Comparison of Serum Immunoglobulin Free Light Chains Assay and Serum Immunofixation Electrophoresis in Patient Transplanted for Multiple Myeloma
Introduction: Serum immunofixation electrophoresis (sIFE) and serum free light chains (sFLC) immunoassays are fundamental for serum monoclonal protein diagnosis and monitoring. In this study, we compared the ability of these assays to detect monoclonal proteins in stem cell transplanted patients. Methods: Three hundred sixty sera belonging to 145 patients affected by MM after autologous stem cell transplantation [113 intact immunoglobulin multiple myeloma (IIMM) and 32 free light chains multiple myeloma (LCMM)] were analyzed by both sIFE and sFLC assay, respectively performed with the Binding Site Minifix Kit and the Binding Site Freelite kit on Cobas-Integra 400 Plus (Roche). Results: Two hundred one samples (55.8%) had an abnormal κ/λ ratio and 32.7% had a monoclonal restricted band in sIFE. For 61.38% samples, there was a concordance between sIFE and sFLC and there wasn’t for 139 samples (p<0.0001). Kappa Cohen’s coefficient was weak (κ= 0.25). When compared to sFLC immunoassay for IIMM, sIFE demonstrated a weak sensitivity of 80.7%, which increases to 94.74% when we compared only LCMM results. Accuracy of sIFE respect to sFLC was the better for IIMM (70.7%), than for all type MM (61.4%), and there was a significant difference between the accuracy of either of these techniques, when performed singly for all MM type, IIMM and LCMM. Conclusion: sFLC assay role in IIMM monitoring is to be confirmed by further studies. sFLC assay is a sensitive tool for the monitoring of patients after transplantation, and that it may be associated to sIFE assay to better individualizing minimal residual disease.
Introduction
Serum immunoglobulin (Ig) free light chain (sFLC) assay is an excellent test for the diagnosis and monitoring of nonsecretory multiple myeloma (MM), oligosecretory MM, as well as light chain MM (LCMM). The ratio of sFLC chains κ/λ being indicative of monoclonality. Whereas, sFLC testing is recommended for intact immunoglobulin MM (IIMM) monitoring and sFLC ratio calculation is of interest in the follow-up of the treated patients, since for about 10% of them, elevation of the sFLC precedes other residual disease markers [1]. Nevertheless, serum immunofixation electrophoresis (sIFE), remains a gold standard in IIMM monitoring [2].
Material and Methods
Material
Our work involved 360 sera samples collected from 145 autologous hematopoietic stem cell transplanted (AHSCT) patients (respectively, 80 sera from 32 patients with LCMM, and 280 sera from 113 patients with IIMM). This work was done as part of the routine testing of the laboratory, respecting the ethical rules.
Methods
All 360 samples were analyzed by both (sIFE) and sFLC assay. sIFE was performed with the Binding Site Minifix Kit. The sFLC assay was performed by Binding Site Freelite kit on Cobas-Integra 400 Plus (Roche).
Statistical Tests
Statistical analysis was done using (Anova Statistical Analysis). To obtain the association of categorical variables, Chi square test; Yates adjusted chi 2 and the Fisher exact test were applied. To find out the efficacy of two methods, McNemar test was used. Cohen’s kappa coefficient was used to assess the concordance between the results of the two techniques. A p value < 0.05 was considered as statistically significant.
Results
Patient Distribution
The average age of patients is 55 years (35 to 73 years). The sex ratio is 82 men / 63 women. The frequency of MM IgG prevails over all IIMM, whereas LCMM represent 22% of all MM.
Comparative Results of IFE and S-FLC Assay
Among the 360 samples analyzed, 201 samples (55.8%) had an abnormal κ/λ ratio and 118 samples (32.7%) had an abnormal sIFE (presence of a monoclonal band). Associations of categorical variables were studied for all MM type, IIMM alone and sFLC MM alone. Among these 360 samples, 221 had agreement between sIFE and κ/λ ratio [presence of a monoclonal band and an abnormal κ/λ ratio or normal sIFE and normal κ/λ ratio] and 139 were discordant [presence of a monoclonal band and normal κ/λ ratio; or normal sIFE and abnormal κ/λ ratio], with a statistically significant difference (p <0.0001). The concordance Cohen’s coefficient kappa found a fair agreement between these two assays (κ=0.25) [Standard error: 0.04; 95% CI: 0.17-0.33].
Accuracy of sFLC and sIFE in the diagnosis of MM relapse were studied for all MM type (Table 1), IIMM alone (Table 2) and LCMM alone (Table 3). Accuracy of sIFE was 61.4 % with respect to sFLC and we note a statistically significant difference between the accuracy of either of these techniques when performed singly in the detection of all MM type relapse (p<0.0001). The sIFE assay shows a low sensitivity (82.4%) and a very low specificity (44. 8%) with respect to sFLC assay (Table 1).
| normal κ/λ | abnormal κ/λ | p value | Sensitivity (%) | Specificity (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|
| normal sIFE | 131 | 111 | <0.0001 | 82.4 | 44.8 | 61.4 |
| abnormal sIFE | 28 | 90 |
Table 1: Accuracy of sFLC and sIFE in the diagnosis of monoclonal gammopathy (all type of MM).
| normal κ/λ | abnormal κ/λ | p value | Sensitivity (%) | Specificity (%) | Accuracy (%) | |
|---|---|---|---|---|---|---|
| normal sIFE | 113 | 55 | 0,0026 | 80.7 | 60.7 | 70.7 |
| abnormal sIFE | 27 | 85 | 0,0026 | 80.7 | 60.7 | 70.7 |
| for header rows | normal κ/λ | abnormal κ/λ | p value | Sensitivity (%) | Specificity (%) | Accuracy (%) |
| normal sIFE | 18 | 56 | <0.0001 | 94.7 | 8.2 | 28.7 |
| abnormal sIFE | 1 | 5 | <0.0001 | 94.7 | 8.2 | 28.7 |
Table 2: Accuracy of sFLC and sIFE in the diagnosis of monoclonal gammopathy (IIMM).
For the 2 groups of patients respectively with IIMM and with LCMM, the association between these two assays was statistically significant only for IIMM group, respectively p<0.0001 and p= 0.56. Whereas the concordance Cohen’s coefficient kappa found a fair agreement between these two assays (κ=0.37) [Standard error: 0.04; 95% CI: 0.28-0.46] for IIMM group and poor agreement (κ=0.01) [Standard error: 0.04; 95% CI: - 0.07-0.09] for LCMM group. The accuracy of sIFE came to be 70.7 % with respect to sFLC in the detection of IIMM relapse and fall considerably to 28.7% in the detection of LCMM relapse, with a statistically significant difference between the accuracy of either of these techniques when performed singly. Whereas, there was a statistically significant difference between the accuracy of either of these assays for the first and the second group, respectively p=0.0026 and p<0.0001 (Tables 2 & 3). The sIFE assay shows both low sensitivity (80.7%) and specificity (60.7 %) with respect to sFLC assay for the first group (Table 2). But for the second group the sIFE shows a high sensitivity (94.7%) and a very bad specificity (8.2 %) (Table 3). Note that for the association between sIFE and extreme κ/λ ratio, there was a statistically significant difference (Table 4). No statistically significant difference was found in the association between the sIFE results and the fact that MM had a κ or λ light chain (p=0.67).
| normal sIFE | abnormal sIFE | ||
|---|---|---|---|
| 100< κ/λ or <0,01 | 11 | 14 | 25 |
| 0,01< κ/λ or <100 | 231 | 104 | 335 |
| 242 | 118 | 360 |
Table 3: Association between sIFE results and extreme κ/λ ratio.
p=0.01. Table 4: Association between sIFE results and extreme κ/λ ratio.
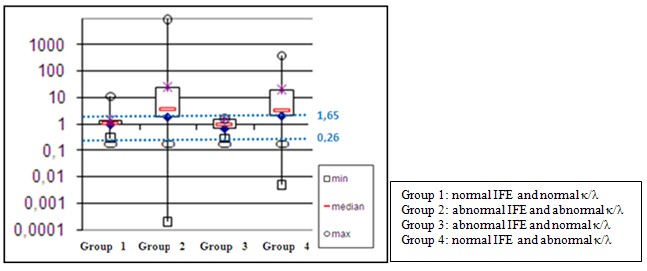
The group of patients who had both an abnormal κ/λ ratio and an abnormal sIFE had the largest distribution of these ratios beyond the normal range, whereas the group who had abnormal sIFE and normal κ/λ ratio had the narrowest one (Figure 1).
| Group 1 | Group 2 | Group 3 | Group 4 | |
|---|---|---|---|---|
| min | 0,29 | 0,0002 | 0,27 | 0,005 |
| médiane | 1,115 | 3,53 | 0,94 | 3,435 |
| max | 11,3 | 9372 | 1,65 | 386,46 |
Normal Values: 0,26 < κ/λ < 1,65. Figure 1: Box plots κ/λ ratios in patients’ different groups.
κ/λ ratio and Blood Creatinine
We have had blood creatinine at the same day of sFLC measurement for only 169 samples and median creatinine values were normal (<115 mmol/l) in patients with a normal κ/λ ratio as well as in those with an abnormal κ/λ ratio. No statistically significant difference was noted between those two groups (p=0.4). Seven patients had blood creatinine above normal range in the first group, extreme (121 mmol/l - 651 mmol/l) against 10 for the second group, extreme (143 mmol /l - 860 mmol/l).
Discussion
sFLC assay is currently the best way to diagnose and monitor LCMM. In this context, serum sFLC κ/λ ratio represents an essential element for such purpose, as well the difference between involved and uninvolved sFLC levels [1]. Other plasma cell dyscrasias such as light chain amyloidosis [3], oligosecretory myeloma [4] and light chain monoclonal gammopathy of undetermined significance (MGUS) [5] can also benefit from this test. For the other types of monoclonal gammopathy especially IIMM, which represents the most frequent one, the evaluation of the interest of this assay is still in progress. Nevertheless, various authors [6, 7, 8] evoke a certain interest for this assay not for the diagnosis of IIMM, but rather in monitoring the evolution of this pathology after transplant and/or chemotherapy [2]. In fact, the κ/λ ratio represents a more sensitive marker of residual disease than protein electrophoresis and serum sIFE [6, 9, 10]. According to Mead, et al. [9] the sFLC assay can be used as a rapid indicator of treatment response in the majority of patients with MM, sFLC having 2 to 6 hours half-life compared to intact immunoglobulin (1-3 weeks). So, this dosage more rapidly reflects the regression of the tumor than the whole intact immunoglobulin [11]. The use of sFLC to monitor relapse in patients with IIMM is rapidly developing as part of light chain escape phenomenon, which is an observation of isolated increasing sFLC concentrations as manifestation of relapse in patients with previous IIMM, has now been described in several case reports [12].
Among the updated diagnostic criteria of the International Myeloma Working Group (IMWG) [13], authors introduced serum sFLC ratio [if greater than or equal to 100 provided and if involved sFLC level is >100 mg/L], as specific biomarkers that can be used to diagnose the disease in patients who did not have CRAB features.
Nevertheless recently, some other authors [14, 15, 16, 17] have raised doubts about the real usefulness of sFLC, especially since the number of false positives and false negatives compared to serum protein electrophoresis (SPE) and sIFE are quite substantial. In the other hand, many factors can enhance those discrepancies such as renal failure [18], propensity of sFLC (especially those λ) to aggregate or polymerase, which may contributes to underestimation of λ FLC [15], hyper or hypogammaglobulinemia [19]. But the point still remaining is that sFLC measurement has the same utility and impact on MM diagnosis and monitoring. While some authors [16, 17] reject the utility of sFLC in the monitoring of MM, because there is neither any benefit from sFLC ratio normalization in clinical remission in myeloma patients in terms of progression-free survival or overall survival [16], nor any significance of the presence of sFLC, especially in autologous stem cell transplantation (ASCT) where the apparition of oligoclonal pattern (which aren’t synonymous to malignant monoclonal proteins), further degrades the performance of sFLC assay [17]. Recently some authors Michallet M & Greil C [20, 21] reported that the use of serum Heavy/light chain is valuable as diagnosis and monitoring tool in MM patients, and that it correlates with clinical outcome in those patients.
We analyzed 360 serum samples from 145 patients, 113 with IIMM and 32 with LCMM. IgG IIMM dominates with 56.5% of all MM, whereas LCMM account for only 22% of the total. Of the 360 samples analyzed, 201 samples (55.8%) had an abnormal κ/λ ratio and 118 samples (32.7%) had an abnormal sIFE appearance (presence of a monoclonal band). Of these 360 samples, 221 had agreement between sIFE and κ/λ ratio and 139 were discordant, with a statistically significant difference in favor of the κ/λ ratio (p <0.0001), which in agreement with what was reported by Milani, et al. [22] but discordant with what reported by other authors [14, 16, 23].
The Cohens’ concordance coefficient κ = 0.25, which denotes a weak correlation between the two assays. Concerning the concordance between sIFE and sFLC assay for IIMM, the frequency of 50% of abnormal κ/λ ratio is equal to that found by Wood, et al. [24]. While this difference remains statistically significant for IIMM (p <0.0001), it is no longer so if only the cases of myeloma with light chains are calculated. This fact can be associated with the detection of sFLC by sIFE in the case of LCMM, whereas in IIMM, these sFLC are not always found. On the other hand, the low sampling of LCMM in our work also has an impact on this result. Since the analyzed samples belong to patients at different stages of remission, the diagnostic value of the κ/λ ratio is not fully accepted, although this report is of interest in the monitoring of patients who are not in intact clinical remission [25].
The sensitivity, specificity of sIFE with respect to sFLC came to be as 82.4%, 80.7%, 94.7% and 44.8%, 60.7%, 8.2% (Tables 1-3) respectively for all type MM, IIMM and LCMM. These findings suggest that both of these techniques possess their own advantages and limitations and one cannot be considered superior over the other, as suggested by Kuriakose, et al. [26]. Particularly, this sensitivity of 94.7% for LCMM (Table 3) may indicates a better demonstration of the monoclonal immunoglobulin by the weighting of sFLC assay than by sIFE assay, as reported by some authors [6, 7, 27]. Whereas accuracy of sIFE respect to sFLC was the better for IIMM (70.7%) (Table 2), than for all type MM was 61.4% (Table 1), which is less than the value found by Kuriakose, et al. [26], there was a significant difference between the accuracy of either of these techniques, when performed singly for all MM type, IIMM and LCMM (Tables 1-3). The mean value of κ/λ in the group which was positive for monoclonal gammopathy was higher than in the group which was negative for monoclonal gammopathy, with a significant difference (Table 4), as reported partially by Kuriakose, et al. [26]. No significant difference was found concerning the association between sIFE results and light chain type, which indicates probably that there was no relative under- detection of lambda dominant κ/ λ ratio in our patients as suggested by some authors [14, 15]. As the median values of blood creatinine were normal in both normal κ/λ patients and those with abnormal κ/λ ratios, this fact indicates probably an absence of kidney damage that would cause an under-estimation of this ratio [28]. This fact is partially demonstrated in Table 8 which shows the absence of blood creatinine interference with free light chain values.
Conclusion
Among the assays used for the diagnosis and monitoring of monoclonal immunoglobulin, we have chosen two, sIFE assay and the sFLC assay, to assess their concordance and possible interest in this context. The sFLC assay is of interest for the diagnosis and follow-up of patients with LCMM, oligosecretory MM and amyloidis. The role of this assay in the monitoring of IIMM remains to be confirmed by larger sample studies. Discrepancies observed in the results between authors, may be due to the use of these assays, especially sFLC assay either in MM diagnosis and monitoring. The escape phenomenon and the under and/ or over estimation of a particular FLC, can also have repercussion on the reported results. Nevertheless, preliminary studies tend to show that sFLC assay is probably a sensitive tool for the monitoring of patients after transplantation, and that it may be associated to sIFE assay to better individualizing MM relapse, when negative minimal residual disease testing by flow cytometry or New Generation Sequencing are not available.
References
-
Willrich MAV, Katzmann JA (2016) Laboratory testing requirements for diagnosis and follow-up of multiple myeloma and related plasma cell dyscrasias. Clin Chem Lab Med 54(6): 907-919.
-
Dimopoulos M, Kyle R, Fermand JP, Rajkumar SV, San Miguel J, et al. (2011) Consensus recommendations for standard investigative workup: report of the International Myeloma Workshop Consensus Panel 3. Blood 117(18): 4701-4705.
-
Lachmann HJ, Gallimore R, Gillmore JD, Carr-Smith HD, Bradwell AR, et al. (2003) Outcome in systemic AL amyloidosis in relation to changes in concentration of circulating free immunoglobulin light chains following chemotherapy. Br J Haematol 122(1): 78-84.
-
Drayson M, Tang LX, Drew R, Mead GP, Carr-Smith H, et al. (2001) Serum free light-chain measurements for identifying and monitoring patients with nonsecretory multiple myeloma. Blood 97(9): 2900-2902.
-
Dispenzieri A, Katzmann JA, Kyle RA, Larson DR, Melton LJ, et al. (2010) Prevalence and risk of progression of light-chain monoclonal gammopathy of undetermined significance: a retrospective population-based cohort study. Lancet 375(9727): 1721-1728.
-
Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, et al. (2016) International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol 17(8): 328-346.
-
Mead GP, Drayson MT (2009) Sensitivity of serum free light chain measurement of residual disease in multiple myeloma patients. Blood 114(8): 1717.
-
Beauvillain C, Renier G, Jeannin P, Ifrah N, Chevailler A (2008) Apport diagnostique du dosage des chaînes légères libres sériques d’immunoglobulines pour l’exploration des gammapathies monoconales. RFL- Revue francophone des laboratoires 38(404): 37-50.
-
Mead GP, Carr-Smith HD, Drayson MT, Morgan GJ, Child JA, et al. (2004) Serum free light chains for monitoring multiple myeloma. Br J Haematol 126(3): 348-354.
-
de Moraes Hungria VT, A Syreeta, Kampanis P, MS Elyara (2016) Serum free light chain assays not total light chain assays are the standard of care to assess monoclonal gammopathies. Rev Bras Hematol Hemoter 38(1): 37- 43.
-
Barley K, Tindle S, Bagiella E, Jagannath S, Chari A (2015) Serum free light chain assessment early after stem cell transplantation as a prognostic factor in multiple myeloma. Clin Lymphoma Myeloma Leuk 15(9): 541-
-
Kühnemund A, Liebisch P, Bauchmüller K, zur Hausen A, Veelken H, Wäsch R, et al. (2009) ‘Light-chain escape- multiple myeloma’—an escape phenomenon from plateau phase: report of the largest patient series using LC-monitoring. J Cancer Res Clin Oncol 135: 477-484.
-
Rajkumar SV, Dimopoulos MA, Palumbo A, Blade J, Merlini G, et al. (2014) International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol 15(12): 538-548.
-
Singh G (2017) Serum Free Light Chain Assay and κ/λ Ratio: Performance in Patients with Monoclonal Gammopathy-High False Negative Rate for κ/λ Ratio. J Clin Med Res 9(1): 46-57.
-
Lee WS, Singh G (2018) Serum Free Light Chains in Neoplastic Monoclonal Gammopathies: Relative Under- Detection of Lambda Dominant Kappa/Lambda Ratio, and Underproduction of Free Lambda Light Chains, as Compared to Kappa Light Chains, in Patients with Neoplastic Monoclonal Gammopathies. J Clin Med Res 10(7): 562-569.
-
Radocha J, Pour L, Pika T, Maisnar V, Spicka I, et al. (2015) Multicentered patient-based evidence of the role of free light chain ratio normalization in multiple myeloma disease relapse. Eur J Haematol 96(2): 119-127.
-
Singh G (2017) Oligoclonal Pattern/Abnormal Protein Bands in Post Treatment Plasma Cell Myeloma Patients: Implications for Protein Electrophoresis and Serum Free Light Chain Assay Results. J Clin Med Res 9(8): 671-679.
-
Hutchison CA, Cockwell P, Stringer S, Bradwell A, Cook M, et al. (2011) Early reduction of serum-free light chains associates with renal recovery in myeloma kidney. J Am Soc Nephrol 22(6): 1129-1136.
-
Rajkumar SV, Kyle RA, Therneau TM, Clark RJ, Bradwell AR, et al. (2004) Presence of monoclonal free light chains in the serum predicts risk of progression in monoclonal gammopathy of undetermined signifcance. Br J Haematol 127(3): 308-310.
-
Michallet M, Chapuis-Cellier C, Dejoie T, Lombard C, Caillon H, et al. (2018) Heavy+light chain monitoring correlates with clinical outcome in multiple myeloma patients. Leukemia 32: 376-382.
-
Greil C, Ihorst G, Gaiser F, Salzer U, Bisse E, et al. (2017) The serum heavy/light chain immunoassay: a valuable tool for sensitive paraprotein assessment, risk and disease monitoring in monoclonal gammopathies. Eur J Haematol 99(5): 449-458.
-
Milani P, Palladini G, Merlini G (2016) Serum-free light- chain analysis in diagnosis and management of multiple myeloma and related conditions. Scand J Clin Lab Invest Suppl 245: 113-118.
-
Li W, Zhou JZ, Chang HR, Dai LJ, Zhu ZL, et al. (2015) Comparison of SPE, IFE, and FLC in Monitoring Patients with Multiple Myeloma After Autologous Stem Cell Transplantation. Cell Biochem Biophys 73(3): 643-647.
-
Wood PB, McElroy YG, Stone MJ (2010) Comparison of serum immunofixation electrophoresis and free light chain assays in the detection of monoclonal gammopathies. Clin Lymphoma Myeloma Leuk 10(4): 278-280.
-
Moustafa MA, Rajkumar SV, Dispenzieri A, Gertz MA, Lacy MQ, et al. (2015) Utility of Serum Free Light Chain Measurements in Multiple Myeloma Patients Not Achieving complete Response to Therapy. Leukemia 29(10): 2033-2038.
-
Kuriakose E, Narayanan Unni Cheppayil S, Kuzhikandathil Narayanan S, Vasudevan A (2019) A Study on Free Light Chain Assay and Serum Immunofixation Electrophoresis for the Diagnosis of Monoclonal Gammopathies. Ind J Clin Biochem 34(1): 76-81.
-
Jenner E (2014) Serum free light chains in clinical laboratory diagnostics. Clin Chim Acta 427: 15-20.
-
Hutchison CA, Basnayake K, Cockwell P (2009) Serum free light chain assessment in monoclonal gammopathy and kidney disease. Nat Rev Nephrol 5(11): 621-627.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies