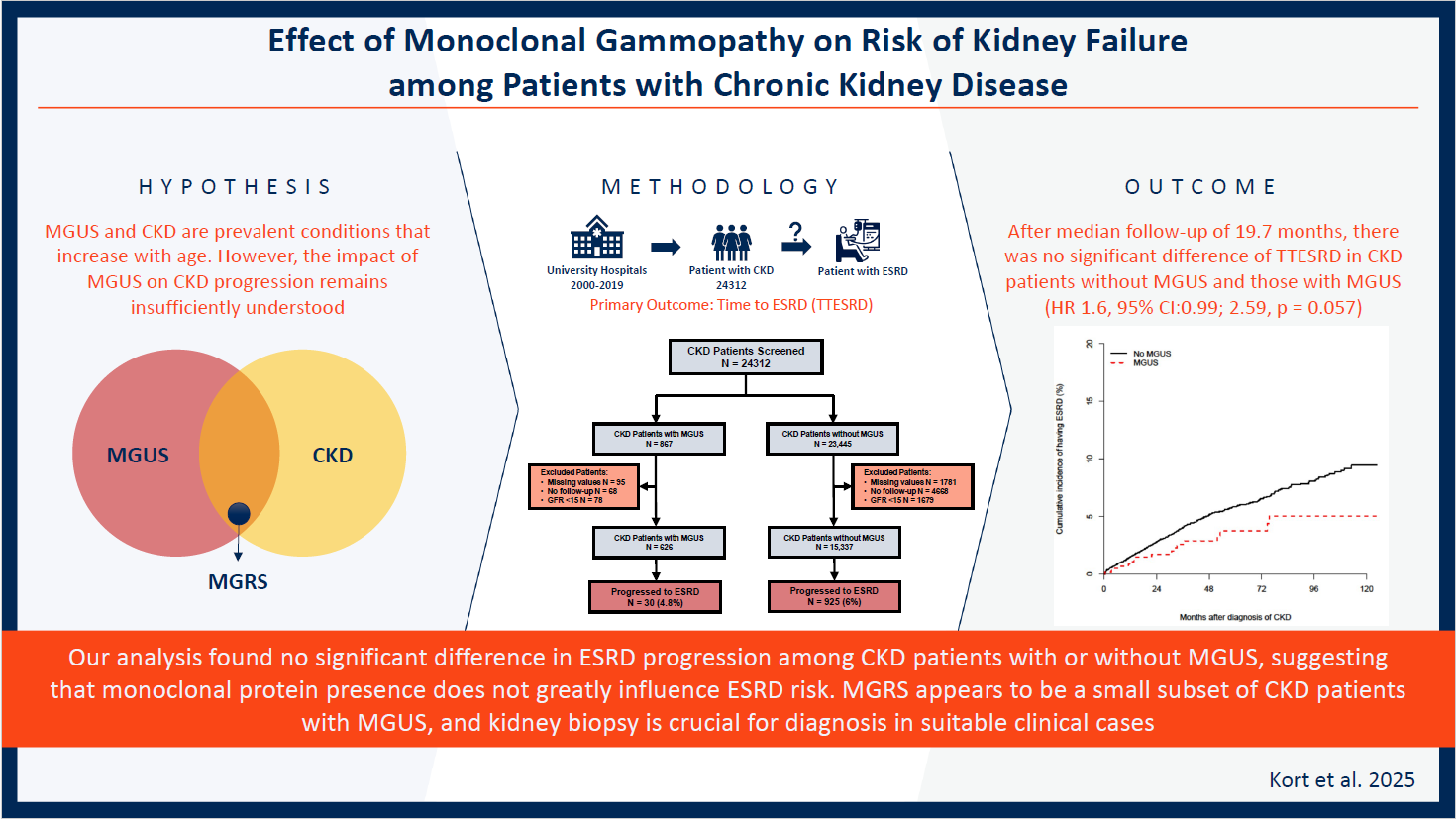
Effect of Monoclonal Gammopathy on Risk of Kidney Failure among Patients with Chronic Kidney Disease
Background: Monoclonal gammopathy of undetermined significance (MGUS) and chronic kidney disease (CKD) are common conditions. MG of renal significance (MGRS) represents a subgroup of MGUS in which monoclonal protein exerts deleterious effect on the kidney, and treating the underlying clone may help prevent progression to end stage renal disease (ESRD). However, the exact prevalence of MGRS remains largely unknown, and the significance of a positive monoclonal protein test in individuals with CKD is not well understood. Methods: We conducted a single-center retrospective analysis for patients with CKD between 2000 and 2019 and included 15,337 patients without MGUS and 626 patients with MGUS. The primary outcome was the rate of progression to ESRD, calculated using Time to ESRD (TTESRD). Results: After a median follow-up of 19.7 months, there was no statistically significant difference in the rate of ESRD between CKD patients with MGUS and those without MGUS (4.8% vs. 6%, p = 0.2). Considering the duration of follow-up and death as competing risks, there was no significant difference in TTESRD between both groups (HR 1.6, 95% CI: 0.99-2.59, p = 0.057). Even after adjusting for age, gender, race, CKD stage, diabetes, and hypertension, no significant difference in TTESRD was found between the two groups (HR 1.64, 95% CI: 0.99-2.72, p = 0.056). Conclusion: For most CKD patients, the identification of monoclonal protein did not provide additional information on the risk of ESRD. Our findings suggest that MGRS represents a small proportion of the overall population of patients with MGUS and CKD.
Abbreviations
CKD: Chronic Kidney Disease; ESRD: End Stage Renal Disease; UH: University Hospitals; GFR: Glomerular Filtration Rate; KDIGO: Kidney Disease Improving Global Outcomes; DM: Diabetes Mellitus; MGUS: Monoclonal Gammopathy of Undetermined Significance; GFR: Glomerular Filtration Rate; ESRD: End Stage Renal Disease.
Introduction
Chronic kidney disease (CKD) is a prevalent condition affecting around 15% of adults, equating to nearly 37 million individuals in the United States [1]. The prevalence of CKD increases with age, with 38% of those aged 65 years or older affected, compared to 12% of those 45-64 years of age. Additionally, CKD is more common in non- Hispanic, Black adults compared to non-Hispanic White or Asian adults. CKD patients face the possibility of their kidney function deteriorating over time, potentially leading to the development of End Stage Renal Disease (ESRD). The incidence of ESRD treated with dialysis or renal transplantation has risen by more than 90% from 1990 to 2016 [1]. Therefore, it is essential to implement strategies that can delay kidney deterioration and postpone or avoid ESRD for optimal patient outcomes.
While non-disease-specific interventions can slow down the CKD progression, addressing underlying pathologic process is of paramount importance [2, 3]. Examining serum or urine to detect monoclonal protein is performed frequently to rule out multiple myeloma (MM) as the causative factor [4, 5]. However, the presence of monoclonal protein often does not meet the standard criteria that define MM, including end-organ damage known as CRAB criteria (high calcium, renal failure, anemia, and bony lesions). In these cases, the hematologic disorder is more consistent with monoclonal gammopathy of undetermined significance (MGUS) rather than MM [4, 6, 7, 8]. MGUS is a common disease as well with increasing prevalence with age: 2.3% in ages 40-59, 6.2% in ages 60-79, and 12.9% in ages 80 and older [9].
This led to the identification of a new entity, as a subgroup of MGUS, termed “MG of Renal Significance” (MGRS), which represents any plasma cell disorder producing a nephrotoxic monoclonal protein that directly or indirectly results in kidney disease or injury, but the clinical picture does not fulfill standard MM diagnostic requirements [7, 10].
Although anti-myeloma treatment is generally not recommended for MGUS, targeting the plasma cell clone utilizing anti-myeloma therapies to suppress the circulating monoclonal protein could lead to preservation/restoration of kidney function in affected patients with MGRS. The true prevalence of MGRS remains mostly unknown due to the need for kidney biopsies for diagnosis, which are seldom performed, and there is frequently considerable ambiguity surrounding the clinical implications of finding a monoclonal protein in individuals with kidney disease [4, 5]. The incidence of MGRS is thought to be underdiagnosed, and there is much interest in better defining this entity given the treatable underlying renal pathology.
Currently, our understanding of the long-term outcomes of monoclonal protein associated with CKD remains limited. It is unclear whether a positive test result for monoclonal protein is associated with an increased risk of progression to ESRD among patients with CKD. Therefore, our study was designed to investigate the potential relationship between MGUS and the progression to ESRD in a large cohort of patients with CKD. This study aims to fill the knowledge gap by providing a better understanding of the clinical significance of finding MGUS in patients with CKD and could provide insights on the entire CKD and MGUS population and thus help to determine the relative health impact of MGRS among these prevalent conditions.
Patients and Methods
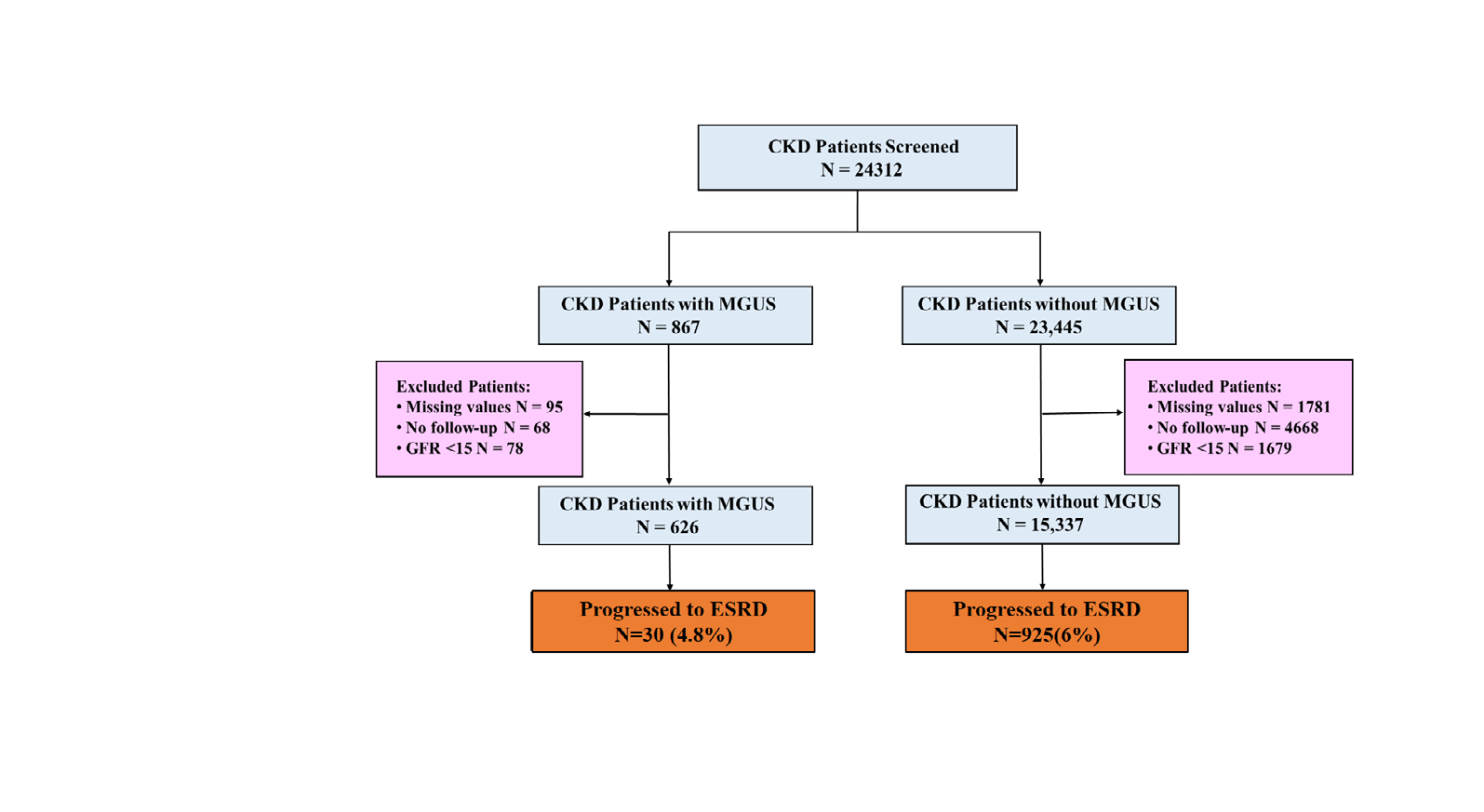
The study was approved by the Institutional Review Board at the University Hospitals (UH) Cleveland Medical Center, Cleveland, OH. Patients diagnosed with CKD (ICD 9: 585.X) from 2000 to 2019 were included in the study. Cases with diagnosis of MGUS (ICD-9: 273.1) were recognized. Baseline patient and disease characteristics were collected at the date of diagnosis with CKD, glomerular filtration rate (GFR) was collected at baseline, 1 year and 5 years following diagnosis. CKD stage was assigned according to the kidney disease: Improving Global Outcomes (KDIGO) guidelines. ESRD was defined as persistent eGFR<15 ml/min per 1.73 m2 or ICD 9 code 585.6. For each patient, the date of CKD diagnosis during this period served as the study baseline. For patients with MGUS, date of diagnosis of MGUS served as the baseline. We excluded all patients with missing GFR values (n=1876) patients who never had follow up (n=4716) and patients with GFR <15 ml/min per 1.73 m2 at baseline (n=1757). We also excluded patients with values of M-protein >3g/dl and FLC ratio> 100 as they fulfilled the diagnostic criteria for Multiple Myeloma. Final analysis included 626 Factor CKD without MGUS (n=15337) CKD with MGUS (n=626) p-value Freq. or mean % or std Freq. or mean % or std Age (year) 71.8 13.7 74.7 10.6 < 0.0001 Sex patients with MGUS and CKD and 15337 patients with CKD without monoclonal protein. The primary outcome was the rate of progression to ESRD, which was calculated using the Time to ESRD (TTESRD) to account for the duration of follow- up and death as competing risk. TTESRD was measured from the date of diagnosis of CKD to the date of diagnosis of ESRD and was censored at the date of last follow up. Overall survival (OS) was measured from the date of diagnosis of CKD to the date of death and was censored at the date of last follow-up for survivors.
Statistical Analysis: We compared patients with CKD and MGUS with patients who had CKD alone. The cumulative incidence of having ESRD was estimated with death as competing risk. The Fine and Gray method was used to compare the cumulative incidence of ESRD between groups [11, 12]. The effect of key factors on TTESRD were further evaluated using multivariable Fine and Gray method. Survivor distribution was estimated using Kaplan-Meier methods [13] and the difference of OS between/among groups was examined by log-rank test. The difference of continuous variables between groups was examined using T-test and the association between two categorical variables was examined using Chi-square test. All tests are two-sided and p-value ≤ 0.05 were considered statistically significant.
Results
A full description of patient demographics and characteristics is summarized in Table 1 and Figure 1. We included 626 patients with both MGUS and CKD and 15337 patients with CKD alone. The median age for patients with MGUS vs. patients without was 71.8 and 74.7 years old, respectively. Both cohorts had a similar male to female distribution of ~1:1. African Americans contributed to 33.5% of the total patient population that was evaluated. There was no significant difference detected between both groups in the frequency of diabetes mellitus (DM), however hypertension (HTN) was higher in patients with MGUS (87.5% vs. 80%; p = < 0.0001). Among the MGUS group, 453 out of 626 patients (72%) had a GFR lower than 60 mL/min, while among the non-MGUS group, 11,529 out of 15,337 patients (75%) had a GFR lower than 60 mL/min. There was a notably higher proportion of patients in the MGUS group who were at stage IV CKD upon recruitment (19.1% in patients with MGUS vs 14.5% in patients without MGUS p = 0.02).
| Female | 7654 | 49.90% | 326 | 52.10% | 0.287 |
|---|---|---|---|---|---|
| Male | 7683 | 50.10% | 300 | 47.90% | |
| Race | |||||
| Black | 5140 | 33.50% | 220 | 35.10% | 0.351 |
| White | 9746 | 63.60% | 383 | 61.20% | |
| Other | 451 | 2.90% | 23 | 3.70% | |
| Diabetes | 6914 | 45.10% | 302 | 48.20% | 0.119 |
| Hypertension | 12278 | 80% | 548 | 87.50% | < 0.0001 |
| Stage of CKD | |||||
| II | 3482 | 23.20% | 119 | 20.80% | 0.02 |
| IIIA | 4693 | 31.30% | 166 | 29% | |
| IIIB | 4652 | 31% | 178 | 31.10% | |
| IV | 2184 | 14.50% | 109 | 19.10% | |
| ESRD | 925 | 6% | 30 | 4.80% | 0.2 |
Table 1: Patient characteristics.
Among 626 patients with MGUS and CKD, 191 had heavy chain MGUS, of which only 19 patients had M protein >= 1.5g/dl. 104 patients had Kappa LC, and 11 had Lambda LC, the rest are unknown.
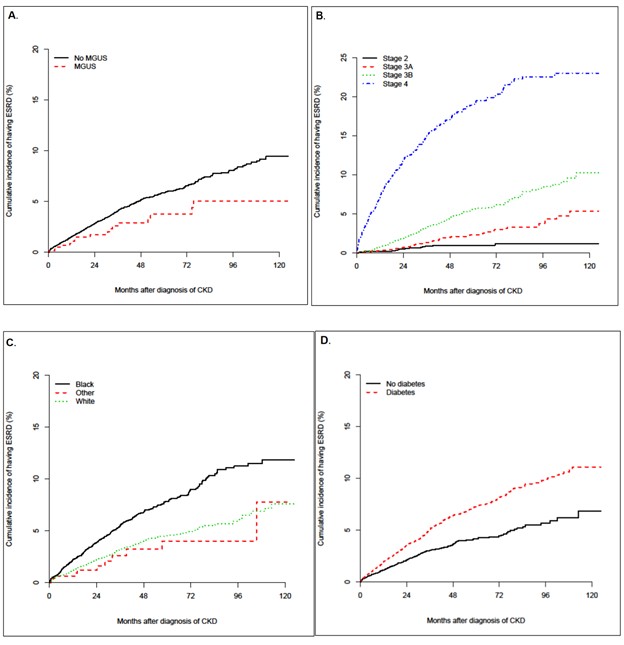
After a median follow up of 19.7 (range: 0.03-128) months, a total of 955 patients reached ESRD. There was no statistically significant difference in rate of ESRD between patients with CKD and MGUS and the patients with CKD without MGUS, 4.8% vs. 6%, respectively (p = 0.2). After including the duration of follow-up and death as competing risk, the unadjusted analyses showed no significant difference of TTESRD in patients who had CKD alone compared to patients who had both CKD and MGUS (HR 1.6, 95% CI:0.99; 2.59, p = 0.057). After controlling for effects of age, gender, race, CKD stage, diabetes and hypertension, there was still no significant difference of TTESRD between the two groups (HR 1.64 95% CI: 0.99, 2.72, p = 0.056). Multivariable analysis also demonstrated higher CKD stage (Stage IV) at baseline and male gender as significant factors associated with higher risk of developing ESRD. The hazard of developing ESRD was also significantly higher among African Americans compared to Caucasian patients (HR 1.49 95% CI: 1.24, 1.79, p < 0.0001). Older patients were also noted to be at a lower risk of developing ESRD in our cohort (HR 0.953 95% CI: 0.948, 0.96, p < 0.0001) (Table 2 and Figure 2).
| Factor | Univariate | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | |
| MGUS (No vs. Yes) | 1.6 (0.99, 2.59) | 0.057 | 1.64 (0.99, 2.72) | 0.056 |
| CKD Stage | ||||
| II vs. IV | 0.05 (0.03, 0.07) | < 0.0001 | 0.03 (0.02, 0.05) | < 0.0001 |
| IIIA vs. IV | 0.1 (0.07, 0.13) | < 0.0001 | 0.1 (0.07, 0.13) | < 0.0001 |
| IIIB vs. IV | 0.23 (0.2, 0.28) | < 0.0001 | 0.25 (0.2, 0.3) | < 0.0001 |
| Age (per year increase) | 0.96 (0.955, 0.963) | < 0.0001 | 0.953 (0.948, 0.96) | < 0.0001 |
| Gender (Female vs. Male) | 1.1 (0.93, 1.29) | 0.263 | 0.75 (0.62, 0.9) | 0.002 |
| Race | ||||
| Black vs. White | 1.81 (1.53, 2.13) | < 0.0001 | 1.49 (1.24, 1.79) | < 0.0001 |
| Other vs. White | 0.81 (0.44, 1.47) | 0.48 | 0.83 (0.45, 1.5) | 0.529 |
| Diabetes (No vs. Yes) | 0.56 (0.48, 0.67) | < 0.0001 | 0.6 (0.5, 0.72) | < 0.0001 |
| Hypertension (No vs. Yes) | 0.97 (0.77, 1.23) | 0.8 | 0.89 (0.68, 1.16) | 0.377 |
Table 2: Results from proportional hazard regression on TTESRD with death as competing risk.
The CKD stage at baseline was compared to the CKD stage at year 1 and year 5 during follow-up. The progression by stage was 28.5% at year 1 for patients without MGUS vs. 29.3% for those with MGUS (p = 0.73). The progression by stage was 38.7% at year 5 for patients without MGUS vs. 39.4 % for those with MGUS (p = 0.89). When patients were subcategorized according to baseline CKD stage, there was no difference in TTESRD, the odds of progression at year 1 neither year 5 between any of the groups.
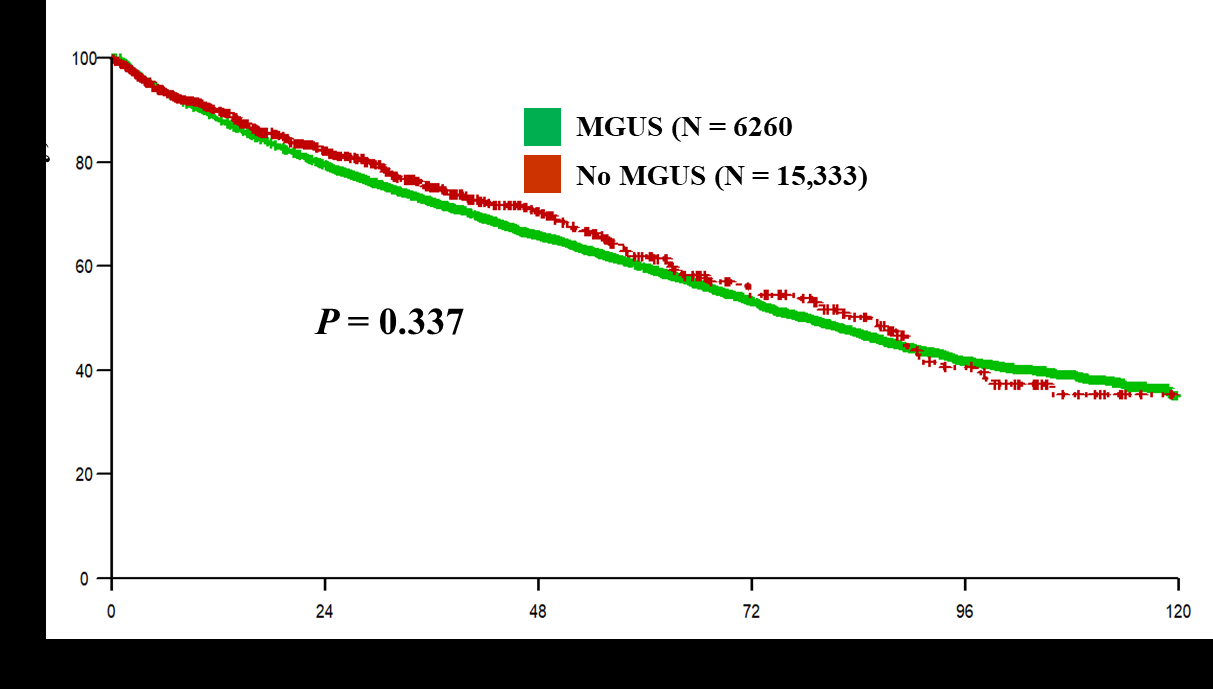
Median OS was 78.5 (95% CI: 74.6, 81.4) months for patients with CKD alone vs. 85.3 (95% CI: 71.6, 90.8,) months for those with both CKD and MGUS (p = 0.337). We did not detect any statistically significant difference between groups (Figure 3).
Among patients with MGUS and CKD, baseline serum albumin was predictive of progression of CKD at year one with odd ratio of 0.66 (95% CI: 0.46, 0.94) per unit increase of albumin. Baseline monoclonal protein was also predictive of progression of CKD at year five with odd ratio of 0.12 (95% CI: 0.02, 0.7) per unit increase. There was no significant correlation between monoclonal protein and GFR overtime (r = 0.09, p = 0.271). Furthermore, correlation between FLC and GFR was weak (r = - 0.11, p = 0.1).
Discussion
Our study utilized data for ~16,000 CKD patients and was acquired from a single institution and accumulated over 19 years. The data analyzed provided a granular view of patient co-morbidities as cofounding factors and did not detect a statistically significant association between a diagnosis of MGUS and the risk of progression to ESRD among patients with various stages of CKD. Given the large population included in our study, it benefits from high statistical power and low type II error. Therefore, the negative result of this study can be clinically significant. The incidence and health care burden of MGRS among patients with monoclonal protein and CKD remains largely unknown. This uncertainty frequently leads to undetermined pre-test probability of MGRS before kidney biopsy. This problem is more pronounced among CKD patients with monoclonal proteins with concomitant common nephropathies, i.e., HTN and DM. Given the invasive nature of kidney biopsy and the potential complications [14], a realistic incidence of MGRS and an accurate pre-test probability of this entity is an essential step toward optimal utilization of this procedure among this patient population. Our study suggests that the presence of MG alone in patients with CKD is not enough to suggest that the monoclonal protein is responsible for the kidney disease given the lack of monoclonal protein impact on CKD course based upon this large observational study.
MG-induced kidney damage can occur due to different mechanisms. Light chain cast nephropathy occurs in high tumor burden states such as MM which is usually accompanied by high levels of serum free light chain leading to tubal precipitation and formation of cast. MGRS-induced kidney injury on the other hand is thought to be caused by lower levels of serum monoclonal proteins via a variety of pathologic processes. The most common mechanism is misfolding of a fragment of monoclonal immunoglobulin heavy or light chain, causing toxic amyloid multimers and fibrils as is observed in AL Amyloidosis. Other mechanisms include deposition of a monoclonal protein in glomeruli triggering an immune complex reaction, direct toxic effect by monoclonal protein on cellular component in glomeruli, i.e., podocytes or mesangial cells, as well as certain mutations in monoclonal protein hampering recycling mechanisms leading to crystallization and aggregation [10]. Renal biopsy is an essential step to delineate an MGRS-defining pathology. Earlier studies have shown worse kidney outcomes in patients with confirmed MGRS. Patients with MGRS had an estimated renal survival of only 81.6% at 24 months follow- up after treatment [15]. Treatment of the underlying plasma cell clone has been suggested to improve renal survival, and the depth of hematological response appears to improve renal survival [16]. However, delayed diagnosis and the ambiguity around the need for renal biopsy have been among the main causes of poor outcomes in those patients [15].
Two prior studies assessed the association between MG and CKD, however, still there remains a wide gap in our knowledge in terms of the real significance of serum monoclonal protein. A large population-based study in Sweden compared survival patterns among patients with or without MGUS and showed an increased risk of dying from amyloidosis, bacterial infection, ischemic heart disease, liver failure and other hematologic malignancies as well as renal failure for patients with MGUS [17]. However, this study was limited by lack of information on potential confounders and lack of more detail clinic data, including co-morbidities leading to testing for MGUS. In another large cohort of US veterans in Veterans Affairs (VA) hospitals who had tested positive for monoclonal protein (i.e., including full blown MM), MG was associated with higher adjusted risk of ESRD in patients with either mild or severe reductions in GFR (15-29 ml/min). However, this correlation was not found in most patients, who had moderate reduction in GFR [18]. Importantly, the VA study included patients with MM that could have affected the results, given MM with high light chain levels is a clear cause of renal failure among this patient population. Furthermore, although it included high number of veterans, given the male dominance among VA patients, the generalizability of those findings to general populations might be limited. Our study delivers further insight that the presence of MG does not alter the progression rate toward ESRD among patients with CKD in a real-world setting.
Recently the iStopMM study, a large prospective population-based screening study of nearly 70,000 individuals in Iceland, found no association between MGUS and CKD. Additionally, they found no association between M protein concentration and GFR or severity of albuminuria. Participants with light chain MGUS were less likely to have CKD than participants without MGUS (OR 0.39, 95% CI 0.31–0.49, p <0.001) [19]. Although population studies screen everyone regardless of clinical symptoms, our study focuses on real-world scenarios where SPEP testing is based on clinical suspicion. This approach is essential to understanding the implications of SPEP testing in the routine care of CKD patients in clinical practice.
In another related study, Mendu et al. showed that serum protein electrophoresis, SPEP, while frequently performed, affected the diagnosis of only 1.4% patients and the management of only 1.7% patients with CKD [2]. Overall, these results suggest that the diagnosis of MGUS in patients with CKD provides limited information about the progression of kidney disease and renal survival. These data support that MGRS forms a small proportion of the whole MGUS population with CKD, and MG does not, by itself, increase the pre-test probability of MGRS diagnosis with kidney biopsy. Clinical judgment, e.g., parallel increase in monoclonal protein and decline in GFR longitudinally, remains crucial to early identify patients with high risk of having MGRS and refer them for kidney biopsy. Assessing the findings of our study in a prospective observational trial with histopathologic evaluation is warranted.
There was a notably higher proportion of patients in the MGUS group who were at stage IV CKD upon recruitment. We hypothesize that CKD patients with more advanced stages were more likely to be screened for MG than those with early stages, as this reflects the real-world practice. However, our multivariate analysis adjusted for CKD stage showed no difference in outcomes between the MGUS and non-MGUS groups. Furthermore, when we stratified the patients by baseline CKD stage, we found no difference in TTESRD, the odds of progression at year 1 or year 5 among any of the subgroups.
It is important to interpret our findings while considering the following limitations. First, these results are from a retrospective analysis of a large, single institution serving a diverse patient population that may not be generalizable to other populations. Second, we used ICD coding to define patients with CKD and MGUS, which may confer some diagnostic bias, by including patients who were mislabeled, or not labelled in a timely manner. Moreover, our CKD without MGUS cohort may not be completely free of MGUS, as not every patient was tested for this condition. However, this reflects the real-world scenario where MGUS screening is not routinely performed in CKD patients. Third, we also could not identify the reason for MG testing among our cohort, did not identify the patients whose diagnosis was confirmed with kidney biopsy and did not record the treatment patterns for CKD and the patients who received treatment for MGUS or who received kidney transplant, and lastly the follow up time was relatively short to determine the effect of progression to ESRD.
Conclusion
In conclusion, our retrospective analysis revealed no significant difference in the progression to ESRD between CKD patients with MGUS and those without it. This finding suggests that the presence of monoclonal protein does not substantially influence the risk of ESRD in most CKD patients. MGRS appears to constitute a small proportion of the CKD population with MGUS, and kidney biopsy remains crucial for diagnosis in the right clinical context.
Disclosures, Funding and Acknowledgments
The authors do not have any conflicts of interest to disclose. References
1. (2019) chronic kidney disease in the United States, 2019 fact sheet. CDC.
2. Mendu ML, Lundquist A, Aizer AA (2015) The usefulness of diagnostic testing in the initial evaluation of chronic kidney disease. JAMA Intern Med 175: 853-856.
3. Fermand JP, Bridoux F (2013) How I treat monoclonal gammopathy of renal significance (MGRS). Blood 122: 3583-3590.
4. Rosner MH, Edeani A, Yanagita M (2016) Paraprotein- related kidney disease: Diagnosing and treating monoclonal gammopathy of renal significance. Clinical Journal of the American Society of Nephrology. Published Online First.
5. Leung N, Bridoux F, Hutchison CA (2012) Monoclonal gammopathy of renal significance: when MGUS is no longer undetermined or insignificant. Blood 120: 4292-4295.
6. Heher EC, Rennke HG, Laubach JP (2013) kidney disease and multiple myeloma. Clin J Am Soc Nephrol 8: 2007-2017.
7. Leung N, Bridoux F, Batuman V (2019) The evaluation of monoclonal gammopathy of renal significance: a consensus report of the International Kidney and Monoclonal Gammopathy Research Group. Nat Rev Nephrol 15: 45-59.
8. Hogan JJ, Weiss BM (2016) Bridging the Divide: An Onco- Nephrologic Approach to the Monoclonal Gammopathies of Renal Significance. Clin J Am Soc Nephrol 11: 1681-1691.
9. Kristinsson SY, Rognvaldsson S, Thorsteinsdottir S (2021) Screening for Monoclonal Gammopathy of Undetermined Significance: A Population-Based Randomized Clinical Trial. First Results from the Iceland Screens, Treats, or Prevents Multiple Myeloma (iStopMM) Study. Blood 138: 156.
10. Leung N, Bridoux F, Nasr SH (2021) Monoclonal Gammopathy of Renal Significance. New England Journal of Medicine 384:1931-1941.
11. Fine JP, Gray RJ (1999) A Proportional Hazards Model for the Subdistribution of a Competing Risk. J Am Stat Assoc. Published Online First.
12. Robert J (1988) A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. The Annals of Statistics.
13. Kaplan EL, Meier P (1958) Nonparametric Estimation from Incomplete Observations. J Am Stat Assoc. Published Online First.
14. Trajceska L, Andreevska G, Vidimliski P (2019) Complications and Risks of Percutaneous Renal Biopsy. Open Access Maced J Med Sci 7: 992.
15. Khera A, Panitsas F, Djebbari F (2019) Long term outcomes in monoclonal gammopathy of renal significance. Br J Haematol 186: 706-716.
16. Jain A, Haynes R, Kothari J (2019) Pathophysiology and management of monoclonal gammopathy of renal significance. Blood Adv 3: 2409-2423.
17. Kristinsson SY, Bjorkholm M, Andersson TML (2009) Patterns of survival and causes of death following a diagnosis of monoclonal gammopathy of undetermined significance: a population-based study. Haematologica 94: 1714-1720.
18. Burwick N, Adams SV, Stenberg JA (2018) Association of Monoclonal Gammopathy with Progression to ESKD among US Veterans. Clin J Am Soc Nephrol 13: 1810-1815.
19. Einarsson T, Eythorsson E, Rognvaldsson S (2022) Monoclonal Gammopathy of Undetermined Significance and Risk of Chronic Kidney Disease: Results of the Population-Based Iceland Screens, Treats, or Prevents Multiple Myeloma (iStopMM) Study. Blood 140: 10108- 10109.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies