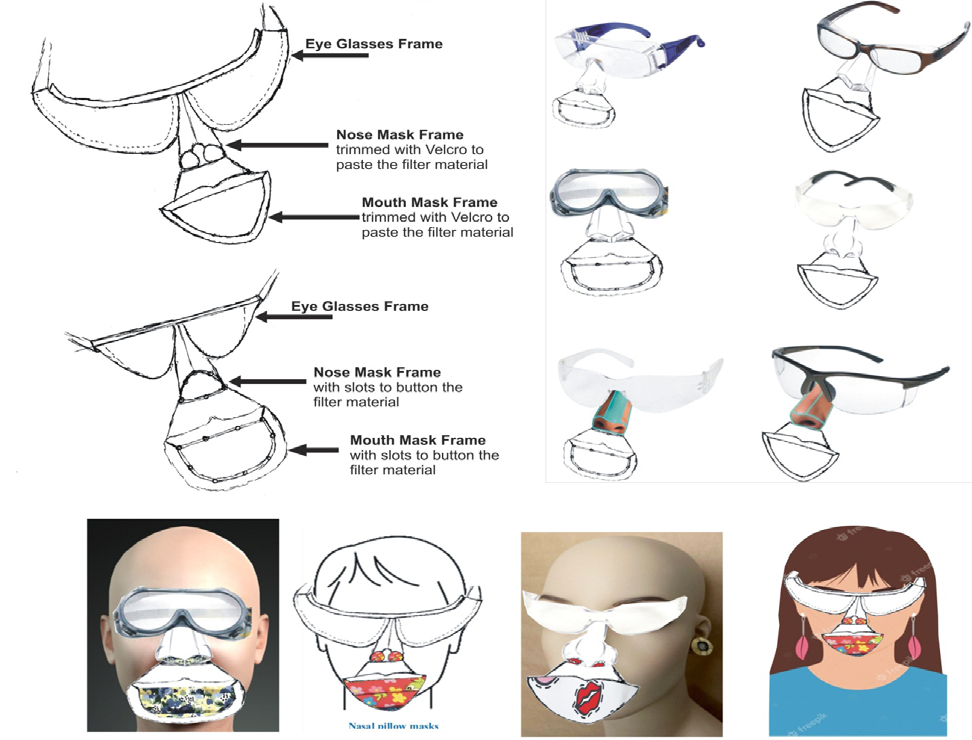
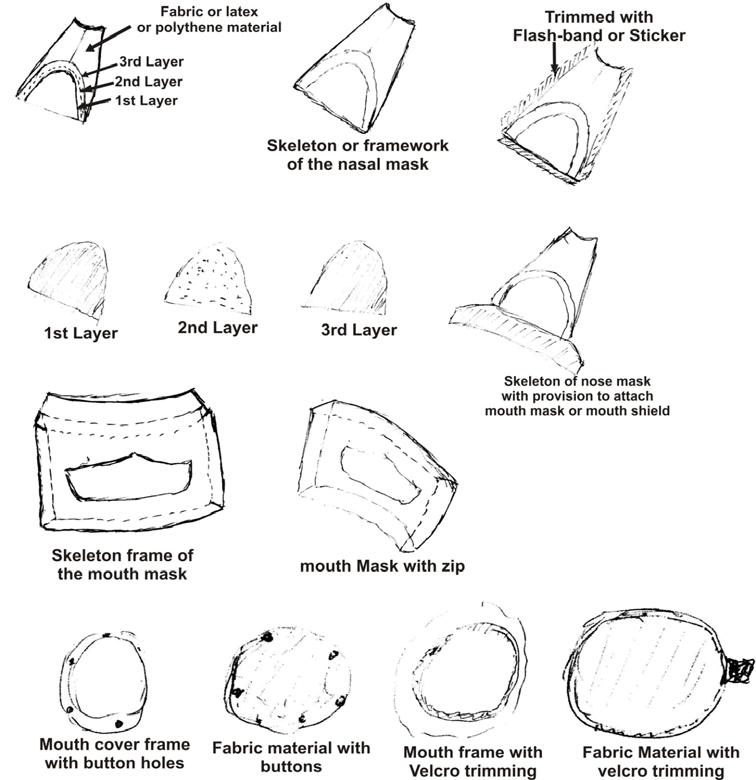
The models of face barrier coverings frame for the protection of eyes, nose and mouth, as depicted in Figure 47, reflects that the nose filter and mouth cover, can be attachment to the frame of eyeglasses, in such a manner that will prevent nose breath-out from entering the mouth as well as prevent mouth odor from entering the nose. Similarly, depending on the situation, at any time the wearer can chose when to detach or attach any of the three for his or her convenience. And Figure 48 presented a customized complete face protection frame design wherein the eyes, nose and mouth sense organs are protected against virus and any airborne pollutant, which also prevent nose breath- out from entering the mouth as well as prevent mouth odor from entering the nose. Figures 49 and 50 shows the modes of replacing the disposable nose filter and mouth covers on the customized face protection frame design.
Research Complex Owerri, Nigeria).
Comparison on Cosmetic Appearance and Other Health or Thermo-Physiological Effects
In figure 51, typical samples of those wearing the present (full face masks, N95s respirators, face shields and combination of face shield-masks or goggles-masks) are placed side by side with samples of those wearing the different varieties of the proposed IJN semi-face masks (a.k.a. AIBE semi-face masks) models, as well as the customized complete face protection frame design that incorporates the eyes, nose and mouth sense organs protection simultaneously or in any preferred option. Comparatively, wearing the existing configuration of face barrier coverings (masks or N95s) tends to conceal or hide the wearer’s face, while the proposed IJN semi-face masks (a.k.a. AIBE semi-face masks) that are modeled as nasal- filters; mouth-covers; eye-protectors virtually retains must of the facial features of the wearer’s. Also, in comparison, wearing the present configuration of particulate face masks that are loosely fitting makes the exhaled air go into the eyes (generates tear from the eyes, which gradually dries the eye as well as develop fogs on eyeglasses), while this proposed sole nose filter or mouth cover options, is an automatic source control (with zero possibility of directing the flow of the exhaled air over the eyes) for mask associated dry eye and foggy eyeglasses, (i.e. zero mask associated dry eye and foggy eyeglasses). Furthermore, by prolonged use of the existing particulate barrier face covering, the normal human airway breathing process is disrupted due to the continued/repeated re-inhaling of some fractions of the wearer’s previously expelled breath, possibly contaminated with some fractions of the odor/gas from the mouth, in the confined space within the barrier face covering i.e. excessive (re-breathing our own exhaled) carbon dioxide (CO2) instead of fresh oxygen, which may lead to a variety/different health issues. Such as increased blood pressure, headaches, dizziness, shortness of breath, muscle twitches, rapid heart rate, chest pain, confusion, fatigue, vertigo, double vision, and in extreme cases, if left untreated, hypercapnia can lead to organ damage and even have long standing effects on the brain, hyperventilation, seizures, or suffocation due to displacement of air and possible death. Simply put, inhaling high levels of carbon dioxide (CO2) may be life-threatening.
On the other hand, by its design, the proposed IJN (a.k.a. AIBE) models are configured (to cover only the nose region) such that CO2 build-up inside the nose masks are minimized since it virtually has direct gas exchange with the environment i.e. there is zero to insignificant possibility of retaining exhaled air in a confinement for re-breathing exhaled CO2. Again, the prolonged use the present configuration of particulate face masks is associated with thermo-physiological responses/ effects such as discomfort and irritation around the region of the nose and mouth, i.e. red marks, bruised face, feeling unfit, tight, itchy, fatigued, odorous and salty; microclimates and skin temperatures inside (such as heart rate and thermal stress), breath resistance/breathing seems harder, etc. This proposed modified configuration will maximally eliminate or significantly reduce these problems, since the face is not cover at all (only the nose and mouth). Notably, with the IJN models there is no significant dead space volume and breathing resistance is reduced to the barest minimum, hence it is expected that there is no overall significantly reduced possible gas exchange volume of the lungs. Breathing tends to be normal since filters are frequently replaced to avoid heavy face masks contamination. As for the perception of humidity (inside the surface of face mask and outside the surface of face mask), i.e. masks are soaked by exhaled air, which potentially accumulates infectious agents from the nasopharynx and also from the ambient air on the outside and inside of the mask” (in particular, serious infection-causing bacteria, fungi and also viruses), because most of the models use exchangeable filters such that disposable (filter materials are regularly replaced), they are expected to be either milder or non-existing with the IJN (a.k.a. AIBE) models. Usually, the quality and the volume of speech between two people wearing masks are considerably compromised and they may unconsciously come closer. In comparison, it will be completely eliminated by wearing the proposed models.
Comparison based on Economic Implication
Face Barrier Coverings are either disposable or reusable/ washable. “Disposable masks represent a category of masks intended for one-time use only-unlike reusable masks, which are often made of cotton or polyester material, disposable masks are not intended to be washed and re-worn.” Disposable masks most commonly include procedural, surgical and N95 masks that are originally designed for use in medical environments, including patient procedures, isolation or dental practices. The main economic consideration is the cost of buying the masks for use within a period of time (one mouth to one year). For the disposable this means one mask every day, while for the reusable/washable it means an average of two masks in a mouth. Presumably, the same material used to make one of the present face masks or N95s respirator mask can be used to produce, either four pieces of semi nose filter or two pieces of semi mouth cover or six pieces of mouth filters, (Figure 52), of the new IJN (a.k.a. AIBE) models, depending on preferred option. In some nose filter design, it could produce well over twenty pieces, since most of the proposed IJN models include some other frame materials, which can last more than one year. Everything put together, the cost of using the new IJN models for a period of two mouths is expected to be 0.5 % (1/2) i.e. half the cost of using the present face masks or N95s respirator masks within the same period.

Further Economic issues
The IJN (a.k.a. AIBE) models tackled the major economic complications associated with the present designs of barrier face coverings as follows:
- The N95 respirators tend to be more expensive than fabric/cloth masks and cannot be washed. All FDA- cleared N95 respirators are labeled as “single-use,” disposable devices. They need to be discarded when they are dirty or soiled, damaged, or difficult to breathe through and replaced with a new one.
- Instead of discarding the entire unit, the active area could be replaceable for a very long period with the proposed IJN (a.k.a. AIBE) models. To replace the active area at the end of the day, safely pull or slid it off the chamber of the N95 respirator and discard by placing it in a plastic bag and dropping it in the trash. Wash your hands after handling the used active area of respirator.
- The N95 respirators are not designed for children or people with facial hair. Because a proper fit cannot be achieved on children and people with facial hair, the N95 respirator may not provide full protection. In those cases, a special respirator called a powered air-purifying respirator may be used instead (that ideally is more expensive).
In this case, the proposed IJN (a.k.a. AIBE) models, with different modes of applications (i.e. attachment to the face) makes it possible for children or people with facial hair to apply/adapt the mode that suite them. Note the conflicting issues with present masking are the following statements:
An obvious flaw with surgical masks compared to N95 respirators is their lack of a tight face fit, which leaves gaps around the edges.
Since N95 respirators form a seal to the face, they may feel harder to breathe through than a cloth mask or surgical mask.
Typically KN95 respirators are held in place by over-ear elastic loops, rather than behind the head elastics. This can result in a weaker seal. Although recently, there are methods for tightening it with products called “ear savers”.
With regards to issues “a”, “b” and “c” above, notably with the proposed IJN (a.k.a. AIBE) models, there are no differences in their modes of fixing (i.e. attachment to the face). In particular, the complete barrier face covering frame is designed to have nasal opening and mouth opening, such that, optionally, (fabric materials or polypropylene materials etc.), can be fixed on the nasal opening and (fabric mouth cover or polypropylene mouth cover etc.) can be fixed on the mouth opening. Thus if the fabric nasal materials and fabric mouth covers are used it serves as cloth masks while if the polypropylene nasal materials and polypropylene mouth covers are used it serves as N95s respirators, etc.
Note: It will be easier to produce various options of the proposed IJN (a.k.a. AIBE) particulate respirators models because it only entails change of the mold to form any desired configuration using either natural fibers or synthetic thermoplastics to produce “non-woven polypropylene” i.e. spun-bonded polypropylene- a fabric or structure in the category of non-woven textile materials or the melt-blown and spun-lace materials.
The overall concept is articulated as follows:
- Using detachable single nostril design (round or oval shaped) or small threaded tubes, with disposable air filter material in form of buttons, a device that will freely inhale/breath in fresh air and comfortably expel/emits beams of waste air from the nose.
- Using detachable double nostril design (round or oval shaped) or small threaded tubes with disposable air filter material in form of buttons, a device that will freely inhale/breath in fresh air and comfortably expel/emits beams of waste air from the nose.
- Using fixed in-built air channel design for either single nostril design or double nostril design.
- Using threaded or screwed- in tubular air filter channel design for either single nostril design or double nostril design.
- Using press-in or plug- in or push-in tubular air filter channel design for either single nostril design or double nostril design, a device that also allows for administering inhaler through the nose to control running-nose and catarrh.
- Using one size fits all design i.e. multi-nose (complete or brief sizes) shape design or universal-nose shape design i.e. that can be used by any human nose type e.g. rounded, pointed, hooked, etc.
- Using specific nose type design (complete or brief sizes) i.e. that can be used by specific nose type e.g. rounded, pointed, hooked, etc., a device that can replicate the wearer’s exact original nose or exact preferred nose.
- Using specific nose type design (complete or brief sizes) i.e. that can be used by specific nose type e.g. rounded, pointed, hooked, etc., a device that can also exclusively fit different fabrics to match the dress wore i.e. uniform for any purpose/function or match individual attire.
- Using specific nose type design with provision to attach small transparent mouth shields, mouth covers when necessary via button/button holes or Velcro.
- Using specific mouth type design i.e. mouth cover or mouth pad or mouth cup for talking i.e. padded with fabric air filter material or air filter foam.
- Using specific mouth type design i.e. mouth cover with provision to attach a straw for drinking/liquid intake, mouth clips or lips clips for eating solid food, mouth mask for talking, etc. which is made with either zip or flip-up cover like button.
- Using brief sizes designs of the nose covers that can be coupled to the eyeglasses frame or the combined nasal shield and mouth shield configuration that can be coupled to the eyeglasses frame.
Note: One of the anticipated shortfall of the masks that unzip to allow for food or straws is the issue of touching a shared surface more often than you would have otherwise, grabbing a straw, and then guiding it into your mouth, both of which leads to upping your potential risk of transmission.
The IJN (a.k.a. AIBE) modeled mouth mask for eating and drinking eliminated the above problems in the following ways:
- By using zip openers that can be grabbed to zip-open or zip-close without the hand touching the fabric material of the mouth mask. It is applicable to either the straight zipping patterns or U-shaped zipping patterns.
- By using handles attached to one side of the flip mouth sheet (right, left, upper or down) that can be twisted to roll-open the flip-mouth sheet without the hand touching the fabrics of the mouth mask.
- By using an overlapping zipping patterns with hooks such that the hook handle is grab and pulled up to release the flip mouth sheet or to hang it at will, without the hand touching the fabric material of the mouth mask.
Note: There are lots of other options to achieve the above. It all depends on the type of material (woven cotton fabric masks and non-woven polypropylene fabric) used for the mouth mask and the type of mask (respirators or face mask) Alternatively, the mouth mask for eating and drinking could be a customized separate item (with mouth shape opening), such that when it is needed, the IJN (a.k.a. AIBE) model exclusive mouth mask will be temporarily removed and replaced with the IJN (a.k.a. AIBE) model exclusive eating and drinking mask. Subsequently, after the meal or drink, they are exchanged once more.
Note, with these designs there is no need to touch the face of the mask to remove it. Rather, it is held by the belt or Velcro (or even standard ear loops/hooks) or plasters etc., to put it on for eating or to pull it off after eating. Then subsequently the regular mouth mask or respirator is replaced for the daily routine. It is just a meal time substituted mask that is very simple and easy to use on board commercial transportations such as inside the airplanes, trains, buses and ships; in restaurants; and in other public events. For the new model it simply entails detaching the mouth mask or mouth shield and attaching the mouth eating and drinking cup or cover etc.
Note also that the model will often come as a package with the entire separate items inside. Thus depending on the situation, at any time, the wearers have the option to use/ wear the desired at the appropriate time e.g. single (nose filter only, mouth cover only or goggles only); double (nose filter and mouth cover combined, goggles and nose mask combined or goggles and mouth mask combined); triple (wearing the nose mask, mouth mask and goggles at the same time either separately or via a complete frame).
Conclusion
According to the distance above sea level (altitude- as well as the air composition, temperature, and pressure), the earth’s atmosphere is divided into five layers (troposphere, stratosphere, mesosphere, thermosphere, and exosphere) in increasing order, of which the “troposphere” is the only layer with the suitable air for use in “photosynthesis” by terrestrial plants and “breathing” by terrestrial animals.
The normal atmosphere air is a mixture of gases, that is commonly modeled or typically quoted in terms of dry air (without water vapor)” composition. It varies from one place to the next (according to geographical location and also where it occurs in the air column) and even varies depending on whether it is day or night. On the average it contains nitrogen (N2 = 78.084%), oxygen (O2 = 20.9476%) and argon (Ar = 0.934%) as the three main components of the atmosphere. The trace gases includes the noble gases neon (Ne = 0.001818%), helium (He = 0.000524%), krypton (Kr = 0.000114%), and xenon (Xe = 0.0000087%), as well as some greenhouse gases carbon dioxide (CO2 = 0.04%), methane (CH4 = 0.0002%), nitrous oxide {N2O - 0.5 parts/ million (PPM)} and ozone {O3 = 0.000007% i.e. 0 to 0.07 parts/million (PPM))} and the other gases such as hydrogen (H2 = 0.00005%), Iodine {I2 = 0.000001% i.e. 0.01 parts/ million (PPM))}, Carbon monoxide {CO - 0 to trace (PPM))}, ammonia {NH3 - 0 to trace (PPM))}, nitrogen dioxide {NO2 = 0.000002% i.e. 0.02 parts/million (PPM))}, and sulfur dioxide - SO2 - 1.0 parts/million (PPM)). Also contains a variable amount of water vapor (H2O), which on average is around 1% at sea level and 0.4% over the entire atmosphere. Water vapor accounts for roughly 0.25% of the atmosphere by mass. “The concentration of water vapor (a greenhouse gas) varies significantly from around 10 PPM) by mole fraction in the coldest portions of the atmosphere to as much as 5% by mole fraction in hot, humid air masses.
Usually, in addition the atmosphere (troposphere region) gets supplied every minute with more natural or anthropogenic (caused by human) particles or particulates {also known as atmospheric aerosol particles, atmospheric particulate matter, particulate matter (PM) or suspended particulate matter (SPM)}, a mixture of solid particles and liquid droplets. PM-refers to inhalable particles composed of sulphate, nitrates, ammonia, sodium chloride, black carbon, mineral dust or water, etc.
Overall the pollutants include chemicals and industrial pollutants such as chlorine and its compounds, fluorine and its compounds, elemental mercury vapor, sulfur dioxide, and hydrogen sulfide. Other components of the atmosphere include spores, particulates like dust and ash (e.g. volcanic ash), and biological matter, like pollen and bacteria and salt from sea spray Some particles, such as dust, dirt, soot, or smoke, are large or dark enough to be seen with the naked eye. Others are so small they can only be detected using an electron microscope. Hence, they are distinguished by their aerodynamic diameter as PM10 {a.k.a. coarse particles-10 micrometers (μm) and smaller (i.e. 10000 nm or less)} and PM2.5 {further distinguished between as fine particles, with a diameter of 2.5 μm or less (i.e. 2500 nm or less); and ultrafine particles (UFP), with a diameter of 100 nm or less (less than or equal to 0.1 micrometer); and soot}.
The greatest source of particulate matter around the home is generally the combustion of polluting fuels (e.g. firewood and other biomass), while in the ambient; the finer particles are derived from primary sources (e.g., combustion of fuels in power generation facilities, industries or vehicles) and secondary sources (e.g., chemical reactions between gases). Hence, particle pollution is produced by a wide variety of natural and manmade sources. This implies that both ambient (outdoor environments) and household (indoor) air pollution can come from similar processes such as incomplete combustion of fuels or chemical reactions between gases. However, the specific source of the combustion process can vary. For example, household activities such as boiling water for bathing or cooking or preparing animal fodder, space heating and water heating with dirty technologies, brewing beverages, and lighting with kerosene, emits a range of health harmful pollutants indoors (household air pollution exposures), while activities such as high temperature combustion in traffic and transportation (e.g. vehicles, aviation, shipping, etc.), industrial activities and power generating facilities, construction sites, waste burning, fires or fields, etc. contribute to ambient air pollution.
The average person breathes in about 16,000 quarts of air per day. Each quart contains some 70,000 visible and invisible particles (That’s over a billion particles per day that our lungs have to filter out!). Approximately 98-99% of all particles by count are in the size range of 5 microns or less, while the majority of harmful particles are 3 microns or less in size. On the other hand, the molecular size of viruses that have proven to be harmful or deadly to humans range between 0.005 to 0.3 microns (i.e. 5 to 300 nm), the average for coronary viruses in particular is about 0.125 microns i.e. 125 nm (though it varies between 0.06 micron and 0.14 micron in diameter i.e. 60 nm and 140 nm). Smaller viruses exist according to scientists, but whether they are a risk to mankind or not, have yet to be determined. Comparatively, different types of experimental measurements reported molecular Size of oxygen O2 as 0.0005 microns (0.5 nm), CO2 0.00065 microns (0.65 nm) and stated that O2 has a slightly smaller diameter than N2 {the difference is size between O2 and N2 is very small, only about 0.3 times 10 to the -10th meters (0.00000000003 meters)}. This means the size of oxygen molecule is 250 times smaller than Corona virus.
When we breathe in, we inhale the same mixture of gases contained in the atmosphere as our nose cannot filter out the oxygen from other gases. A N95 mask has pore size of 0.1 micron (100 nm), although pore size also varies up to 300 nm. A mask with pore size of 100 nm or 0.1 micron can easily allow oxygen molecules (0.5 nm or 0.0005 microns) and other gases (e.g. CO2 0.00065 microns or 0.65 nm and N2) but not particulate matters {fine particles that has the size of less than 2.5 micrometer/microns (0.00025 cm) i.e. 2500 nm or less} and corona virus (0.125 microns or 125 nm) as well. This simply means that molecule of oxygen, nitrogen and carbon dioxide, will freely get through the mask to enable the body receive the oxygen it needs. The amount of so inhaled air contains 21% of oxygen and 0.04% of carbon dioxide, while the air we breathe out contains 16.4% of oxygen and 4.4% of carbon dioxide. The composition of the nitrogen exhale remains almost the same as the nitrogen we inhale, only the percentage of carbon dioxide and oxygen changes. Essentially, viruses are never naked in air or on any dry surface. They are contained in water based droplets (of size larger than 1 micron i.e. 1000 nm). Such droplets are actively filtered by masks (100 nm to 300nm). Simply put when we cough or sneeze, viral particles are contained in fluid droplets, and it’s the droplets that make it possible to trap the virus i.e. the droplets make it possible for masks to have some effect, never 100%.
Several research investigations globally revealed that urban air quality (a.k.a. ambient or outdoor) and indoor air pollution are two of the world’s worst toxic pollution problems. Precisely, they presumed that more than 99% of the global population lives in areas where the air pollution is above the World Health Organization (WHO) air quality guidelines, and (WHO) specifically, reported that 9 out of 10 people worldwide breathe air containing high levels of pollutants . Furthermore, WHO estimated that 7 million premature deaths annually are linked to air pollution, with most deaths in developing countries and researcher in Catalonia concluded that the mortality rate from air pollution is eight times larger than the mortality caused by car accidents each year and proclaimed that, on a local level, 3500 deaths a year are caused by air pollution in Catalonia. Recently, other researchers stated that worldwide exposure to PM2.5 contributed to 4.1 million deaths from heart disease and stroke, lung cancer, chronic lung disease, and respiratory infections in 2016 and that, ambient particulate matter ranks as the sixth leading risk factor for premature death globally. Specifically, WHO reported that, about 4.2 million deaths are attributed to ambient air pollution each year while 3.2 million people die prematurely from household air pollution every year, because around 2.4 billion people cook and heat their homes with polluting fuels (e.g. firewood and other biomass).
Different areas may have different sizes of fine particle sizes. The size of particles is directly linked to their potential for causing health problems. Fine particles (PM2.5) pose the greatest health risk. These fine particles can get deep into lungs and some may even get into the bloodstream. When fine particles successful pass through the nostril and enter the lung, it will be deposit on the alveoli and causing long term effect. Some individual who have constant exposure without protection can even suffer from cardiac pulmonary disease causing sudden lung and health failure. Especially, the pollutants in the form of particulate matters (PM), smog, dust, carbon monoxide (CO), ozone (O3), nitrogen dioxide (NO2) and sulfur dioxide (SO2), etc. have the ability to penetrate deep into the lungs and brain from the blood streams, causing health problems. Coarse particles (between PM10 to PM2.5) are of less concern, although they can irritate a person’s eyes, nose, and throat.
Presently, the principal public health method of preventing and controlling the hazardous effects of air-borne pollutants such as microorganisms (viruses) and particulate matters (PM), are pharmaceutical interventions (particularly vaccination) and non-pharmaceutical interventions (include the use of surgical and non-surgical face masks and other personal protective equipment-PPE, face shields, goggles, etc.). However, prolonged wearing of the existing configurations of face masks and respirators can lead to numerous health issues such as self-contamination by the wearer from both inside and outside, including via contaminated hands, and other logistical, physiological, psychological, social and economic complications. This includes (i) the continued/repeated re-inhaling of some fractions of the wearer’s previously expelled breath, possibly contaminated with some fractions of the odor/gas from the mouth, in the confined space within the barrier face covering (i.e. re-breathing our own exhaled) carbon dioxide (CO2) instead of fresh oxygen; (ii) Uncomfortable eyes and variable vision due to mask associated dry eye (MADE) and foggy eyeglasses issues; (iii) Discomfort and irritation around the region of the nose and mouth, such as red marks; etc. A barrier faces covering, as described in “American Society for Testing and Materials (ASTM)” F3502-21 is a product worn on the face specifically covering at least the wearer’s nose and mouth, with the primary purpose of providing “source control” and to provide a degree of particulate filtration to reduce the amount of inhaled particulate material. By this simple definition, it incorporates the uses of both surgical and non-surgical respirators and face masks. In reality, they are simply distinguished as particulate respirators (either valve- or non-valve-) and particulate face masks or technically distinguished as surgical respirators; non- surgical respirators, medical/surgical face mask, and non- surgical/medical face mask (i.e. cloth/homemade face mask). They differ by their configuration type and effectiveness of filtering infectious particles and waging droplets via inhalation and exhalation or simply their intended uses and levels of protection. In all, the basic, “regulatory standards require that the face barrier covering should not permit blood or other potentially infectious materials to pass through to or reach the wearer’s skin, eyes, nose, mouth, or other mucous membranes under normal conditions of use and for the duration of time that the protective equipment will be used.” Air pollution health problem is global; hence from the following (a) The public/general health point of view, (b) Based on the defined motive for those items (respirators/ face masks) and (c) severity of particles contaminants in the air humans breathe, wearing of barrier covering should mandatorily be used by individuals who have symptoms of respiratory infection such as coughing, sneezing, or, in some cases, fever. Furthermore it should be made compulsory in construction companies, cement production factories, asbestos companies, coal industry, petroleum industry, paint factories, fertilizer companies, chemical companies, etc. Ordinarily even when there is no pandemic outbreak the use/wearing of face coverings should be mandatory in public places or gatherings e.g. classrooms in schools and universities, churches and Islamic centers, barracks, markets, political rallies, senates and house of assembles, amusement parks, wedding and entertainment halls, inside transit transportations such as airplanes, ships, trains, buses and taxi, etc. On the other hand, in periods of outbreaks: fully vaccinated and non – vaccinated people should continue to wear barrier face coverings: both indoor public places and outdoors such as crowded events or large gatherings, to drastically reduce transmission of virus as well as reduce drastically the hospitalization and mortality associated with inhaling polluted air.
Just as natural selection has shaped the evolution of humans, plants, and all living things on the planet, natural selection shapes viruses/plague which has been a reoccurring feature in human life for centuries starting from the 6th century (named the Plague of Justinian after emperor Justinian 1), such as the 1347 infamous pandemic of bubonic plague (a.k.a. Black Death) and the 1918 pandemic flu/Spanish flu also known as the Great Influenza epidemic or the 1918 influenza pandemic. Hence, the origin of surgical mask also referred to medical mask could be traced to the use of beaked masks that plague doctors wore during the 17th-century (1600s) plague epidemic, which lead to the introduction of mouth and nose coverage (mouth protection, face veils, face masks, mouth bandages) for doctors use during surgical operations, in the 1800-1900 (i.e. 19th to 20th-century). So far the face mask in use for COVID-19 (i.e. December 2019 to date- July 2023) has been the same type introduced since 1918 influenza, with very little modification such as the present advanced surgical masks and surgical N95 respirators that healthcare workers use today. Hence the desire in this work is tore-configure the face barrier coverings in diverse forms (demarcated configuration face masks), to remedy most of the short coming (physiological and psychological convenience, social and economic implication, health complications, etc.) of the present configuration of face mask used globally within the medical environments and the general public.
All the categories of barrier face coverings gadgets in use, ever since, are being made from variety of materials that are not flammable, which fall into two major categories-woven materials e.g. woven cotton fabric (made of multiple layers) and non-woven materials (polypropylene) made of either natural fibers or synthetic thermoplastics. The most common are spun-bond, melt-blown and spun-lace materials.” Overall, these materials prevent 79 per cent to 99.97 per cent (level of filtration) of mouth bacteria in particles of all sizes reaching the environment during coughing or talking. The current designs of many of the cloth masks in use are usually made with several types of reusable gauze or woven cotton and are likely producing dual levels of filtration to the person wearing them. That is, they have the ability to protect against inhaled particles and also resist fluids and limit the dispersion of exhaled properties. Alternative face masks for special situations are either clear masks or cloth masks with a clear plastic panel that may be helpful when interacting with certain groups of people, such as deaf or hard of hearing.
The proposed IJN models of barrier face coverings gadgets are configured to isolate the operations of the nose, mouth and eyes as nature intended, thereby eliminate or control most of the health issues associated with re-breathing CO2, mask associated dry eye “MADE”, bacteria phenomena, red marks/bruised face and other inconveniences/irritation on the face (around the nose, mouth and eye) experienced with wearing the present models of surgical/medical masks, cloth/homemade masks, surgical/non-surgical respirators and face shields. Of special benefit and interest is the fact that it is configured as an ornamental wear, to be used as a regular make-up dressing gadget much like the wrist watches, ear rings, sun glasses, ankle bangles or anklets, beads, neck-lace or neck chains, etc., such that it serves dual purposes. Firstly it protects the wearer 24/7 from inhaling any form of air borne particulates and pollutants (including viruses, bacteria, smoke, dusts, etc.) and secondly serves as beautifying cosmetics (e.g. used in place of cosmetic surgery or enable an individual to appear in any shape of nose he desires at any time, such as pointed, flat, round, etc.). Some could be soaked to produce refreshing aromas if desired in any particular environment.
The filter sections/areas of the IJN models demarcated configuration face barrier coverings/masks are made (produced/fabricated) with the same types of materials used to make the existing face masks and respirators, such as wool felt, fiberglass paper, or polypropylene, plastics, rubber or latex, polyurethane, woven cotton fabrics (at least 100 threads per inch); flannel (either cotton or poly-cotton blend- at least 90 threads per inch; tea towel material; cotton T-shirt material; or their combination, etc., as recommended by the World Health Organization (WHO). It is aimed at making, the wearing of air-borne pollutants protective gadgets part of human beings regular dressing mode with little or no discomfort and does not affect face recognition issues. In addition, it can be made with bio-cellulose, hydro- gel, nano-materials: that make it look natural instead of concealing face of the wearer as in the case of the present designs. Notably, it can be attached to the face in a variety of ways, for instance, they may be clipped to the nose or hooked to eyeglasses or attached to the ear with elastic rope, or fasten it behind the head with Velcro, belt, button, ear handle, or gummed to the sides of the nose or mouth with stickers, plasters, flash bands, etc. to improve on the cosmetic/ aesthetics appearance. The designs as reflected in figures 40 to 51 are not the perfect real finished fittings rather it illustrates the ideal concepts. In comparison, wearing the present configuration of particulate face masks that are loosely fitting makes the exhaled air go into the eyes (generates tear from the eyes, which gradually dries the eye as well as develop fogs on eyeglasses), while this proposed sole nose cover or mouth cover options, is an automatic source control for mask associated dry eye and foggy eyeglasses (i.e. zero mask associated dry eye and foggy eyeglasses); carbon dioxide (CO2) re-breathing (is eliminated or significantly reduce to maintain the human tolerable limit, depending on the particular model applied), etc. Precisely, since the nose mask is configured to cover only the nose region, it has zero possibility of directing the flow of the exhaled air over the eyes or retaining exhaled air in a confinement. Effectively, the cost of using the new IJN models is expected to be 0.5 % (1/2) i.e. half the cost of using the present face masks or N95s respirator masks within the same period.
References
-
(2023) Atmosphere of Earth. Wikipedia.
-
https://www.windows2universe.org/earth/ Atmosphere/images/stratosphere_diagram_big_jpg_ image.html 17/3/2023.
-
https://www.google.com/imgres?imgurl=http:// geologycafe.com/oceans/images/atmosphere_energy. jpg&imgrefurl.
-
(2023) Air Mass Flow Meter and Compressed Air Flow Meters. Sage Metering.
-
(2023) Air-Composition and Molecular Weight. Engineering tool box.
-
(2023) Composition of Normal Air. columbia.edu.
-
(2023) Background. Conde Engineering.
-
(2023) composition of normal air. Bing images.
-
(2023) Name the components of air with their approximate percentage by volume in air. Does the percentage by volume of each component remain the same, in the atmosphere of different parts of the world? Explain with reasons. Brainly.
-
(2023) Soot. Wikipedia.
-
(2022) Common Particles and Their Sizes in Microns.
-
(2022) Particle (Contaminant) Size Chart in Microns.
-
Howard J (2020) Particle sizes for mask filtration.
-
(2022) Particle sizes for mask filtration. fast.ai.
-
(2023) Particulate Matter (PM) Basics. US EPA.
-
(2023) Nanotechnology. National Geographic.
-
(2023) Particulates. Wikipedia.
-
(2022) Particle (Contaminant) Size Chart in Microns. Portable water filters.
-
Azzari C, Baraldi E, Bonanni P, Bozzola E, Coscia A, et al. (2021) Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Italian Journal of Pediatrics 47(198).
-
(2023) Respiratory Syncytial Virus (RSV). Pfizer.
-
(2023) What You Should Know About RSV in Babies. healthline.
-
(2023) Respiratory syncytial virus vaccine. Wikipedia.
-
(2023) Can Masks Capture Coronavirus Particles. Smart air filters.
-
United States Environmental Protection Agency (2023) Particulate Matter (PM) in New England. Air Quality Planning Unit New England US.
-
https://www.bing.com/newtabredir?url=https%3 A%2F%2Fwww.vectorstock.com%2Froyalty-free- vector%2Finfographics-pollution-human-activity- vector-2245158
-
(2023) PM2.5 Bound Metals and Their Associated Health Effects. Science Trends.
-
World Health organization (2023) Air quality and health.
-
United States Environmental Protection Agency (2023) Health and Environmental Effects of Particulate Matter (PM). Health Effects.
-
United States Environmental Protection Agency (2023) How Does PM Affect Human Health. Air Quality Planning Unit New England.
-
United States Environmental Protection Agency (2023) Health and Environmental Effects of Particulate Matter (PM). Health Effects.
-
(2021) Buildings as Filters: Capturing air pollution. IAAC Blog.
-
Bloss W (2014) environmental-brief-no-4-2014_tcm18- 237725.pdf
-
(2023) Harmful Effects of PM. Bing images.
-
https://www.bing.com/newtabredir?url=http%3A%2F %2Ftechalive.mtu.edu%2Fenvengtext%2Fch12_health. html.
-
Free Respiration Cliparts, Download Free Respiration Cliparts png images, Free ClipArts on Clipart Library (clipart-library.com)
-
(2017) Chemical handling. ppt. slide share.
-
(2022) Respiratory System Diagram, Respiratory System Anatomy | Respiratory system anatomy, Respiratory system, Human body systems (pinterest.com)
-
Lakna (2017) Difference between Internal and External Respiration. Biology.
-
Buildings as Filters: Capturing air pollution – IAAC Blog
-
https://www.bing.com/newtabredir?url=https%3A%2 F%2Fwww.lalpathlabs.com%2Fblog%2Fhealth-effects- of-air-pollution%2F
-
Janolo H (2023) What is the initial energy form of coal. Coal.
-
How coronavirus is transmitted - Bing images.
-
(2021) The A-Z Guide Of Soldering Fumes Health Effects (Updated). Fixitman blog.
-
Axe D (2022) New Mutant Omicron Feared to Be the Most Contagious Variant Yet. Knight Lab.
-
Mara L (2021) How to solve common face mask problems-from foggy glasses to irritated ears. Business Insider.
-
Korab A (2020) 8 Side Effects of Wearing Face Masks- Eat. This Not That.
-
Li Y (2005) Effects of wearing N95 and surgical facemasks on heart rate, thermal stress and subjective sensations. Int Arch Occup Environ Health 78(6): 501-509.
-
Wilkinson L (2020) Full-time mask-wearing brings its own set of problems. The Crimson White.
-
Kisielinski K (2021) Is a Mask That Covers the Mouth and Nose Free from Undesirable Side Effects in Everyday Use and Free of Potential Hazards. Int J Environ Res Public Health 18(8): 4344.
-
Desai AN, Mehrotra P (2020) Medical Masks. Infectious Diseases JAMA 323(15):1517-1518.
-
Hill DG (2020) From the Frontlines: The Truth About Masks and COVID-19. American Lung Association.
-
(2021) Health Freedom Idaho. Serious Concerns Over Masks and Carbon Dioxide Levels.
-
Walsh K (2020) Mask Associated Dry Eye (MADE): Why does it happen and what can you do. Core University of Waterloo.
-
Porter KK Burshnic VL (2020) Optimizing Effective Communication While Wearing a Mask During the COVID-19 Pandemic. J Gerontol Nurs 46(11): 7-11.
-
Marler H, Ditton A (2021) I’m smiling back at you”: Exploring the impact of mask wearing on communication in healthcare. Int J Lang Commun Disord 56(1): 205-214.
-
Afrikanza (2020) African Masks Examined: History, Type, Role, Meaning & Examples. Afrikanza Culture & History.
-
Wingert PS (2022) mask. Definition, History, Uses, & Facts Britannica.
-
(2013) A History of the Anonymous Mask. Dazed Text Angus Griffin.
-
OnStage Blog (2020) The Origins of the Comedy and Tragedy Masks of Theatre. OnStage Blog.
-
(2022) Masks in Greek Theatre. History of Greek Theatre.
-
(2022) Masks: Reflections of Culture and Religion. Culture Library.
-
Carstairs C (2020) A Brief History of Masks, Through Plagues and Pandemics. The Tyee Independent
-
Journalism that swims against the current.
-
(2022) History-Plague Masks.
-
Clarke R (2022) Bubonic Plague: Why a Doctor Invented the First Face Mask. by Regina Clarke Medium.
-
(2022) The Plague Doctor Mask. A History VIVO Masks.
-
(2020) Long Before PPE Suits: Why Did Bubonic Plague Doctors Wear Those Strange Beaked Masks. Buzz News 18.
-
(2020) A brief history of masks from the 17th-century plague to the ongoing corona virus pandemic. The concversation Academic rigour, journalistic flair.
-
Harris J (2018) The 1918 Flu Pandemic. Origins.
-
(2022) Spanish flu. Wikipedia.
-
Martingano S (2022) The 1918 Spanish Flu: Only The Vaccinated Died. Ficpa.
-
Wei H (2020) A Brief History of Face Masks in China. Sixth tone.
-
Williams C (2020) Looking back: The history of medical masks and today’s parallels to prior pandemics. KSL news.
-
Matuschek C, Friedrich M, HeinerF, Johannes CF, Zanker K (2020) The history and value of face masks. Eur J Med Res 25(1): 23-24.
-
Types of Masks and Respirators. CDC.
-
(2023) N95 vs FFP3 & FFP2 masks - what’s the difference. Fast life hacks.
-
The Canadian Shield (2020) Procedural Masks vs Surgical Masks: What’s The Difference. The Canadian Shield.
-
Mertes A (2022) What Are the Different Types of Face Masks & Which One is Best.
-
Image of the melt-blown filaments under microscope. MDPI.
-
Leung NH, Daniel KWC, Eunice YCS, Kwok Hung C, Mc Devitt JJ, et al. (2020) Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat Med 26(5): 676-680.
-
Robertson P (2020) The Ultimate Guide to Homemade Face Masks for Corona virus. Masks Clean Air Blog.
-
Image via. Smart air filters.
-
Image from the masks 4all. co. DIY mask project.
-
Kurt S (2020) Maker Mask launches in Seattle using 3D-printing technology to produce protective gear. Geek Wire.
-
(2020) The Protective Mask Produced By Boeing Is Officially Delivered, 3D Printed And Reusable. 3D Printers News Shaoxing Xinshan Science Technology Co. Ltd.
-
(2020) Free 3D Printable Resources for COVID-19 Prevention. Blog CGTrader.
-
(2023) new nasal illness defender mask. Bing images.
-
Jennifer NJ (2018) People Are Now Wearing Nose Warmers. Simplemost.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria