Thrombocytosis on Adult Patient with SARS-Cov-2 in Africa
The 2019-2020 pandemic caused by a novel coronavirus, SARS-Cov-2 or COVID-19 is ongoing. The outbreak of a respiratory illness caused by COVID-19 was first identified in Wuhan, Hubei Province, China and declared by the local authorities in December 2019. Since the beginning of the pandemic, Governments and health authorities across the world are striving to limit the widespread of the virus. The African continent registered its first cases about two months ago, and then readily implemented massive preventive measures such as lockdown, confinement and curfew. Like others, African Scientists are learning from and sharing their experiences about the disease. The aim of this article is to present a case of a COVID-19-related moderate pneumonia with unusual laboratory findings. This study has been approved by the local bioethics committee.
Case Report
A 38-year-old diabetic patient, on glicazide 60 mg daily, and a combination of Metformine 500+ Vildagliptine 50 mg twice daily, with a history of sarcoidosis that required a long term corticosteroid therapy was admitted on March 27, 2020 in a private clinic for a cough, shortness of breath and anosmia. The patient had traveled to Dubai 3 weeks before starting to show symptoms on March 20, 2020. At the time of admission, the patient reported anosmia and presented with high fever (T: 40 °C), tachypnea (RR: 28/min), insufficient oxygenation (ambient air saturation: 93%), the heart rate was normal: 98/ minute, W: 95kg, H: 169cm, BMI: .33.26Kg/ m2. Lungs auscultation revealed crackles in both bases. Cell blood count (CBC) showed a slight lymphopenia with 1.42 G/L, C-reactive protein (C-RP) was moderately elevated: 74.5mg/L, GGT as well: 135UI/L. The patient tested negative for Malaria, Dengue and Chikunguya Table 1. Differential diagnoses included flu and COVID-19. The patient was immediately isolated, received supplemental oxygen 3l/min (Figures 1 & 2).
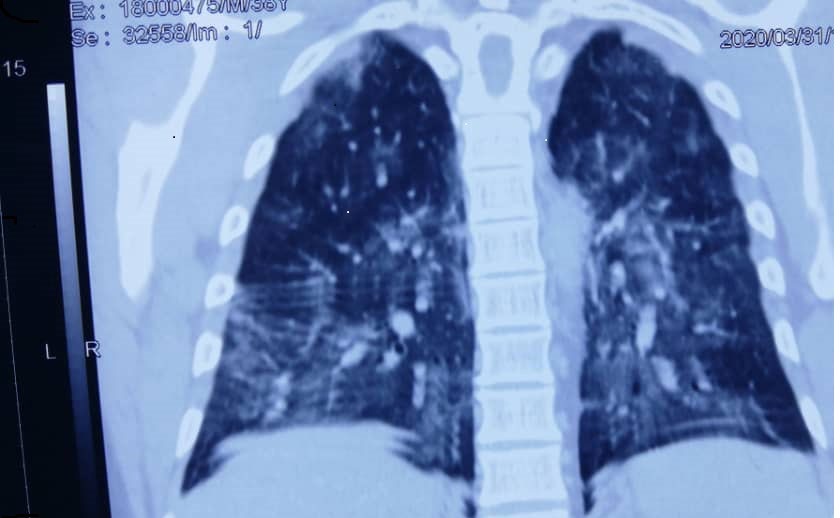
Figure 1
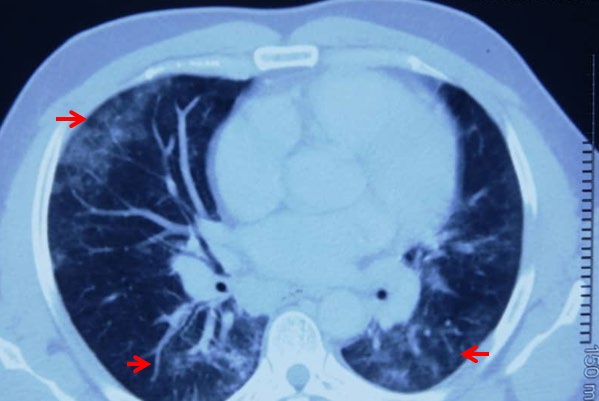
Figure 2 Figures 1,2: Chest C-T showed multifocal and bilateral pulmonary “ground glass “opacities in lungs suggestive for SARS-Cov-2 pneumonia.
