A Case Control-Study of Cloperastine Treatment in Covid-19. Potential Drug, Clinical Observation and Common Sense
Background: Cloperastine, a widely used antihistamine drug in the treatment of cough, has been postulated as a potential treatment for coronavirus disease 2019 (COVID-19) as this drug modulates Sigma-1 receptor, a potential drug target. Objective: Efficacy of cloperastine (used as antitussive) evaluated according to the duration of COVID-19 symptoms in general medicine. Methodology: A case-control study (cases: duration of symptoms 13 days) was conducted in patients with COVID-19 confirmed with PCR, who consulted in general medicine office at a health center in Toledo, Spain, from March 1 to August 31, 2020, and the previous history was sought of exposure to the prescription factor of cloperastine. Results: 74 patients were included, 43 cases (COVID-19 with improvement or cure 13 days or death). No statistically significant difference was found in exposure to cloperastine between cases and controls: Among the cases there were 18 patients exposed to cloperastine (42%); among the controls there were 12 patients exposed to cloperastine (39%) (X2 = 0.0742; p = .785336. NS). Conclusion: In the context of general medicine in Toledo (Spain), during the exponential growth phase of COVID-19 outbreak (March-May 2020) and the subsequent outbreaks (July and August 2020), the previous exposure to cloperastine was not significantly associated with improvement or early cure in COVID-19 patients. Due to the design of the study, this finding should be considered as preliminary or exploratory and be confirmed or refuted by clinical trials. However, the result is in line with what is observed naturally in Spain, where it is frequently used cloperastine, but with high mortality data. It is suggested that the efficacy of cloperastine against COVID-19, if it exists, will be modest, and possibly of little clinical-epidemiological value.
Introduction
On March 11, 2020, the World Health Organization declared the coronavirus disease 2019 (COVID-19) outbreak a pandemic. To date, the 2019 coronavirus disease (COVID-19) pandemic has caused more than 34 million cases and more than 1 million deaths worldwide [1, 2, 3, 4, 5, 6]. In just over six months, numerous pharmacological and non-pharmacological interventions have been implemented to try to limit patient exposure, stop the spread and provide medical treatments to those infected [7, 8]. However, there is currently no vaccine or effective medical treatment for COVID-19, and treatment algorithms have included treatments for which data from randomized trials were not available. It can be said as of this writing that the only pharmacological interventions with proven benefit in this early stage of the pandemic include the use of immunomodulatory therapies in patients with severe respiratory problems (ventilated or oxygen dependent): remdesivir and dexamethasone [9, 10].
However, on the one hand, the growing burden of coronavirus disease (COVID-19) has led to the massive use of other drugs with uncertain or unproven effects such as hydroxychloroquine, azithromycin, ivermectin, tocilizumab, and Interferon-β [11, 12, 13]. In addition there are anecdotal suggestions about indomethacin, celecoxib, zinc, dipyridamole, vitamin D, fenofibrate, vitamin C, etc. And, on the other hand, the drugs for which the first useful results are obtained refer to hospitalized and seriously ill patients. Thus, with respect to remdesivir, it is suggested that this drug shortens the course of the disease for hospitalized patients and reduces the risk of death by up to 62% in critically ill patients; so, viral infection develops less quickly and patients in severe state recover an average of four days earlier than usual, conferring a modest clinical benefit for patients and the clinical significance of these findings is uncertain [14, 15]. And, with respect to dexamethasone, it reduced death rates by about a third among seriously ill hospitalized COVID-19 patients [13].
Thus, none of these interventions is applicable at the onset of the disease or at the community level at the general medicine (GM) level. Therefore, it would be a good question to ask about outpatient treatment of mild-moderate disease. This is where research and publications are lacking. All there is “anecdotal” evidence. It should be borne in mind that all severe and critical COVID-19 patients were previously mild or moderate COVID-19 patients or uninfected citizens. It must be taken into account that the strategies to develop a new therapy will require a lot of time and very extensive resources. Therefore, drug reuse has become an ideal strategy towards a smart, versatile and rapid way of possible COVID-19 treatments [16, 17]. Thus, drugs whose operation has already been tested in people -even against other viruses or in other indications- are the ones that are most likely to be used in the short term [14]. In this context, a study carried out by researchers from the US and Hong Kong has indicated the existence of a certain number of compounds that could be potential viral blockers of the severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2) causing of COVID-19. The study, carried out on a total of 12,000 compounds, has obtained 100 “good candidates” with the potential to block the viral replication of SARS-CoV-2 [18].
SARSCoV2 has been found to manipulate cells by blocking at least 332 of its own proteins; In this way the virus causes the host cells to produce new viruses. They are housed in a pair of proteins known as receptor Sigma-1 (Sig- 1R) and Sigma-2 (Sig-2R). These receptors are part of the cell’s communication network and help it resist stress in its environment. However, it is not really known why SARSCoV2 needs to manipulate Sigma receptors. One possibility is that the virus uses Sigma receptors to make a cell produce more of the oily molecules that form membranes for new viruses. Among the substances that act on Sigma receptors and block the virus, is cloperastine [17]. Thus, it has been postulated that drugs that modulate proteins within the cell through Sig-1R and Sig-2R, including the antihistamine used as antitussive, cloperastin, would be promising agents to effectively reduce viral infectivity in COVID-19 [18, 19].
Cloperastine is an antihistamine, but it has other effects, in addition to modulating Sig-1R: inhibiting SGLT1blocking glucose uptake in lung cells [20], and acting on other various cell receptors or channels [21, 22]. However, cloperastine has only been tested against the virus in laboratory experiments, and a 20% or 30% reduction in virus has been reported, which is a modest or very modest reduction [20].
Cloperastine was first studied at the University of Tokyo and was introduced in Japan in the 70s of the last century [23]. It is a derivative of diphenhydramine. Scientists found that this substance had a more effective effect than codeine, which has been used for years to treat coughs. Cloperastine is marketed worldwide and especially by countries in North America, Europe, Japan, Brazil, Russia, India, China, South Africa and Australia [24, 25]. Cloperastine is a widely used drug in the treatment of acute and chronic cough in pediatric and adults patients, having a dual mechanism of action at the central bulbar cough center and at peripheral receptors in the tracheobronchial tree. Chemically, it has antihistaminic properties related to an ethylamine moiety, which is common to anticholinergic agents [26].
The prescription of cough suppressants, including cloperastine, is frequent in some countries, mainly Japan
[20, 27] and in Spain, where it is available, can be obtained without a prescription (it is not funded by the Public Health System), and where it is prescribed and used frequently [28, 29]. And even clinical guidelines usually recommend it for the treatment of dry cough in adults, the elderly, and children over two years of age, pointing out cloperastine as the best option, preferably as an antitussive over codeine, its synthetic derivative dextromethorphan, and mucoilitics such as methyl arahydroxybenzoate sodium salt, ambroxol, etc [30, 31, 32].
It is evident that cough is a frequent reason for consultation in emergency services, GM and pediatrics that entails a significant consumption of cough suppressants [27, 33]. Cough constitutes an impressive expression of the normal defense mechanisms of the respiratory system. Cloperastine has been investigated in various types of cough and, unlike codeine, has been shown to possess dual activity. It also acts as a mild bronchorelaxant and has antihistaminic activity [23].
But, coughing is also one of the top three symptoms of COVID-19 [34]. While a wide range of symptoms can accompany to COVID-19, the majority of patients exhibit one of three symptoms: fever, cough, and shortness of breath (96% of patients have fever, cough, or shortness of breathe). And the most common symptom was cough (84%) followed by fever (80%) [35]. Thus, cloperastine, being an antitussive and an antihistamine, already has the correct indication in COVID-19, especially at the level of GM or out-of-hospital, where patients with less severe COVID-19 are treated.
On the other hand, randomized clinical trials continue to be the best available method for understanding the causal relationship between an intervention and subsequent outcome. But, in the absence of these data, patients, families, doctors and the health system are forced to rely on common sense and observation. Although, the urgent need for effective treatment has led to multiple proposed therapies with a plausible mechanism (common sense) and potential benefits, data based on the best possible evidence are accurate [36]. In this scenario, a small preliminary study of cases and controls (COVID-19 patients with improvement / cure or without improvement/cure) exposed or not previously to cloperastine is presented, carried out in a GM consultation in Toledo (Spain) with the aim of initially exploring the usefulness of this drug, which is available over the counter and widely used in Spain as an antitussive.
Material and Methods
A longitudinal, retrospective, analytical and observational case-control study was carried out, in which, based on the presence or absence of improvement / cure, a previous history of exposure to the prescribing factor of cloperastine was sought in patients with COVID-19 confirmed with polymerase chain reaction (PCR) oropharyngeal. As cloperastine is a frequently used antitussive in Spain and in the consultation object of the study, the study design was retrospective and therefore it was not a clinical trial: the GP prescribed cloperastin to patients with COVID-19 with cough as symptomatic treatment. At the initial moment of the data studied, the author was not aware that cloperastine could have any effect on COVID-19, and it was not prescribed in order to analyze its results; this decision was later, and thus, with retrospective data collection.
The study was conducted at a GM consultation in the Santa Maria de Benquerencia Health Center, Toledo, Spain, was conducted, which has a list of 2,000 patients> 14 years of age (in Spain, general practitioners -GPs- care for people> = 14 years of age, except for exceptions requested by the child’s family and accepted by the GP), from March 15, 2020 to August 31, 2020. Because of at the beginning of outbreak diagnostic tests were not available at the primary care level, since the instructions indicated that diagnostic test for SARS- CoV-2 be performed at people with a clinical picture of acute respiratory infection admitted to the hospital. Similarly, routine diagnostic tests are not performed on contacts [36, 37]. It was since May 19, 2020 PCR began to be carried out on suspected COVID-19 cases in GM. In this way, patients undergoing follow-up after diagnosis at the hospital were initially cared for, and later also patients diagnosed in GM.
Inclusion Criteria
All patients with COVID-19 confirmed with PCR from March 1 to August 31, 2020 who could be followed in their evolution in the consultation object of the study. Only cases of patients who belonged to the office list of patients and for whom data were available on their entire clinic course, from start to “cure” or death (hospital data including), were included; During this period, other cases of COVID-19, belonging to other surgeries, were attended occasionally due to the absence of their usual GP.
Definition of Result
Patient-reported outcomes self-assessments of patient health status are central to COVID-19 response, recovery, and resilience [38]. Based on this criterion, the result was the duration of the disease assessed by the number of days of duration from the onset to the disappearance of symptoms, reported and assessed by the patient. The result was quantitatively defined as follows: the arithmetic mean of the sick days of all the patients studied (except the deceased) was calculated, which showed a mean of 13 days. It was considered as “improvement or cure” when the number of days of illness were less than or equal to the arithmetic mean of days of illness of the total of patients (13 days; which supposes the center of gravity of a distribution) and it was considered “no improvement or no cure” when the number of sick days was greater than or equal to the arithmetic mean (>13) of sick days of all patients, or death had occurred.
Definition of Case and Control
Thus, “case” was defined as any patient who presented “improvement or cure” (duration of symptoms <= 13 days), and “control” was defined as any patient who presented “no improvement or no cure” (duration of symptoms> 13 days) of illness
Sample Size
Sample size was calculated for unpaired case-control studies for a Two-sided Confidence Level (1-alpha) of 95, a Power (% probability of detection) of 80, a Ratio of controls per case of 1, a Hypothetical ratio of controls with 30% exposure, Hypothetical proportion of cases with 65% exposure, Total Sample Size (Kelsey) should be 64; 32 cases and 32 controls [39].
Collected Variables
The following variables were collected: days duration of symptoms, age, sex, symptoms, severity, treatments different from cloperastine in the course of COVID-19 disease, and chronic diseases (defined as “any alteration or deviation from normal that has one or more of the following characteristics: is permanent, leaves residual impairment, is caused by a non- reversible pathological alteration, requires special training of the patient for rehabilitation, and / or can be expected to require a long period of control, observation or treatment” [40, 41, 42], classified according to the International Statistical Classification of Diseases and Health-Related Problems, CD- 10 Version: 2019 [43].
The severity classification was based on 4 levels according to severity of symptoms: mild, moderate, severe and critical. Mild patient that only showed as mild symptoms in without radiographic feature; Moderate patient showed as fever, respiratory symptoms & radiographic feature; Severe cases of meeting one of three criteria such as dyspnea, respiratory rate> 30 times / min; oxygen saturation <93% in ambient air; PaO2 / FiO2 <300 mmHg; For critical patient also meet one of three criteria such as respiratory failure; septic shock; multiple organ failure [44]. The classification of these cases to mild, moderate and severe depends on a subjective evaluation that in some cases was carried out remotely [45]. In the cases that required hospitalization, hospital reports were used to obtain the data. Following previous communications on the minor importance of the radiological examination as a diagnostic tool [46, 47], X-rays and other imaging tests were not performed systematically in all cases.
Guidelines for the management of suspected or confirmed cases in the community were followed. These guidelines recommend minimizing personal consultation and limited examination unless necessary (limited examination means that auscultation is not essential, and a rapid diagnosis of pneumonia could be made based on confusion, temperature, respiratory rate and heart rate, which are the clinical observations that are readily available to professionals in primary health care). So, the most of the consultations with patients were remote or telemedicine consultations [48, 49].
Statistical Analysis
The bivariate comparisons were performed using the Chi Square test (X2), X2 with Yates correction or Fisher Exact Test, for percentages, and the Student t test for the mean.
Results
74 patients were included, 43 cases (COVID-19 with improvement or cure <= 13 days) and 31 controls (COVID-19 with improvement or cure> 13 days or death). There were 4 patients who died. Both groups did not differ by sex: 23 (54%) were women in the group of cases, and 14 (45%) in the group of controls, and 20 (46%) men in cases and 17 (55%) in controls (X2 = 0.4996; p = .479665. NS). Likewise, both groups did not differ according to those under 65: 40 (93%) in cases and 23 (74%) in controls (X2 with Yates correction= 3.6686; p= .055448. NS); but the mean age was lower in the group of cases. There were no differences between cases and controls for COVID-19 symptoms, except that the cases had fewer mental symptoms. On the other hand, the cases did differ from the controls in that they presented less severity: in the cases, patients with mild-moderate severity were 41 (95%) vs. 20 (65%) in controls (X2 = 11.8253; p = .000584. Significant at p <.05) (Table 1). The cases and controls did not differ by prevalence of chronic diseases, except that the cases presented fewer diseases of the circulatory system (Table 2). Regarding the treatments received for COVID-19 (except cloperastine), there were no statistically significant differences between cases and controls, except that the cases received more analgesic drugs (Table 3).
| Variables n=74 | Cases (Time To Improvement Or Healing <= 13 Days) n=43 | Controls (Time To Improvement Or Cure> 13 Days Or Death) n=31 | Statistical Significance |
|---|---|---|---|
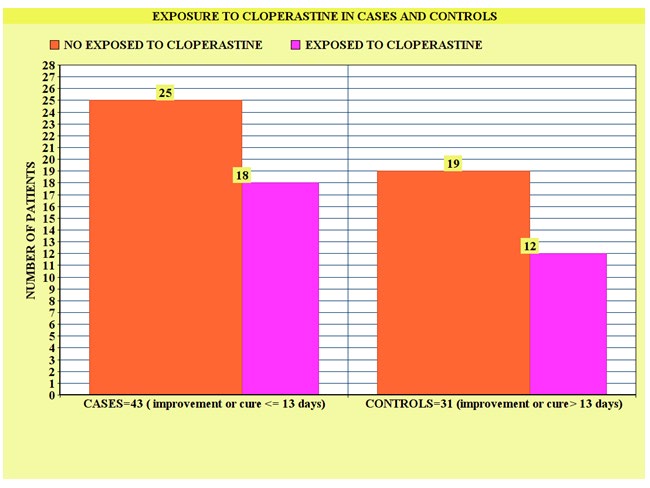
| Exposed to Cloperastine | 18 (42) | 12 (39) | X2 = 0.0742; p= .785336. NS |
| Symptom duration (arithmetic mean and standard deviation) | 5.7 +- 4.0 | 24.9 +- 10.1 | t = -11.10655; p < .00001. |
| Age (arithmetic mean and Standard deviation) | 35.0 +- 18.4 | 50.7 +- 15.8 | t = -3.81578; p= .000142. NS |
| <65 years | 40 (93) | 23 (74) | X2 with Yates correction= 3.6686; p= .055448. NS |
| Women | 23 (54) | 14 (45) | X2= 0.4996; p= .479665. NS |
| Respiratory symptoms * (cough, dyspnea, chest pain) | 24 (32) | 40 (33) | X2= 0.0026; p= .959088. NS |
| General symptoms * (fever, asthenia, general pain, arthralgia, myalgia, headache) | 34 (46) | 41 (34) | X2=2.9689; p = .084882. NS |
| ENT symptoms * (odynophagia, ageusia, anosmia, rhinorrhoea) | 8 (11) | 11 (9) | X2= 0.1694; p = .680627. NS |
| Digestive symptoms * (anorexia, nausea, vomiting, diarrhea, dysphagia) | 3 (4) | 10 (8) | X2 with Yates correction= 0.6952; p= .404413. NS |
| Dermatological symptoms * (chilblains / blisters, petechiae) | 0 | 2 (2) | Fisher exact test= 0.5276. NS |
| Neurological symptoms * | 5 (7) | 10 (8) | X2= 0.1351; p= .713162. NS |
| (headache, dizziness, tremor) | |||
| Mental symptoms * (anxiety, grief, insomnia) | 0 | 8 (7) | Fisher exact test= 0.0256. Significant at p < .05. |
| TOTAL symptoms (n=196) | 74 (100) | 122 (100) | |
| Mild-Moderate Severity | 41 (95) | 20 (65) | X2= 11.8253; p = .000584. Significant at p < .05. |
| Severe-Critical Severity | 2 (5) | 11 (35) | X2= 11.8253; p= .000584. Significant at p < .05. |
Table 1: ** Description of the Variables in Cases (Improvement or Cure Time <= 13 Days) and Controls (Improvement or Cure Time> 1
( ): Denotes percentages *Patients could have more than one symptom. The percentages of the symptoms are on the total of symptoms of cases and controls NS: Not significant at p < .05. Table 1: Description of the Variables in Cases (Improvement or Cure Time <= 13 Days) and Controls (Improvement or Cure Time> 13 Days or Death).
| Chronic Diseases according to who, Icd-10 Groups n=74 | Cases (Time to Improvement or Healing <= 13 Days) n=43 | Controls (Time to Improvement or Cure Time> 13 Days or Death) n=31 | Statistical Significance |
|---|---|---|---|
| -II Neoplasms | 1 (2) | 1 (2) | Fisher exact test = 1. NS |
| -IV Endocrine | 11 (23) | 12 (21) | X2= 0.0827; p= .773665. NS |
| -V Mental | 3 (6) | 6 (10) | X2= 0.5594; p= .454493. NS |
| -VI-VIII Nervous and Senses | 6 (13) | 1 (2) | X2 with Yates correction = 3.376; p= .066152. NS |
| -IX Circulatory system | 4 (9) | 13 (23) | X2 = 3.8503; p= .049738. Significant at p < .05 |
| -X Respiratory system | 3 (6) | 8 (14) | X2 with Yates correction = 0.8883; p= .345934. NS |
| -XI Digestive system | 4 (9) | 6 (10) | X2 with Yates correction = 0.0002. NS |
| -XII Diseases of the skin | 2 (4) | 1 (2) | Fisher exact test = 0.5881. NS |
| -XIII Musculo-skeletal | 6 (13) | 4 (7) | X2 with Yates correction = 0.4297. NS |
| -XIV Genitourinary | 7 (15) | 5 (9) | X2= 0.9458; p= .330802. NS |
| TOTAL=104 * | 47 (100) | 57 (100) |
Table 2: ** Distribution of Chronic Diseases in Cases (Time to Improvement or Cure <= 13 Days) and Controls (Time To Improvement
( ): Denotes percentages *Patients could have more than one chronic disease. The percentages of chronic diseases are over the total of chronic diseases of cases and controls Table 2: Distribution of Chronic Diseases in Cases (Time to Improvement or Cure <= 13 Days) and Controls (Time To Improvement or Cure> 13 Days Or Death).
| Cases (Time to Improvement or Healing <= 13 Days) n=43 | Controls (Time to Improvement or Cure Time> 13 Days or Death) n=31 | Statistical Significance | |
|---|---|---|---|
| ANALGESIC DRUGS (paracetamol [acetaminofen], metamizol)) | 17 (55) | 12 (16) | X2 = 16.6483; p= .000045. Significant at p < .05. |
| NSAIDs | 4 (13) | 3 (4) | Fisher exact test = 0.1904. NS |
| CODEINE | 1 (3) | 2 (3) | Fisher exact test = 1. NS |
| MUCOLYTICS (Carbocysteine, Acetylcysteine, Bromhexine, Ambroxol) | 2 (6) | 2 (3) | Fisher exact test = 0.5786. |
| BRONCHODILATORS (Salbutamol, Ipratropium) | 2 (7) | 8 (10) | X2 with Yates correction = 0.0962. p = .756476. NS |
| ANTIBIOTICS | 4 (13) | 20 (26) | X2 = 2.3722. p = .12351. NS |
| (Azithromycin, Ceftriazone, Linezolid) | 4 (13) | 20 (26) | X2 = 2.3722. p = .12351. NS |
| HYDROXYCHLOROCINE | 0 | 7 (9) | Fisher exact test = 0.1032. NS |
| ANTIRETROVIRALS (Lopinavir, ritonavir) | 0 | 8 (11) | Fisher exact test = 0.1014. NS |
| BIOLOGICAL DRUGS (tocilizumab) | 0 | 3 (4) | Fisher exact test = 0.5541. NS |
| CORTICOSTEROIDS | 0 | 3 (4) | Fisher exact test = 0.5541. NS |
| ANTIEMETICS | 0 | 2 (3) | Fisher exact test = 1. NS |
| PROTON-PUMP INHIBITOR | 0 | 2 (3) | Fisher exact test = 1. NS |
| LOW MOLECULAR WEIGHT HEPARIN | 1 (3) | 2 (3) | Fisher exact test = 1. NS |
| IMMUNOGLOBULINS | 0 | 1 (1) | Fisher exact test = 1. NS |
| TOTAL (n=106)* | 31 (100) | 75 (100) |
Table 3: Description of Treatments for Covid-10 in Cases (Time of Improvement or Cure <= 13 Days) and Controls (Time Of Improveme
As main result, no statistically significant difference was found in exposure to cloperastine between cases and controls: Among the cases (COVID-19 with improvement or cure <= 13 days) there were 18 patients exposed to cloperastine (42%); among the controls (COVID-19 with improvement or cure> 13 days or death) there were 12 patients exposed to cloperastine (39%) (X2 = 0.0742; p= .785336. NS) (Figure 1).
Discussion
Cloperastine is theoretically a promising drug for effectively reducing viral infectivity. An international effort that includes researchers from the University of California, San Francisco (UCSF), the Gladstone Institutes, the Icahn School of Medicine at Mount Sinai and the Institut Pasteur (Paris) revealed promising compounds for clinical trials against COVID-19: Some Medications can fight COVID-19 while others promote infectivity. By looking at a list of drugs that interact with the protein blueprint, the UCSF researchers led studies using chemical biology and computational approaches. Two categories of drugs emerged as promising agents to effectively reduce viral infectivity: protein translation inhibitors (including zotatifine and ternatine-4 / plitidepsin) and drugs that modulate proteins within the cell known as Sig-1R and Sigma2. Including progesterone, PB28, PD-144418, hydroxychloroquine; the antipsychotic drugs haloperidol and cloperazine; siramesin, an antidepressant and anxiolytic drug; and the antihistamines clemastine and cloperastine. In this context, cloperastine would have been shown to be effective in interrupting the replication of the coronavirus in monkey cells, with a 20% or 30% reduction in the virus reported in the laboratory, but so far the drug has not been tested in humans against this infection. In our study, the prescription of cloperastine was motivated by clinical reasons (cough, itchy throat, pharyngeal secretions, hoarseness, etc.), and not for the purpose of a clinical trial to evaluate its efficacy in COVID-19.
Mechanisms of Action of Cloperastine
Cloperastine is marketed as a cough suppressant mainly in Japan, Hong Kong, and in some European countries, such as Spain and Italy [23, 50, 51, 52, 53, 54]. The precise mechanism of action of cloperastin is not completely clear, but several different biological activities have been identified for the drug, including: Sig-1R ligand (probably an agonist) [55], GIRK channel blocker [56, 57, 58, 59], antihistamine action (for the H1 receptor) [23, 55] and anticholinergic [23, 60]. The last two properties are believed to contribute to side effects, such as sedation and drowsiness, while the first two may be involved or responsible for the antitussive efficacy of cloperastine [61].
The Sigma-1 Receptor (Sig-1R)
Sigma1, also known as Sig-1R, or σ1R is a unique cellular protein that was recently identified as a potential drug target to treat COVID-19. The Sig-1R is one of two sigma receptor subtypes; it is a chaperone protein at the endoplasmic reticulum (ER) that modulates calcium signaling through the IP3 receptor. In humans, the Sig-1R is encoded by the SIGMAR1 gene [62, 63, 64, 65, 66, 67]. Receptor binding is one of the main determinants of tissue tropism for coronaviruses and appears to be an important mediator of COVID-19 pathophysiology. The CoV spike protein of SARS-CoV-2 plays the most important roles in viral binding, fusion and entry, and serves as a target for the development of antibodies, entry inhibitors, and vaccines. The possible participation of a wide range of receptors in the entry of SARS-CoV-2 into cells has been hypothesized. A foregoing line of evidence supports the hermeneutical notion that the SARS-CoV-2 might enter the cell via angiotensin-converting enzyme-2 receptors. Presumably, Sig-1R might play a role in the infectivity of SARS- CoV-2. Previous research has suggested that pharmacological manipulation of Sig-1R activity might provide antiviral activity, particularly for RNA viruses including hepatitis C virus (HCV) and human immunodeficiency viruses (HIV). These findings indicate that Sig-1R may also be involved in the cellular transmission of SARS-CoV-2, which has a genomic structure similar to that of HCV and HIV [68].
Cloperastine Has another Effect: It is an Inhibitor of SGLT1
Cloperastine blocks glucose uptake in lung cells [20, 69, 70]. The study of primary human lung cells that were infected in the laboratory with SARS-CoV-2 has shown how the cells accumulate large amounts of lipid. After infection, lung proteins decrease the ability of lung cells to burn carbohydrates and fatty acids. Lung cells are not designed to retain fat, which could explain some of the severe damage to the lungs of COVID-19 patients. The virus depends on the absorption of glucose, the production of cholesterol and the oxidation of fatty acids.
Cloperastine Efficacy Assessed According to Duration of Symptoms
In our study, the duration of symptoms was chosen as the outcome measure. However, the duration of symptoms is not the main measure of interest in COVID-19 studies. Although an average length of hospital stay of 5-14 days has been reported, according to differences in admission and discharge criteria between countries, age, severity of the disease, and the different moments within the pandemic, it is known relatively little about the clinical course of COVID-19 and return to initial health for people with milder ambulatory illnesses [71].
Patient-reported outcomes self-assessments of patient health status are central to COVID-19 response, recovery, and resilience. Thus, in our study the reported duration of symptoms was used as an outcome. On the other hand, the arithmetic mean of the number of days with symptoms is a familiar and intuitively clear concept for the doctor, the patient and the health system. Therefore, this symptom duration criterion was chosen because it is more reasonable in primary care. Furthermore, the criterion was “conservative or modest”: the duration of symptoms until improvement or cure <= 13 days (<= the arithmetic mean of the duration of symptoms of all patients), it is a low or “modest” level of definition of improvement. It has been reported that, in general, many people have symptoms for two weeks and a few patients more and a few less. Patients with more serious illnesses are considered to need care and continue to have symptoms such as dyspnea for six weeks or longer. In addition, a significant number of previously healthy young patients, one in five, do not regain their normal health within 14 to 21 days after testing positive for the virus. In fact, 26% have been reported of people ages 18 to 34 who had a symptomatic case of COVID-19 had persistent symptoms, most commonly coughing, fatigue, and shortness of breath, more than two weeks after PCR. That number increased as people were aging: 32% of those aged 35 to 49 reported the same, along with 47% of those aged 50 and over [72, 73].
In our small retrospective study, where the cases and controls did not differ by sex or age (< and > 65 years), nor by the main symptoms of COVID-19, nor by the frequency of chronic diseases (except more diseases of the circulatory system (The clinical-epidemiological characteristics of some of these patients have already been published previously), no statistically significant differences in previous exposure to cloperastine were found (used at usual doses as antitussive, and prescribed as antitussive) between cases (COVID-19 with improvement or cure <= 13 days) and controls (COVID-19 with improvement or cure> 13 days or death).
Our group of cases differed from that of controls because they presented less severity of COVID-19. This fact probably reflects that patients with faster improvement or healing have less severity of the disease. This can be related to the fact that the group of cases presented fewer chronic diseases of the circulatory system. On the other hand, the group of cases showed a greater number of analgesic treatments; This would probably be an artefact, since patients in the control group presented greater severity of COVID-19, so they were treated more times in the hospital, and in the retrospective collection of the treatments based on hospital reports the analgesic treatment, is surely omited, with respect to the rest of the specialized treatment (antibiotics, antiretrovirals, hydroxychloroquine, biological drugs, etc.)
Regular use of Cloperastine; a Natural Experiment in Spain
In our retrospective study, cloperastine was not prescribed to test its efficacy in COVID-19 (the possibility of which was published much more recently than the date the majority of patients were treated), but was prescribed as an antitussive, which is of common use in Spain as symptomatic treatment, supported by clinical guidelines. This fact that cloperastine is frequently prescribed and used as an antitussive in Spain (furthermore, it is an Over The Counter drug, not subject to medical prescription and not funded by the health system), and that Spain was the country that had the second highest mortality rate in the time of most intense outbreak) [74], offers a natural experiment that seems to indicate that the efficacy of cloperastine on COVID-19 is at least very modest or possibly non-existent. The results of our study are compatible with this clinical observation in the natural experiment.
Cloperastine, Common Sense and Clinical Observation
Our study is including “real world” data with variables not initially collected for clinical research purposes; these variables were taken for a posterior investigation in a case-control design (patients with faster improvement and patient without rapid improvement or death, exposed or not to the prescription of cloperastine). Despite this argument, randomized clinical trials remain the best available method to understand the causal relationship between an intervention and subsequent evolution at the population level for most diseases. But, in the absence of data from randomized clinical trials, the evaluation relies on common sense and observation. In the context of the global COVID-19 pandemic, the urgent need for effective treatment has led to multiple proposed therapies with plausible mechanisms (common sense) and potential benefits. However, our study does not show clinical benefit in terms of reduction of days of COVID-19 symptoms, in exposed to cloperastine vs. not exposed.
Limitations and Strengths of the Study
This study should be considered a first exploration of the subject, and its results should be validated or refuted by studies with a more rigorous design (for example, clinical trials). There are a number of limitations and strengths that must be taken into account:
- The study is retrospective, which is often subject to biases (errors that affect the observations of an investigation); for example, in the collection of data.
- The final endpoint (improvement / cure if the duration of symptoms were <= than arithmetic mean -13 days), is certainly arbitrary. This can be identified as a weakness of the study; final endpoint could be no hospitalization or not death, or testing negative for active infection or positive for antibodies, the impact on viral load, etc. However, it is accepted that defining and measuring recovery from COVID-19 should be more sophisticated than checking for hospital discharge, or having a test negative for active infection or positive test for antibodies. In our endpoint criteria, once recovery is defined, we can differentiate COVID-19 that quickly goes away from the prolonged form [75].
- The design and location of the study do not ensure that the cases actually complied with the prescription of cloperastine, or that it was taken at the appropriate dose and time; It could be said that the results are analyzed under the principle of «intention to treat» [76].
- Cloperastine was prescribed as antitussive (symptomatic treatment, not etiological), and it was used at usual doses as antitussive. Therefore, the data and results of our study cannot be extrapolated to other possible interventions with other doses of the drug.
- The sample size can be considered small for the differences in exposure to cloperastine obtained in the case group (50%) and in the control group (39%), a sample of 400 cases and 400 controls would have been required to be able to find statistically significant differences. But, obviously, in that situation, one could not speak of clinical significance and practical utility in the treatment of COVID-19.
Conclusion
We must avoid the prescription of useless drugs, in general and for Covid19 itself. Many useless drugs can change immunity and promote iatrogenesis. In the context of GM in Toledo (Spain), during the exponential growth phase of COVID-19 outbreak (March-May 2020) and the subsequent outbreaks (July and August 2020), our study shows no clinical benefit, in terms of reduction of days duration of COVID-19 symptoms, in exposed to cloperastine vs. not exposed. This negative result is compatible with the clinical observation of incidence and mortality rates in Spain with a high prescription of cloperastine as antitussive. Due to the design of the study, this finding should be considered as preliminary or exploratory, and it represents only the result of clinical observation and common sense, and should be confirmed or refuted by clinical trials.
References
-
WHO (2020) WHO Timeline-COVID-19.
-
Información Científica-Técnica (2020) Coronavirus disease, COVID-19 Update, August 28, 2020. Coordination Center for Health Alerts and Emergencies. Ministry of Health (Spain).
-
Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins. The Center for Systems Science and Engineering (CSSE) at JHU.
-
Li Q, Guan X, Wu P, Wang X, Zhou L, et al. (2020) Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med 382: 1199-1207.
-
Zhu N, Zhang D, Wang W, Li X, Yang B, et al. (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382: 727-733.
-
García-Basteiro AL, Chaccour C, Guinovart C, Llupià A, Brew J, et al. (2020) Monitoring the COVID-19 epidemic in the context of widespread local transmission. Lancet Respir Med 8(5): 440-442.
-
Tay MZ, Poh CM, Rénia L, MacAry PA, Ng LFP, et al. (2020) The trinity of COVID-19: immunity, inflammation and intervention. Nat Rev Immunol 20: 363-374.
-
Ramirez-Valles J, Breton E, Chae DH, Haardörfer R, Kuhns LM (2020) The COVID-19 Pandemic: Everything Old Is New Again in Public Health Education. Health Educ Behav 47(4): 501-513.
-
Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, et al. (2020) Remdesivir for the Treatment of Covid- 19-Preliminary Report. N Engl J Med.
-
Recovery Collaborative Group (2020) Effect of Dexamethasone in Hospitalized Patients with COVID-19- Preliminary Report. N Engl J Med.
-
Nagaraja BS, Ramesh KN, Dhar D, Samim MM, Treshita D, et al. (2020) HyPE study: hydroxychloroquine prophylaxis-related adverse events’ analysis among healthcare workers during COVID-19 pandemic: a rising public health concern. Journal of Public Health 42(3): 493-503.
-
Turabian JL (2020) Acute Respiratory Infections in Children during Coronavirus Disease 2019: Without Reverse Transcriptase-Polymerase Chain Reaction Test and With Risk of Over-Prescription of Antibiotics, the Perfect Storm. Pediatric Infect Dis 5(2): 1.
-
Scudder L (2020) Drug Treatment for COVID-19: A Quick Summary for PCPs. Medscape.
-
NIH (2020) NIH clinical trial shows Remdesivir accelerates recovery from advanced COVID-19. NIH News Releases.
-
Spinner CD, Gottlieb RL, Criner GJ, López JRA, Cattelan AM, et al. (2020) Effect of Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients With Moderate COVID-19: A Randomized Clinical Trial. JAMA 324(11): 1048-1057.
-
Nazeam J, Mohammed EZ, Raafat M, Houssein M, Elkafoury A, et al. (2020) Based on Principles and Insights of COVID-19 Epidemiology, Genome Sequencing, and Pathogenesis: Retrospective Analysis of Sinigrin and ProlixinRX (Fluphenazine) Provides Off-Label Drug Candidates. SLAS DISCOVERY.
-
Zimmer C (2020) Old Drugs May Find a New Purpose: Fighting the Coronavirus. The New York Times.
-
Gordon DE, Jang GM, Bouhaddou M, Xu J, Obernier K, et al. (2020) A SARS-CoV-2 protein interaction map reveals targets for drug repurposing. Nature 583: 459-468.
-
Institut Pasteur (2020) Revealing how SARS-CoV-2 hijacks human cells; points to drugs with potential to fight COVID-19 and a drug that aids its infectious growth.
-
Whyte J, Nahmias Y (2020) Can Cholesterol Drugs and Antihistamines Fight COVID-19?. Medscape.
-
Takahara A, Fujiwara K, Ohtsuki A, Oka T, Namekata I, et al. (2012) Effects of the Antitussive Drug Cloperastine on Ventricular Repolarization in Halothane-Anesthetized Guinea Pigs. J Pharmacol Sci 120(3): 165-175.
-
Takahama K (2012) Multiple Pharmacological Actions of Centrally Acting Antitussives-Do They Target G Protein- Coupled Inwardly Rectifying K+ (GIRK) Channels?. J Pharmacol Sci 120: 146-151.
-
Catania MA, Cuzzocrea S (2011) Pharmacological and clinical overview of cloperastine in treatment of cough. Ther Clin Risk Manag 7: 83-92.
-
Market Research, Pharmaceutical, Therapy Market Trends (2017) Cloperastine Sales, Price Analysis, & Sales Forecast-2017, Report Linker.
-
Clifford C (2020) Cloperastine Hydrochloride (CAS 14984-68-0) Market 2020 Industry Size, Share, Growth Drivers, Top Leaders, Development Strategy, Future Trends, Historical Analysis, Competitive Landscape, and Regional Forecast 2026 | Impact of COVID-19 on the industry, La Vanguardia Noticias.
-
Serrano M, Sanz‐Cuesta M, Villaronga M, Frontado Hayek L, Perez‐Dueñas B (2012) Cloperastine‐based cough syrup and acute dystonic reactions. Dev Med Child Neurol 54(3): 287.
-
Jofré DP, García KC (2017) Cough in otolaryngology: An up to date of the diagnostic approach. Rev Otorrinolaringol Cir Cabeza Cuello 77(4).
-
Blanco Guzmán E, Ruano López A, Ugarte Libano R (2013) Antitussive prescription in Primary Care pediatricians of the Basque Country. Rev Pediatr Aten Primaria 15(59).
-
Cano Garcinuño A, Casares Alonso I, Rodríguez Barbero J, Pérez García I, Blanco Quirós A (2012) Prescription of systemic cold and cough drugs to children 0-13 years old. An unresolved problem. An Pediatr (Barc) 78(1): 43-50.
-
Redacción (2019) The most widely used cough syrups lack evidence on their effectiveness. El Independiente.
-
Centros Gerontológicos Gipuzkoa (2012) Pharmacotherapeutic guide for geriatric patients. Eusko Jaurlaritza-Gobierno Vasco, Osasun eta Kontsumo Saila- Departamento de Sanidad y Consumo.
-
Spessot DE Antitusivos y Mucolíticos Farmacología Medicina U.N.N.E. Argentina.
-
Marchello CS, Ebell MH, McKay B, Shen Y, Harvill ET, et al. (2019) Clinical management decisions for adults with prolonged acute cough: Frequency and associated factors. Am J Emerg Med 37(9): 1681-1685.
-
Ellis R (2020) CDC Says Three COVID-19 Symptoms Are Most Common. Medscape.
-
Turabian JL (2020) Coronavirus Disease 2019 (COVID-19) in General Medicine: A Clinical-Epidemiological Case Series Reporting of 16 Patients in Toledo (Spain), March- May 2020 also in Covid-19, “If you Hear Hoofbeats, Think Horses not Zebras”. Epidemol Int J 4(S1): 000S1-006.
-
Bahit C (2020) Randomized clinical trials versus common sense and clinical observation. Medscape.
-
Turabian JL (2020) Micro-Impact of the Pandemic by Covid-19 in the General Medicine: Clinical and Epidemiological Reflections from the Situation in Spain March 2020. Epidemol Int J 4(2): 141.
-
Aiyegbusi OL, Calvert MJ (2020) Patient-reported outcomes: central to the management of COVID-19. Lancet 396(10250): 531.
-
Open Source Epidemiologic Statistics for Public Health.
-
Strauss AL (1984) Chronic illness and the quality of life. St Louis: The CV Mosby Company.
-
Gill M (2017) Augmented care: An alternative model of care for people with chronic disease. Int J Care Coord 20(1-2): 5-7.
-
Calderón-Larrañaga A, Vetrano DL, Onder G, Gimeno- Feliu LA, Coscollar-Santaliestra C, et al. (2016) Assessing and Measuring Chronic Multimorbidity in the Older Population: A Proposal for Its Operationalization. J Gerontol A Biol Sci Med 72(10): 1417-1423.
-
WHO (2019) International Statistical Classification of Diseases and Health-Related Problems. ICD-10 Version: 2019.
-
WHO (2020) Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19).
-
Hamed E, Abd Elhamid M, Alemrayat B (2020) Suspected cases of COVID-19: study protocol for reporting characteristics and the outcomes. Fam Med Community Health 8(2): e000400.
-
Qiu H, Wu J, Hong L, Luo Y, Song Q, et al. (2020) Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: an observational cohort study. Lancet Inf Dis 20(6): 689- 696.
-
Chen D, Tang F, Lu S, Song Q (2020) Toward a clinically based classification of disease severity for paediatric COVID-19-Authors’ reply. Lancet Inf Dis.
-
National Institute for Health and Care Excellence (NICE) (2020) COVID-19 rapid guideline: managing suspected or confirmed pneumonia in adults in the community (NG165).
-
National Institute for Health and Care Excellence (NICE) (2020) COVID-19 rapid guideline: managing symptoms (including at the end of life) in the community. NICE guideline [NG163].
-
National Center for Biotechnology Information (2020) PubChem Compound Summary for CID 2805, Cloperastine.
-
NCATS. Inxight: Drugs. CLOPERASTINE.
-
Elks J (2014) The Dictionary of Drugs: Chemical Data: Chemical Data, Structures and Bibliographies. Berlin, Springer, pp: 301.
-
Swiss Pharmaceutial Society, ed. (2000) Index Nominum 2000: International Drug Directory. 17th (Edn), Oxford, Medpharm Scientific Publishers.
-
William Andrew Publishing (2013) Pharmaceutical Manufacturing Encyclopedia. Elsevier, pp: 1103.
-
Gregori-Puigjané E, Setola V, Hert J, Crews BA, Irwin JJ, et al. (2012) Identifying mechanism-of-action targets for drugs and probes. Proc Natl Acad Sci U S A 109(28): 11178-11183.
-
Chung KF, Widdicombe J (2008) Pharmacology and Therapeutics of Cough. Berlin: Springer Science & Business Media, pp: 230.
-
Soeda F, Fujieda Y, Kinoshita M, Shirasaki T, Takahama K (2016) Centrally acting non-narcotic antitussives prevent hyperactivity in mice: Involvement of GIRK channels. Pharmacol Biochem Behav 144: 26-32.
-
Yamamoto G, Soeda F, Shirasaki T, Takahama K (2011) Is the GIRK channel a possible target in the development of a novel therapeutic drug of urinary disturbance?. Yakugaku Zasshi 131(4): 523-532.
-
Kawaura K, Honda S, Soeda F, Shirasaki T, Takahama K (2010). Novel antidepressant-like action of drugs possessing GIRK channel blocking action in rats. Yakugaku Zasshi 130(5): 699-705.
-
Korolkovas A (1988) Essentials of Medicinal Chemistry. Nueva Jersey, Wiley.
-
Cloperastine (2020) Wikipedia.
-
Sigma-1 receptor (2020) Wikipedia.
-
Su TP, Su TC, Nakamura Y, Tsai SY (2016) The Sigma-1 Receptor as a Pluripotent Modulator in Living Systems. Trends Pharmacol Sci 37(4): 262-278.
-
Maurice T, Su TP (2009) The pharmacology of sigma-1 receptors. Pharmacol Ther 124(2): 195-206.
-
López OV, Gorantla S, Segarra AC, Norat MCA, Álvarez M, et al. (2019) Sigma-1 Receptor Antagonist (BD1047) Decreases Cathepsin B Secretion in HIV-Infected Macrophages Exposed to Cocaine. J Neuroimmune Pharmacol 14(2): 226-240.
-
Friesland M, Mingorance L, Chung J, Chisari FV, Gastaminza P (2013) Sigma-1 receptor regulates early steps of viral RNA replication at the onset of hepatitis C virus infection. J Virol 87(11): 6377-6390.
-
Zhu LX, Sharma S, Gardner B, Escuadro B, Atianzar K, et al. (2003) IL-10 Mediates Sigma1 Receptor-Dependent Suppression of Antitumor Immunity. J Immunol 70(7): 3585-3591.
-
Yesilkaya UH, Balcioglu YH, Sahin S (2020) Reissuing the sigma receptors for SARS-CoV-2. J Clin Neurosci 80: 72- 73.
-
Oranje P, Gouka R, Burggraaff L, Vermeer M, Chalet C, et al. (2019) Novel natural and synthetic inhibitors of solute carriers SGLT1 and SGLT2. Pharmacol Res Perspect 7(4): e00504.
-
Dominguez Rieg JA, Rieg T (2019) What does sodium- glucose co-transporter 1 inhibition add: Prospects for dual inhibition. Diabetes Obes Metab 21(Suppl 2): 43-52.
-
Rees EM, Nightingale ES, Jafari Y, Waterlow NR, Clifford S, et al. (2020) COVID-19 length of hospital stay: a systematic review and data synthesis. BMC Med 18: 270.
-
Tenforde MW, Kim SS, Lindsell CJ, Rose EB, Shapiro NI, et al. (2020) Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network- United States. MMWR Morb Mortal Wkly Rep 69(30): 993-998.
-
COVID: UK Data (2020) How long does COVID-19 last? COVID Symptom Study.
-
RTVE (2020) Coronavirus. Peru, Belgium, the United Kingdom and Spain, the countries with the most deaths with coronavirus by number of inhabitants. RTVE es 27.08.
-
Alwan NA (2020) A negative COVID-19 test does not mean recovery. Pandemic policy must include defining and measuring what we mean by mild infection. Nature 584(170).
-
Capurro D, Gabrielli L, Letelier LM (2004) Intention to treat and follow up are important in assessing validity of a randomized clinical trial. Rev Méd Chile 132: 1557- 1560.
- Epidemiological Surveillance and Rumors on Social Media
- Awareness and Treatment of Uncontrolled Hypertension in US Overweight/Obese Youths Aged 16–24 Years, NHANES 2021–2023
- Strengthening EPI Through Parental Engagement: Lessons from Dhaka Slums for IA-2030
- Mothers Knowledge of the Prevalence, Causes, Effects, Prevention and Control of Diarrhoea among Children in Ife East Local Government Area, Ile Ife, Osun State, Nigeria
- Covid-19 Reinfections Case Series from October 2023 to October 2024 in A General Medicine Office in Toledo (Spain)
- Water Contact! One Risk Too Many: Risk Factors Associated with Schistosoma haematobium infection in Osun State, Nigeria