Post-Acute Covid-19 in General Medicine: A Clinical- Epidemiological Reporting of 33 Patients from March 2020 to March 2021 in Toledo (Spain)
Background: Although many of SARS-CoV-2 infected recover without complications, some have a prolonged illness, but the evidence for their characteristics is limited. Objective: To study in general medicine clinical-epidemiological characteristics of patients with post-acute COVID-19 syndrome (persistent symptoms and/or delayed or long-term complications beyond 4 weeks from the onset of symptoms). Methodology: An observational, longitudinal and retrospective case series study of patients with post-acute COVID-19 syndrome, based on a prospective cohort of COVID-19 patients in a family medicine office in Toledo (Spain) was carried out from March 15, 2020 to March 31, 2021. Results: 33 patients were included, 58% were women. Mean age was 54 years. All but one was symptomatic in the acute phase. Half of the patients required sick leave, 51% had moderate-severe severity in the acute phase and 42% required hospitalization. 54% had at least one chronic disease, predominantly endocrinological with 21% and cardiovascular with 19%. The main symptoms in the post-acute phase were: 36% general (discomfort, asthenia, myalgia, and fever), 32% respiratory symptoms (cough, dyspnea, chest pain), and ENT symptoms (anosmia/ageusia, odynophagia, rhinorrhea, dryness and pharyngeal mucus) 14%. There were no statistically significant differences between symptoms in the acute phase and the post-acute phase. 14 new health problems were diagnosed in the 33 patients during the post-acute period: oral candidiasis, bacterial endocarditis, 2 diabetes mellitus type 2, pathological grief, limb tremor, myopathy, lower limb deep vein thrombosis, angina pectoris, atrial fibrillation, pulmonary embolism, gallstones, acute gout, and renal colic. Conclusion: In the context of general medicine in Toledo (Spain), patients with post-acute COVID-19 are predominantly women, with mean age of 54 years, with previous chronic endocrinological and cardiovascular diseases, which presented moderate-severe severity and frequently required admission hospital, with general and respiratory symptoms, both in the acute and post-acute phases, with no differences between the two.
Introduction
The coronavirus disease (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS- CoV-2), was first reported in China in December 2019 [1] and spread rapidly in many countries. The first case of coronavirus disease 2019 (COVID-19) in Spain was confirmed on the 31st of January (an imported case). Subsequently, new cases were detected in other Spanish regions and a rapid spread was observed. Spain declared a state of alarm in March 13, 2020 [2, 3, 4, 5].
Common symptoms in the acute phase include cough, fever, dyspnea, musculoskeletal symptoms (myalgia, joint pain, and fatigue), gastrointestinal symptoms, and anosmia/ dysgeusia [6, 7, 8, 9]. But, data is emerging that many patients have long-lasting symptoms, several months after initial infection with COVID-19 [10]. However, information is lacking on these symptoms that persist after recovery. When it comes to strategies for the COVID-19 pandemic, doctors and politicians often discuss infection and death rates, effects on children and adolescents, or socioeconomic effects. The long-term consequences of COVID-19 receive little attention, although they are of considerable importance for those affected, for the health system and for the entire economy [11].
People living with “Long Covid” around the world describe a complex and multifaceted condition that involves a variety of physical, cognitive, psychological and social implications, and although there is an emerging recognition of Long Covid, the evidence base is limited and fragmented and many research questions remain. Thus, one of the priorities is epidemiological studies to define the clinical presentations of Long Covid and the impact of comorbidities. Reorienting and including Long Covid in existing cohorts, trials, and studies could be the most efficient way to conduct this research [12].
In this context we present an observational, longitudinal and retrospective cases series study of patients with post- acute COVID-19 syndrome, based on a prospective cohort of COVID-19 patients in a family medicine office in Toledo (Spain), with the aim of studying the clinical-epidemiological characteristics of patients with post-acute COVID-19 syndrome (persistent symptoms and/or delayed or long- term complications beyond 4 weeks from the onset of symptoms) in general medicine.
Material and Methods
Design and Emplacement
An observational, longitudinal and retrospective case series study of patients with post-acute COVID-19 syndrome, based on a prospective cohort of COVID-19 patients was carried out from March 15 , 2020 to March 31, 2021, in a family medicine office in the Health Center Santa Maria de Benquerencia, Toledo (Spain), which has a list of 2,000 patients> 14 years of age (in Spain, the general practitioners [GPs] care for people > 14 years of age, except for exceptions requested by the child’s family and accepted by the GP).
Diagnosis of COVID-19
The diagnosis was performed with reverse transcriptase polymerase chain reaction (PCR) oropharyngeal swab tests or antigen testing. Spain had not initially devised an intensive testing strategy for suspected cases of COVID-19 infections [13]; since the beginning of the pandemic in mid-March 2020, PCR tests were only performed in the hospital context until mid-May 2020, when they began to be performed in general medicine as well. In mid-December 2020, rapid antigen tests began for symptomatic patients with less than 5 days of evolution. The PCR tests were performed both in symptomatic patients and in asymptomatic contacts. A symptomatic confirmed case with active infection was considered to be any person with a clinical picture of sudden onset acute respiratory infection of any severity that occurs, among others, with fever, cough or feeling of shortness of breath. Other symptoms such as odynophagia, anosmia, ageusia, muscle pain, diarrhea, chest pain or headache, among others, were also considered symptoms of suspected SARS-CoV-2 infection according to clinical criteria; and a positive PCR or rapid antigen test positive [14].
Diagnosis of Post-Acute COVID-19
It was defined as a syndrome characterized by persistent symptoms and/or late or long-term complications beyond 4 weeks from the onset of symptoms [15].
Collected Variables
Data were extracted from the medical records of the general medicine practice under study. The following variables were collected: age; sex; symptoms; chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and/or can be expected to require a long period of control, observation or treatment” [16], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD- 10 Version: 2019 [17]; social-occupancy class (according to the Registrar General’s classification of occupations and social status code) [18, 19]; complex family and low income household based on the genogram and in the experience of the general practitioner for their continuity of care and knowledge of the family (genogram was a schematic model of the structure and processes of a family, which included the family structure, life cycle and family relational patterns. It was understood that “complex” genogram identified families with psychosocial problems) [20, 21, 22, 23]; number of family members; ethnic minority; and severity of the disease (mild cases: clinical symptoms are mild and no manifestation of pneumonia can be found on images; moderate cases: with symptoms such as fever and respiratory tract symptoms, and the manifestation of pneumonia can be seen on the imaging tests; and severe cases: respiratory distress, respiratory rate ≥ 30 breaths/min., pulse oxygen saturation≤93% with room air at rest, arterial partial pressure of oxygen/oxygen concentration≤300 mmHg.) [24]. To simplify comparison, moderate and severe cases were counted together.
Sample
All patients who met the criteria for post-acute COVID-19 from March 15, 2020 to March 31, 2021 were included, and that they were seen in the consultation object of the study and their medical documentation was available.
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2) with Yates correction or Fisher Exact Test when necessary, (according to the number the expected cell totals) for percentages.