RT-PCR from a pharyngeal swab confirmed SARS-Cov-2 infection. We concluded to a mild pneumonia due to COVID-19 and started therapy including liponavir-ritonavir during 10 days associated with azithromycin for 5 days and supportive parenteral treatment. The third day of the treatment, we noticed an improvement; there was no more shortness of breath. However, air ambient saturation remained low (92%) and the patient was still febrile (T: 39.6°C). The C-RP peaked at 269.9 mg/L. On day 7, the anosmia symptom was practically over. The physical was unremarkable, vital parameters were normal: T: 37°C, RR: 16, HR: 86, ambient air saturation: 98%. CBC revealed a thrombocytosis with 593G/L. The C-RP flagged at 5 mg/L. The next day the CBC revealed that the thrombocytosis kept increasing to reach its maximum at 609G/L, there was a discrete neutropenia with 1.72 G/L. The C-reactive protein kept decreasing at 3.5 mg/L. By day 16, two testings for the COVID-19 were performed 24 hours apart and were negative. The patient was declared recovered and was released Table 1.
| At the admission | Beginning of the treatment | Day 3 | Day 7 | Day 8 | Day 14 | |
|---|---|---|---|---|---|---|
| 03-30-2020 | 02-04-2020 | 06-04-2020 | 07-04-2020 | 13-04-2020 | ||
| Hemoglobin (13-17g/dL) | 15.7 | 13.9 | 13.9 | 17.1 | 15.5 | 13.8 |
| WBC(4.1-11.1 G/dL) | 4 | 7.3 | 7.3 | 5 | 4 | 4.7 |
| Neutrophile granulocyt (2.0-7.5 G/L) | 2.35 | 4.28 | 4.2 | 2.6 | 1.72 | 1.99 |
| Lymphocyt (1.5-4.0G/L) | 1.42 | 2.48 | 2.48 | 2 | 1.92 | 2.09 |
| Platelet (145-400 G/L) | 199 | 192 | 192 | 593 | 609 | 425 |
| CRP (<10 mg/L) | 74.8 | 199.7 | 269 | 5 | 3.5 | 1.3 |
| ALT (<45UI/L) | 107 | 28 | 32 | 25 | ||
| AST (<40UI/L) | 42 | 29 | 27 | 32 | ||
| GGT (<61 UI/L) | 135 | 138 | 140 | 125 | ||
| Creatinine (62- 115 umol/L) | 105 | 89 | 78 | 115 | ||
| Urea (3-7.5 mmol/L) | 5.8 | 3.8 | 3.5 | 6.1 | 6.1 | 3.5 |
| Sugar fasting (4.1-6.1 mmol/L) | 6.1 | 6.1 | 6 | 6 | 5.8 | 5.8 |
| Rapide malaria test | Negative | |||||
| Dengue, Chikunguya serologies | Negative |
Table 1: Overview of laboratory findings during SARS-Cov-2 course.
Discussion
Since January 2020 the WHO has declared the outbreak of a novel coronavirus in China (SARS-Cov-2 or COVID-19) as a global health emergency. The new disease made public by China in December 2019 rapidly spread across the globe and struck the African continent in March 2020. To date (April 29, 2020) nearly 34,610 cases have been reported in Africa, of which around 1,517 deceased from the COVID-19 and 11,180 reported recoveries [1]. In the Republic of Congo, the first case was declared on March 14, 2020. From March 14 to April 29 2020, 220 cases have been diagnosed COVID-19 positive, among them we accounted 9 deaths and 19 recoveries. So far, the lethality has been much lower than what had been predicted by the WHO. A younger demography, warmer weather and a lower density of the population are factors that may change some aspects of the disease on the continent.
We present here a case of COVID-19 with the aim of describing the clinical and biological features observed and then compare them with the case reports and studies performed in Asian and Western countries. This patient is the third symptomatic patient diagnosed with COVID-19 in Pointe Noire, the second largest city of the country (Republic of Congo). Despite having serious co-morbidities: acquired immunodeficiency (long term steroid) diabetes, obesity and sarcoidosis, the patient recovered while they are known to suffer more severely the clinical outcomes as compared to those without [2]. The pandemic spread in the Congo, endemic for malaria, during the regular flu outbreak season. All the three diseases share similar symptoms. It might at the beginning of the SARS-Cov-2 outbreak in the country delayed consultation and probably lead to misdiagnosis. Our patient consulted 8 days after the beginning of the symptoms for shortness of breath. The medium time from beginning of the symptoms to dyspnea ranges from 8 to 12 days [3, 4]. Cough and fever were constantly found in the first week of the course of the disease, as well as myalgia which was not displayed by our patient [2]. Instead, he presented an anosmia which is formally recognized as a symptom of COVID-19, resulting from an olfactory dysfunction [5].
CT imaging was made available before RT-PCR and showed suggestive images of SARS-CoV-2 pneumonia. Even though the Rt-PCR is the gold standard for the diagnosis of the disease, the place of the conventional imaging or CT when available in low resource countries where testing are limited should be explored for an early recognition of the disease.
There are significant knowledge gaps in the pathogenesis of COVID-19. The level of the interferon gamma induced protein 10, CXCL 10 may be predictive of the subsequent clinical course of the disease as well as the lymphopenia [2, 6, 7]. It is a common biological abnormality observed in patients with COVID-19 and its severity is a predictive factor for bad outcome [2, 6]. SARS-CoV-2 viral load usually peak within 5 to 6 days of symptoms onset. During that period other biomarkers may be observed as well.
The study of Mardani, et al. showed that high level of C-reactive protein, ALT, AST, LDH and neutropenia could be used to predict the presence of the COVID-19 [6]. Correlation between the viral load and the level of these biomarkers have not been confirmed. We observed an improvement of the symptoms in our patient when C-RP, ALT and AST plasma were highest. Perhaps other markers in patients with co- morbidities would better fit for monitoring. We observed a progressive thrombocytosis that we initially associated to the inflammatory syndrome despite the fact that the C-RP flagged down. We did a literature search in “PubMed” and” google Scholar” database. Thrombocytosis in the adult population has not been found to date to be associated with SARS-Cov-2 but common in patients with SARS-Cov. Yang, et al. found in that population an increase in thrombopoietin level in the plasma, which can provide a possible explanation of the genesis of the thrombocytosis [8]. The level is measured to be higher in the convalesced cases which was the status of our patient if based on the clinic.
Conclusion
Despite the slower progression of the COVID19 pandemic in Africa, our Clinical and biological findings are similar than those found in patients in Asian and Western countries. Imaging an useful tool for early diagnosis in countries were RT-PCR capacities are limited. The thrombocytosis and trend of biomarkers are the specificities of our report. They require further studies.
References
-
World Health Organization Regional Office for Africa.
-
Rodriguez AJ, Cordona Ospina JA, Guitiérrez Ocampo E, Villamizar Pena R, Holguin Rivera Y, et al. (2020) Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Medecine and Infectious Disease 34.
-
Yang M, Ng MH, Li CK, Chan PKS, Liu C, et al. (2008) Thrombopoietin levels increased in patients with severe acute respiratory syndrome. Thromb Res 122(4): 473- 477.
-
Huang C, Wang Y, Li X, Ren L, Zhao J, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395(10223): 497-506.
-
Wang D, Hu B, HU C (2020) Clinical characteristics of 138 hospitalized patients with 2019 novel Coronavirus- infected pneumonia in Wuhan, China. BMJ.
-
Hopkins C, Surda P, Kumar N (2020) Presentation of new onset anosmia during the COVID-19 pandemic. Rhinology 58(3): 295-298.
-
Mardani R, Vasmehjani AA, Zali F, Gholami A, Nasab SDM, et al. (2020) Laboratory parameters in detection of COVID-19 patients with RT-PCR; a diagnostic accuracy study. Archives of Academic Emergency Medecine 8(1):
-
Mason RJ (2020) Pathogenesis of COVID-19 from a cell biology perspective. European Respiratory Journal 55: 2000607.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies