The Challenge for Component Therapies
Blood Transfusion is a supportive or preventive hemotherapy focuse on pathophysiology due to deficiencies. Key is the threat of organ failure due to lacj of perfusion and oxygen delivery. Preferably blood as composite should be used in its composing elements, cells and plasma proteins. That means that the supply of blood products should answer the clinical demand based on the clinical need equal to the demand. In Most indications one should observe the pathophysiological response to deficiencies occurring, which usually takes around 24 hours before the bone marrow and the liver synthesis have come to full production of cells and proteins. There is therefore no need to replace all what has been lost or otherwise deficient.
Abbreviations
PDMPs: Plasma Derived Medicinal Products; HDN: Hemolytic Disease of the Newborn; SWOT: Strengths and Weaknesses, Opportunities and Threats; M&E: Monitor and Evaluate.
Introduction
Blood transfusion is a supportive or preventive hemotherapy focused on patho-physiology due to deficiencies (absolute or functional) of blood elements (cells and proteins). Key is the threat of organ failure which has a multi-causal origin, e.g., hemostasis, immunodeficiency, oxygen, inborn or acquired, trauma, surgical or obstetric.
Each of these causative conditions requires a specific approach, starting with diagnostic procedures including history and careful clinical observation, laboratory support, mechanical repair of ruptured or damaged vessels and application of simple though effective measures to compensate for the deficiency.
Blood as a Composite
Although human blood for transfusion is indeed a composite, it should preferably not be used as a composite but applied in its individual components. That requires an integration of procurement or manufacturing and used, an organisation where demand and supply are an integral part of this specific part of the health care system.
The demand reflects a rational use of the composite, considering the use of alternatives. The supply reflects an optimal use of the composite ‘whole blood’ to allow a rational therapeutic application. Optimal use means a policy to process the composite into its constituting elements, from simple separation of cells from plasma to an ultimate purification of cellular components (e.g., leukocyte depletion) and fractionation of proteins from plasma to produce plasma derived medicinal products (PDMPs).
The most important requisite of the individual components is in the preservation of the function of cells and proteins. The clinical demand is based on the assumption that the supply offers optimal therapeutic capacity. Red cells need to be able to transport and release oxygen, platelets should be able to form primary hemostatic clots. Proteins need to have a functionality as present in the streaming blood; albumin should be effective in colloid-osmosis; clotting factors should be effective in fibrin formation and immunoglobulins should provide humoral defence, e.g., anti-Rhesus D to prevent antibody formation and hemolytic disease of the newborn (HDN).
Deficiencies
When deficiencies develop, the levels of circulating elements diminish sometimes to such an extent that the balance becomes disturbed, the body defenceless and organs fail to function. That requires a careful clinical observation and follow up to allow identification of the risk zone for such severe morbidity to occur. Where there is still functioning hematopoiesis and active protein synthesis, there will be a compensating mechanism triggered to overcome the threat. However, when the deficiency develops faster than the compensating mechanism, the body and its organs will lose the battle and decompensate. So, there is a pathophysiological risk zone that should be observed as an ultimate trigger to transfuse the deficient component or compensate for the loss of function.
Alternatively, there may be a case for prevention of morbidity from deficiencies, such as in hereditary clotting factor deficiencies, e.g., Hemophilia, hemoglobinopathies such as Thalassaemia and acquired thrombocytopenia during cancer or leukaemia treatment.
Whole Blood
The old-fashioned idea of many clinicians that there should always be returned what has been lost is based on a simplistic understanding of the pathophysiology of blood loss, whether chronic or massive. Although bleeding does never occur per element of the composite, it does not mean that the clinical countering of loss of the composite should be transfusion of the intact composite, whole blood. Normal physiology learns that the concentration of proteins and cellular components embedded is the matrix plasma in whole blood is relatively low. In case of deficiencies supportive treatment with higher concentrations (blood products like platelet concentrates and cryoprecipitate) is needed.
In severe burn injury it is the massive protein coagulation on the burn wound surface, that causes the prime morbidity and unbalance, needing protein (plasma, albumin) transfusion to restore colloid-osmosis, hemostasis and humoral immune defence.
The Challenge
Prescription of supportive or preventive hemotherapy should be based on evidence, knowledge and experience. Prescription should also be based on a well-organized and properly facilitating health care infrastructure that encompasses both the demand and the supply parts of the chain.
Where there is a demand there is a need, and where there is a need, there should be a mechanism to satisfy or compensate that need (supply). The dynamics are not unilateral but bilateral. Offering blood components (products) without a need or a related demand does not make much sense. Requesting blood components (products) without a guaranteed and adequate response to supply is equally senseless. So, the dynamics represent a balance between the two, where the ‘markets’ are of equal importance – the supply as a market for the need, and the demand as a market for the supply.
Different Dimensions
There are, however, two other dimensions related to the balance of demand and supply:
- The first dimension is proper and individual patient care based on the old Hippocratic adagio: first do no harm. The body needs support with essential functions to restore and survive. That brings us back to the principles of physiology and pathophysiology, the knowledge and comprehension of the course of disease.
- The second dimension is with the source of the human blood. Blood as a special tissue for clinical supportive use is to be shared between individuals on an altruistic and moral-ethical ground. There is therefore a responsibility charge with the procurement organization responsible for the supply to ensure that the tissue voluntarily donated is not only processed and preserved optimally, but that the ultimate clinical use follows principles of rationality. It should not be wasted and not be abused. It should not be treated such that the essence of the composite elements is affected or used such that it fails to bring the expected clinical effects. This implicates an accountability of both the supplier and the consumer towards the donor or in general the public and the patient.
The Challenge for Component Therapy
To explore the challenge for component therapies both in resource limited and resource available countries, observational surveys of current practices together with explorative studies focused on knowledge and experience of prescribing clinicians are needed against the background of similar collection of information on the supply part of the chain – the procurement or manufacturing. Such approach follows the concept of an analysis of strengths and weaknesses, opportunities and threats (SWOT). These observational surveys and explorative studies would therefore reveal a SWOT analytical wealth of information on which a policy and related strategies for rational use of blood components in hemotherapy are to be developed. For benchmark reasons and evaluation of progress, regular repetition of these observational and explorative studies is an effective tool to monitor and evaluate (M&E) outcomes – a starting principle of evidence-based practice.
What Can Be Done?
Transfusion medicine is a bridging science and practice that spans the healthy community and the clinical care of those in need. It connects the source of safe and efficacious and quality-assured blood as a transplant with the ultimate rational application at the bedside.
The challenge of an optimal and rational therapeutic use of blood as a composite tissue is in the parallel and simultaneous development of the three key parts of the vein-to-vein chain – community, procurement and clinical use (Figure 1).
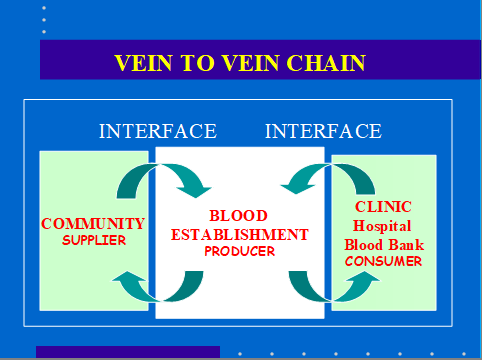
Each of these three key parts needs a special though health care integrated approach to allow an optimal and rational practice of transfusion medicine – a competent bridge function as an integral part of the health care system. The interfaces are between community and procurement or manufacturing, and between procurement or manufacturing and rational clinical use. Only when these realities are recognized, understood, implemented and applied in mutual respect and synergic application, will supportive hemotherapy become a true clinical blessing, especially in resource limited countries. Focusing only or predominantly on the bridge deck will lead to a technocratic laboratory- oriented development that would not find a proper market for the necessary qualities and quantities of the source - human blood as a supportive treatment commodity.
Alternatively, it will not find a proper and receptive ‘market’ for what technocratically has been produced and is offered – clinically effective and safe blood components that would allow a rational supportive or preventive hemotherapy to be practiced at the bedside.
Development
So, the development should be planned as a composite of these three key parts, each given equal and appropriate attention. However, the three parts have different complexities in their development.
The community needs a long term and intense social marketing approach to change culture and perception, and maintain the right mind set needed for a solid and sustained community support of the need.
The procurement needs a professional development based on principles of physiology and physics to understand what is needed to collect, process and preserve a tissue and its components to be used for transplantation. That is more than just blood grouping or testing for infectious disease markers. It needs a thorough understanding of the morphology and physiology of cells and proteins and the desired ex vivo environment to keep their functionality as optimal as possible over the processing and preservation time. It also needs an understanding of social behaviour and culture to access successfully and sustained the community source.
The clinical use will need a continuum of education through teaching and training of those involved in the clinical care. That must start at medical school to understand how blood as a transplant needs to be handled vein-to-vein to contribute to appropriate and integrated clinical care of the patient.
For each of these key parts an overarching quality management system must be put in place to secure consistence and fitness for use of the transplant from donor to recipient.
Conclusion The challenge for component therapy (patient blood care) is multifaceted –
- challenging the community to become aware of the principle of sharing as a social act,
- challenging the procurement institutions or blood establishments to change their island position into a competent and professionally built bridge connecting the source with the ultimate clinical use,
- challenging the prescribers to value and treasure the contribution of supportive and preventive hemotherapy in their clinical practices and account for the appropriate and rational use to donor, public and patient– the old Hippocratic adagio: primum est non nocere.
Reference
1. Smit Sibinga CTh, Jansen van Galen JP (2020) The Blood Supply – A special manufacturing process. In: Manufacturing Systems: Recent Progress and Future Directions. In: Mellal MA (Edn.), Nova Science Publishers 8: 165-186.
References
-
Smit Sibinga CTh, Jansen van Galen JP (2020) The Blood Supply – A special manufacturing process. In: Manufacturing Systems: Recent Progress and Future Directions. In: Mellal MA (Edn.), Nova Science Publishers 8: 165-186.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- Effect of Monoclonal Gammopathy on Risk of Kidney Failure among Patients with Chronic Kidney Disease