Results
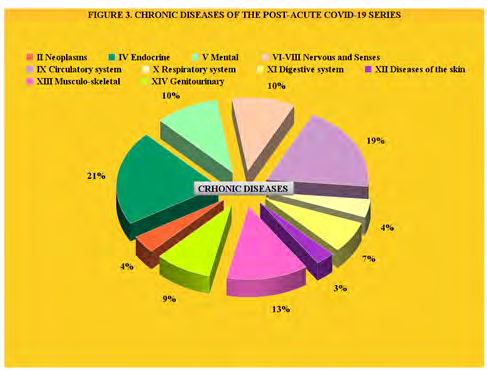
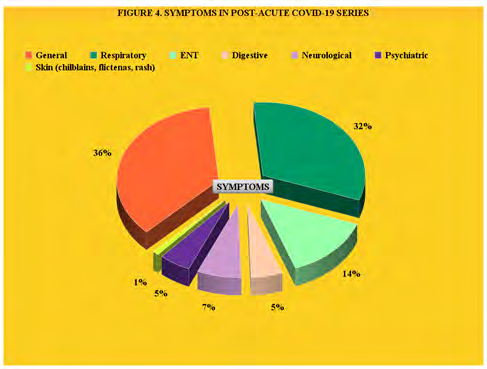
33 patients were included, 58% were women. Mean age was 54 years (Range: 20-80 years). All but one were symptomatic in the acute phase, with 33% general symptoms (discomfort, Asthenia, Myalgia, fever), 33% respiratory symptoms (Cough, Dyspnea, Chest pain), and 11% ENT symptoms (Anosmia/Ageusia, Odynophagia, Rhinorrhea, dryness and pharyngeal mucus), half of the patients required sick leave from work, 51% had moderate-severe severity in the acute phase and 42% required hospitalization. 54% had at least one chronic disease, predominantly endocrinological with 21% and cardiovascular with 19%. The main symptoms in the post-acute phase were 36% general (discomfort, asthenia, myalgia, fever), 32% respiratory symptoms (cough, dyspnea, chest pain), and ENT symptoms (anosmia/ ageusia, odynophagia, rhinorrhea, dryness and pharyngeal mucus) with 14% (Tables 1 & 2, Figures 1-4). There were no statistically significant differences between symptoms in the acute phase and the post-acute phase (Table 3). 14 new health problems were diagnosed in the 33 patients during the post-acute period: oral candidiasis, bacterial endocarditis, 2 diabetes mellitus type 2, pathological grief, limb tremor, myopathy, lower limb deep vein thrombosis, angina pectoris, atrial fibrillation, pulmonary embolism, gallstones, acute gout, and renal colic (Table 4).
| Variables | Post-Acute Covid-19 Syndrome |
|---|---|
| Age in years (Arithmetic mean + - Standard deviation; Range) | 54.21+-13.71 Range: 20-80 years |
| > = 65 years | 7 (21) |
| < 45 years | 8 (24) |
| < 18 years | 0 |
| Women | 19 (58) |
| Family with > = 4 members | 5 (15) |
| Asymptomatic | 1 (3) |
| Social-occupancy class of patients (people with some type of labour specialization) | 17 (51) |
| Sick leave | 15 (45) |
| Students | 1 (3) |
| Ethnic minority | 9 (27) |
| Low income household | 4 (12) |
| Complex family | 0 |
| Chronic diseases presence | 18 (54) |
| Moderate-severe Severity | 17 (51) |
| Hospitalization in acute phase | 14 (42) |
| Readmission after hospital discharge | 2 (6) |
| Chronic Diseases According To Who, Icd-10 Groups * | Post-Acute Covid-19 Syndrome N=33 |
| -II Neoplasms | 3 (4) |
| -IV Endocrine | 15 (21) |
| -V Mental | 7 (10) |
| -VI-VIII Nervous and Senses | 7 (10) |
| -IX Circulatory system | 13 (19) |
| -X Respiratory system | 3 (4) |
| -XI Digestive system | 5 (7) |
| -XII Diseases of the skin | 2 (3) |
| -XIII Musculo-skeletal | 9 (13) |
| -XIV Genitourinary | 6 (9) |
| TOTAL chronic diseases* | 70 (100) |
Table 1: Description of Selected Variables of the Post-Acute Covid-19 Series.
( ): Denotes percentages Table 1: Description of Selected Variables of the Post-Acute Covid-19 Series.
( ): Denotes percentages *Patients could have more than one chronic disease. The percentages are over the total of chronic disease Table 2: Description of Chronic Diseases of the Post-Acute Covid-19 Series.
| Symptoms** | Symptoms In Covid-19 Acute Phase N=33 | Symptoms In Post- Acute Covid-19 N=33 | Statistical Significance |
|---|---|---|---|
| General (discomfort, asthenia, myalgia, fever, arthralgias) | 45 (33) | 21 (36) | X2= 0.2367. p= .626581. N S. |
| Respiratory (cough, dyspnea, chest pain) | 45 (33) | 18 (32) | X2= 0.0464. p= .829454. N S. |
| ENT (anosmia / ageusia, odynophagia, rhinorrhea, pharyngeal dryness- mucus, epixtasis) | 15 (11) | 8 (14) | X2= 0.337. p= .561576. N S. |
| Digestive (anorexia, nausea / vomiting, diarrhea, abdominal pain) | 12 (8) | 3 (5) | X2 with Yates correction= 0.3054. p= .58054. N S. |
| Neurological (headache, dizziness, mental confusion -brain fog) | 13 (9) | 4 (7) | X2= 0.3284. p= .566627. N S. |
| Psychiatric (anxiety, insomnia) | 7 (5) | 3 (5) | X2 with Yates correction= 0.1066. p= .744002. N S. |
| Skin (chilblains, flictenas, rash) | 1 (1) | 1 (1) | Fisher exact test= 0.5053. N S. |
| Total symptoms** | 138 (100) | 58 (100) |
Table 2: ** Comparison of Covid-19 Symptoms in Covid-19 Acute Phase and Symptoms in Post-Acute Covid-19.
( ): Denotes percentages Patients could have more than one symptom. The percentages are over the total of symptoms NS: Not significant at p< .05. Table 3:** Comparison of Covid-19 Symptoms in Covid-19 Acute Phase and Symptoms in Post-Acute Covid-19.
| Post-Acute Covid-19N=33 | |
|---|---|
| -I Infectious | 2 (oral candidiasis, bacterial endocarditis) |
| -IV Endocrine | 2 (diabetes mellitus type 2) |
| -V Mental | 1 (pathological grief) |
| -VI-VIII Nervous and Senses | 2 (limb tremor, myopathy) |
| -IX Circulatory system | 4 (lower limb deep vein thrombosis, angina pectoris, atrial fibrillation, pulmonary embolism) |
| -X Respiratory system | 0 |
| -XI Digestive system | 1 (gallstones) |
| -XII Diseases of the skin | 0 |
| -XIII Musculo-skeletal | 1 (acute gout) |
| -XIV Genitourinary | 1 (renal colic) |
| Total New Diagnostics During The Post-Acute Covid-19 Phase | 14 |
Table 3: New Diagnostics during the Post-Acute Covid-19 Phase.
Discussion
The symptoms of Long-COVID or post-acute COVID-19 syndrome are very varied. COVID-19 can lead to a wide range of clinical manifestations, ranging from asymptomatic infection to acute respiratory distress syndrome and multi- organ failure with high mortality rates [12, 25]. It has been established that SARS-CoV-2 not only infects the respiratory tract but that subsequent viral replication and immune response also affect multiple organ systems. Although many of those infected recover without complications, some suffer from a prolonged illness [26, 27, 28, 29, 30, 31]. Long-term consequences are also possible if the disease is mild or has no symptoms [11]. It is described that, after an improvement in the acute phase, other symptoms may suddenly appear (for example, pericardial effusion); furthermore, the patient may begin to realize that something else is wrong: extreme insecurity, loss of control over mental abilities, etc. The patient may not talk to anyone about these symptoms and feel very uncomfortable; he or she may be embarrassed to speak of his complaints to the doctor, and some of those complaints may be dismissed and ascribed to a psychosomatic origin; the fear may take hold of the patient that he could no longer cope with his daily work [25].
Age
A prolonged course of the disease has been reported in adults and children, and all age groups are affected, regardless of the severity of the infection (from asymptomatic to severe) and health status [11]. Chinese researchers analyzed health data of more than 1,700 patients discharged from a hospital in Wuhan as cured between January 7 and May 29, 2020; they were 57 years old on average; three-quarters of them still had complains 6 months later [32]. In a survey on long COVID-19, about a third of those surveyed were between 40 and 49 years old, and just over a quarter between 30 and 39 and between 50 and 59 years old [27]. In another study, the mean age was 56.5 (SD, 14.6) years (range, 19-84 years). In our series of cases, data already published are repeated: we found a mean age was 54 years (Range: 20-80 years).
Sex/Gender
The post-acute COVID-19 syndrome particularly frequently affects young women, without risk factors, with a mild to moderate course in the acute phase [11, 25]. Again, our data is along the same lines, with a slight majority of women: of our 33 patients, 58% were women.
Long-COVID Clinical Picture
An analysis in the UK (10) indicated that “prolonged COVID” could be due to 4 syndromes: permanent damage to the lungs and heart, post-intensive care syndrome, post- viral fatigue syndrome and persistent COVID-19 symptoms. Researchers from the US, Sweden, and Mexico published the results of a meta-analysis of 15 studies [30]: 80% of all SARS-CoV-2 infected patients developed at least 1 long-term symptom; these included fatigue (58%), headache (44%), attention deficit (27%), hair loss (25%), and shortness of breath (24%). Certainly, a growing number of reports describe a series of fluctuating or persistent symptoms that patients experience for months after recovery from COVID-19. Symptoms include cough, fatigue, dyspnea, pain, and so-called mental confusion or “brain fog” (cognitive impairment, including confusion and memory loss) and are associated with a deleterious effect on activities of daily living [33]. In another study, patients reported tiredness (63%) and insomnia (26%) [32]. One of the first studies to describe persistent symptoms in a post-COVID cohort of patients from a hospital in Italy, 87% reported having symptoms: 53% reported fatigue, 43 % dyspnea and 23 cough, 2 months after discharge [6].
In an international survey 45% reported that they require reduced working hours compared to before the illness; the majority complained of persistent fatigue (78%) or cognitive impairment (55%). Almost half of the respondents (45%) stated that they could work less than before and a fifth could not even work [27]. Likewise, other researchers have reported that the most prevalent persistent symptoms were fatigue (92%), loss of concentration/memory (74%), weakness (68%), headache (65%) and dizziness (64%). Most of the participants reported higher levels of disability associated with shortness of breath, increased fatigue, and reduced quality of life [34].
We found that the main symptoms in the post-acute phase were 36% general (discomfort, asthenia, myalgia, fever), with 32% respiratory symptoms (cough, dyspnea, chest pain), and ENT symptoms (anosmia/ageusia), odynophagia, rhinorrhea, dryness and pharyngeal mucus) with 14%. Some experts define as manifestations of post- acute COVID-19 only those that appear in the follow-up and not in the acute phase, or if they did, they recovered [35]. In this sense, in our study there were no statistically significant differences between symptoms in the acute phase and the post-acute phase. However, based on a study that enrolled patients by tweeting (“If you consider yourself a Long-hauler, please let us know which symptoms you have experienced.”), the symptoms of post-acute COVID-19 are probably much more numerous than those currently listed [36].
Respiratory and General Symptoms
At present, many reports have described that cough can persist for weeks and months after SARS-CoV-2 infection in some patients, with varying degrees of severity of acute symptoms [33]. Cough is one of the most common presenting symptoms of COVID-19, and is reported in approximately 60 to 70% of symptomatic patients. Coughing is not only distressing for patients, but also increases the risk of community transmission by respiratory droplets.
In a multicenter observational cohort study of 1,250 COVID-19 survivors in Michigan, USA, 15% of those who responded to the telephone survey reported a new or worsening cough 2 months after discharge. Persistent cough has also been reported in patients with mild baseline severity; Cohort studies in Norway and the Faroe Islands found that about 10% of their outpatients had a cough 4 months after the onset of symptoms. In a pooled analysis, the estimated prevalence of persistent cough was found to be 18% in 14 inpatient studies.
However, the prevalence varies widely between studies and presumably depends on the characteristics of the patient, the treatment, the length of follow-up, and the definition of the results. Longitudinal studies in the general population have not been reported so far, but in the UK Office for National Statistics COVID-19 Infection Survey, cough was the second most common persistent symptom (11%), with fatigue being the first. Among the most frequent general symptoms, in addition to fatigue, 26% of the symptoms experienced by patients with post-acute COVID-19 are described as painful in a survey [36].
Neuro-Psychiatric Symptoms
While the impact of COVID-19 on the lungs and vascular system has received some medical and media attention, survey results suggest that symptoms of the brain, whole body, eyes and skin are also common health problems for people recovering from COVID-19 [36]. At the same time, specialized societies warn about neurological complaints [37]. COVID-19 is often associated with neurological symptoms during the acute phase; taste and odor disorders are typical, but headaches, muscle pain, and fatigue syndrome are also common. In addition, encephalopathies are quite common, especially in severe cases. Life-threatening neurological complications are also known during or immediately after the acute phase of infection. It is unclear whether COVID-19 could cause long-term dementia symptoms or promote the progression of neurodegenerative diseases.
Using data from a large network of electronic medical records (> 81 million patients), an estimated incidence of a neurological or psychiatric diagnosis within 6 months of COVID-19 diagnosis was 34%, with 13% of first diagnoses. Regarding individual diagnoses, the results of this study showed that the entire COVID-19 cohort had estimated incidences of 0.6% for intracranial hemorrhage, 2% for stroke, 0.1% for Parkinsonism, 0.7% for dementia, 17% for anxiety disorder and 1% for psychotic disorder, among others [38]. In our series we found that in the post-acute phase symptoms, 9% were neurological and 7% psychiatric (a total of neuropsychiatric symptoms of 16%), with two new neurological diagnoses (tremor and myopathy) and one mental (pathological grief).
Cardiovascular Symptoms
Since the beginning of the pandemic, it has become increasingly clear that SARS-CoV-2 is particularly dangerous for people with cardiovascular disease. The infection can lead to myocarditis, cause heart attack-like symptoms, cause arrhythmias, and lead to acute and chronic heart failure. Isolated cases of COVID-19 patients with stress cardiomyopathy have also been described [39]. In addition to direct infection of the heart muscle cells, the myocardium can also be damaged by a systemic inflammatory reaction. The entry of the virus into the endothelial cells that line the blood vessels leading to the heart is also documented. One consequence that is particularly important for the course of the disease is inflammation of this endothelium [40].
Because the possible consequences of systemic endotheliitis are serious microcirculation disorders of many organs, coagulation disorders, pulmonary embolisms, cerebral and gastrointestinal vascular occlusions and also a fatal multi-organ failure. Patients who already have high blood pressure, diabetes, heart failure, or coronary disease, and therefore already have endothelial damage, are particularly at risk. Other possible relevant cardiovascular consequences of a SARS-CoV-2 infection are dysregulation of the renin-angiotensin-aldosterone system and, in addition to hypercoagulability, also a destabilization of arterial plaques mediated by cytokines [41].
In a prospective cohort study of more than 1,200 COVID-19 patients, the majority had abnormal echocardiographic findings. These and other imaging findings raise the question of whether cardiac involvement is not more common than previously assumed, especially since at least 30-40% of infections are asymptomatic or undetected [42]. The truth is that to date there is no answer as to why some people are prone to serious cardiovascular complications after a SARS-CoV-2 infection, and others are not. In our series, 4 cardiovascular diseases were diagnosed during the post- COVID-19 phase: lower limb deep vein thrombosis, angina pectoris, atrial fibrillation, pulmonary embolism.
Severity of the Acute and Post-Acute Phase COVID-19
Although the risks are higher in patients who had severe COVID-19, less than 10% of the 3,762 participants in a study from 56 countries had been treated as hospitalized patients, so the post-acute COVID-19 syndrome can affect both hospitalized patients and those who did not require it [11, 26, 27, 28, 29, 30, 31]. For example, it has been reported that 7-10% of patients who recovered from COVID-19 pneumonia may develop a severe cough 2 months after discharge [43, 44]. In our series, 42% required hospital admission in the acute phase.
Comorbidities
Common comorbid conditions have been reported to be cardiovascular disease (25.1%), dyslipidemia (16.0%), diabetes mellitus (11.2%), chronic obstructive pulmonary disease (6.6%), asthma (7,5%) and cancer (5.1%) [45]. we found 54% of patients had at least one chronic disease, predominantly endocrinological with 21% and cardiovascular with 19%.
Study Limitations
Case series studies are studies of “numerators” only. No control group or controlled assignments of patients is involved. Nevertheless, aside from these inherent limitations, case study series are often good source of information [46]. The presentation of a limited number of cases indicates that these cases are probably nor unique, and that a better descriptive study might or should be attempted. Consequently, despite the fact that registries in general practice are key sources for morbidity estimates, especially if all people are registered in a general practice and if the GP is the gatekeeper of health care, the cases presented probably indicate an “incidence minimal” [47, 48].
Conclusion
In the context of general medicine in Toledo (Spain), patients with post-acute COVID-19 are predominantly women, older than 45 years, with previous chronic endocrinological and cardiovascular diseases, which presented moderate-severe severity and frequently required admission hospital, with general and respiratory symptoms, both in the acute and post-acute phases, with no differences between the two.
References
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Linden P (2020) Health confirms in La Gomera the first case of coronavirus in Spain. El Pais.
-
(2020) Ministerio de Sanidad Coronavirus (COVID-19)-08 March 2020. Madrid, Spain: Official site of the Department of National Security.
-
Turabian JL (2020) A Family Doctor’s Clinical- Epidemiological Diary in Spain of the Times of Covid-19. February 24 to March 15: Is Covid-19 A Lottery?. Epidemol Int J 4(3): 1-8.
-
Turabian JL (2020) Micro-Impact of the Pandemic by Covid-19 in the General Medicine: Clinical and Epidemiological Reflections from the Situation in Spain March 2020. Epidemol Int J 4(2): 1-8.
-
Carfì A, Bernabei R, Landi F (2020) Persistent Symptoms in Patients After Acute COVID-19. JAMA 324(6): 603- 605.
-
Docherty AB, Harrison EM, Green CA, Hardwick HE, Pius R, et al. (2020) Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterization Protocol: prospective observational cohort study. BMJ 369: 1985.
-
Wang D, Hu B, Hu C, Zhu F, Liu X, et al. (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 323(11): 1061-1069.
-
Landi F, Barillaro C, Bellieni A, Brandi V, Carfì A, et al. (2020) The new challenge of geriatrics: saving frail older people from the SARS-CoV-2 pandemic infection. J Nutr Health Aging 24(5): 466-470.
-
Mahase E (2020) Long covid could be four different syndromes, review suggests. BMJ 371: 3981.
-
Kron T (2021) Long-COVID: Infectiously recovered, but not healthy-at least every 10th patient suffers from these long-term consequences. Medscape.
-
Carson G (2021) Research priorities for Long Covid: refined through an international multi-stakeholder forum. BMC Med 19: 84.
-
Montenegro P, Brotons C, Serrano J, Fernandez D, Ramos CG, et al. (2021) Community seroprevalence of COVID-19 in probable and possible cases at primary health care centres in Spain. Family Practice 38(2): 153-158.
-
(2020) Instituto de Salud Carlos III Strategy for early detection, surveillance and control of COVID-19. Ministry of Health. Spain.
-
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, et al. (2021) Post-acute COVID-19. Nat Med 27(4): 601-615.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The CV Mosby Company.
-
WHO (2019) International Statistical Classification of Diseases and Health-Related Problems. World health Organization, ICD-10.
-
Royal Collage of General Practitioners (1986) The Classification and Analisis of General Practice Data. Occasional Paper.
-
Donaldson RJ, Donaldson LJ (1983) Essential Community Medicine. Lancaster: MTP Press.
-
Turabian JL (2017) Family Genogram in General Medicine: A Soft Technology that can be Strong. An Update. Res Med Eng Sci 3(1): 186-191.
-
Russell LT (2020) Capturing Family Complexity in Family Nursing Research and Practice. J Fam Nurs 26(4): 287- 293.
-
Watts C, Shrader E (1998) How to do (or not to do)… The genogram: a new research tool to document patterns of decision-making, conflict and vulnerability within households. Health Policy Plan 13(4): 459-464.
-
McIlvain H, Crabtree B, Medder J, Stange KC, Miller WL (1998) Using practice genograms to understand and describe practice configurations. Fam Med 30(7): 490- 496.
-
Mao S, Huang T, Yuan H, Li M, Huang X, et al. (2020) Epidemiological analysis of 67 local COVID-19 clusters in Sichuan Province, China. BMC Public Health 20: 1525.
-
Viciano A (2021) As if Corona had eaten my brain: This doctor has long COVID - how the disease changed her life and how she deals with uncertainty. Medscape.
-
Alwan N, Johnson L (2020) Long COVID: where do we start with the case definitions?. OSF Preprints.
-
Davis HE, Assaf GS, McCorkell L, Wei H, Low RJ, et al. (2020) Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. MedRxiv.
-
Ayoubkhani D, Khunti K, Nafilyan V, Maddox T, Humberstone B, et al. (2021) Epidemiology of post- COVID syndrome following hospitalisation with coronavirus: a retrospective cohort study. BMJ 372: 693.
-
(2021) Office of National Statistics. Updated estimates of the prevalence of long COVID symptoms.
-
Leon SL, Ostrosky TW, Perelman C, Sepulveda R, Rebolledo PA, et al. (2021) More than 50 long-term effects of COVID-19: a systematic review and meta- analysis. MedRxiv.
-
Michelen M, Manoharan L, Elkheir N, Cheng V, Dagens D, et al. (2020) Characterising long-term covid-19: a rapid living systematic review. MedRxiv.
-
Huang C, Huang L, Wang Y, Li X, Ren L, et al. (2021) 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 397(10270): 220-232.
-
Song WJ, Hui CKM, Hull JH, Birring SS, McGarvey L, et al. (2021) Confronting COVID-19-associated cough and the post-COVID syndrome: role of viral neurotropism, neuroinflammation, and neuroimmune responses. Lancet Respir Med 9(5): 533-544.
-
Tabacof L, Mancuso JT, Wood J, Cortes M, Kontorovich A, et al. (2020) Post-acute COVID-19 syndrome negatively impacts health and wellbeing despite less severe acute infection. MedRxiv.
-
Cotelo J (2021) Post-COVID-19 syndrome: rebound in neuropsychiatric disorders is predicted. Medscape.
-
Lambert NJ (2020) COVID-19 “Long Hauler” Symptoms Survey Report. Indiana University School of Medicine.
-
(2021) Deutsche Gesellschaft für Neurologie The five most common neurological consequences of COVID-19.
-
Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ (2021) 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry 8(5): 416-427.
-
Giustino G, Croft LB, Oates CP, Rahman K, Lerakis S, et al. (2020) Takotsubo Cardiomyopathy in COVID-19. J Am Coll Cardiol 76(5): 628-629.
-
Varga Z, Flammer AJ, Steiger P, Haberecker M, Andermatt R, et al. (2020) Endothelial cell infection and endotheliitis in COVID-19. Lancet 395(10234): 1417-1418.
-
Modin D, Claggett B, Pedersen CS, Hojbjerg Lassen MC, Skaarup KG, et al. (2020) Acute COVID-19 and the Incidence of Ischemic Stroke and Acute Myocardial Infarction. Circulation 142(21): 2080-2082.
-
Kron T (2020) Virus with dangerous “weakness” for the heart: How the corona infection affects the cardiovascular system. An overview. Medscape.
-
Mandal S, Barnett J, Brill SE, Brown JS, Denneny EK, et al. (2021) ‘Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax 76(4): 396-398.
-
D’Cruz RF, Waller MD, Perrin F, Periselneris J, Norton S, et al. (2020) Chest radiography is a poor predictor of respiratory symptoms and functional impairment in survivors of severe COVID-19 pneumonia. ERJ Open Res 7(1): 00655-2020.
-
Nanda S, Toussaint L, Vincent A, Fischer KM, Hurt R, et al. (2021) A Midwest COVID-19 Cohort for the Evaluation of Multimorbidity and Adverse Outcomes from COVID-19. J Prim Care Community Health 12: 1-6.
-
Jenicek M (2001) Clinical case reporting in Evidence- based Medicine. Clinical case reporting in Evidence- based Medicine 2nd (Edn.), Arnold, London, pp: 256.
-
Turabian JL (1995) Notebooks of Family and Community Medicine. An introduction to the principles of Family Medicine. Madrid.
-
Marino M, Lucas J, Latour E, Heintzman JD (2021) Missing data in primary care research: importance, implications and approaches. Fam Pract 38(2): 200-203.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria