Central Airway Obstruction due to Hematologic Malignancies, Diagnosis and Local Treatment - A Narrative Review
Background: Malignant hematologic diseases may present with rare features. One of these is the first manifestation as a central airway lesion whose symptoms could be mistaken for asthma, chronic obstructive pulmonary disease, non-resolving or recurrent pneumonia, foreign body inhalation or both acute and chronic heart failure. The age of onset of the symptoms does not help in the differential diagnosis, leaving the clinician with a diagnostic dilemma, frequently clarified by invasive sampling. Current evidence of this group of entities is based predominantly on case reports. The aim of this work is to report a non-systematic review of haematological pathologies that can present themselves as an obstruction of the central airways, the possible ways in which it is possible to diagnose and treat them locally. Methodology: This revision work is the result of a critical analysis of the existing literature, carried out by collecting the main bibliographic entries in different languages present in international scientific databases relative to the topic of interest. All the arguments have been elaborated by the authors and critically re-proposed, in a non-systematic way (narrative revision).
Introduction
Malignant hematologic diseases have typical usual presentations, but unfrequently can present with rare features. One of these is the first manifestation as a central airway or endobronchial lesion (EL), whose symptoms could be mistaken for asthma, chronic obstructive pulmonary disease, non-resolving or recurrent pneumonia, foreign body inhalation or both acute and chronic heart failure [1, 2, 3, 4]. The age of onset of the symptoms does not help in the differential diagnosis as both adult and paediatric cases have been described. [5, 6, 7]. This presentation represents a diagnostic dilemma, frequently clarified by thoracic imaging as chest X-ray or chest computed tomography scan and diagnosed by invasive techniques as bronchoscopy. Blood tests can promote diagnostic suspicion and highlight the severity of the underlying disease.
Current evidence of this group of entities is based predominantly on case reports. The purpose of this paper is to report a non-systematic review of the pathologies that can present with the morphological aspect of a central airway obstruction.
Central airway obstruction due to hematologic malignancies may develop because of:
- a localized primary lesion derived from a parietal layer
- direct invasion of mediastinal pathological lymphatic structures
- direct invasion of parenchymal pathological structures
- diffusion by the lymphatic route
- diffusion by the haematogenous route The characteristic aspects of radiologic imaging of an EL are [8, 9, 10]: • Complete atelectasis of a single or multiple lung lobes • An endoluminal exophytic lesion • Localized narrowing of the airway lumen The main differential diagnoses are [11, 12, 13, 14]: • Lung carcinoma or other malignant histotype • Benign tumor • Papillomatosis • Pulmonary tuberculosis • Fungal infection • Sarcoidosis • Vasculitis
Material and Methods
This revision work is the result of a critical analysis of the existing literature, carried out by collecting the main bibliographic entries in English, German and Spanish present in international scientific databases (Medline, PubMed, Scopus, Google Scholar), by keyword research (hematology, hematologic, lymphoma, myeloma, leukemia, myeloid, amyloid, lymphoproliferative, myeloproliferative, endobronchial, endotracheal, airway).
All the arguments have been elaborated by the authors and critically re-proposed, in a non-systematic way (narrative revision). The list of bibliographic entries, therefore, is not necessarily comprehensive but reflects the body of evidence deemed by the authors functional to the objectives of this article.
Discussion
Leukaemia
Infiltration by leukaemia cells can occur in many organs. However, the formation of a tumor mass is rare. Green et al, reported a large series of patients with leukaemia of all types; only 4 of 109 showed involvement of the bronchial mucosa [15].
Sajiai, et al. described the case of a 17-year-old farmer with no previous known diseases [16]. The patient was symptomatic for cough and fever. He had a subclavicular lymphadenopathy on physical evaluation. On chest x-ray a mediastinal mass and a pleural effusion were demonstrated. An EL contiguous to the mediastinal mass was described, which demonstrated both a compression and infiltration effect on the main bronchial branches. An endobronchial biopsy was diagnostic for a T phenotype monoclonal disease (membrane expression of anti-CD10 antibodies, anti-CD5 and anti-CD3). The study of bone marrow cytology confirmed the suspicion of T-acute lymphoblastic leukaemia.
Chronic lymphocytic leukaemia (CLL) pulmonary involvement is present in 40% of patients, but ELs are rare [17]. It manifests itself mostly as small lesions distally located in the bronchial tree. Infact, Nudel described a case-series of 19 patients. HRTC scans of the lungs showed anomalies located in the small airways and peripheral bronchi. The endobronchial sampled lesions revealed a mucosal infiltration by B-lymphocytes with a phenotype consistent with CLL [18]. More rarely proximal endobronchial polypoid lesions in the airways or a diffuse infiltration of the bronchial wall have been described [19, 20].
Hodgkin’s Lymphoma
Patients with Hodgkin’s lymphoma (HL) have a 40% likelihood of pulmonary involvement. It usually presents as a solitary lung mass, cavitary lung lesion, apical lung lesion with Pancoast syndrome or widespread involvement of the lungs, but presentation as an EL is very rare [21, 22]. Fewer than 100 cases of primary pulmonary HL have been described and it occurs predominantly in women with a bimodal age distribution, with the first incidence peak in the third decade, and the second being in the sixth/seventh decade [23]. A careful initial staging is necessary in order to confirm the absence of involvement of regional hilar or mediastinal lymph nodes and systemic disease.
Hoste, et al. firstly introduced in 1984 two criteria aimed at defining an endobronchial presentation of HL: 1) involvement of the lung, lobar or primary bronchus, with or without mediastinal involvement; 2) no evidence of extra-thoracic lymphoma at the time of diagnosis or for three months thereafter [24]. Instead in 1994 Tredaniel proposed two simplified criteria: 1) histopathological features consistent with Hodgkin’s disease; 2) bronchoscopy revealing endobronchial obstructing lesion [25, 26].
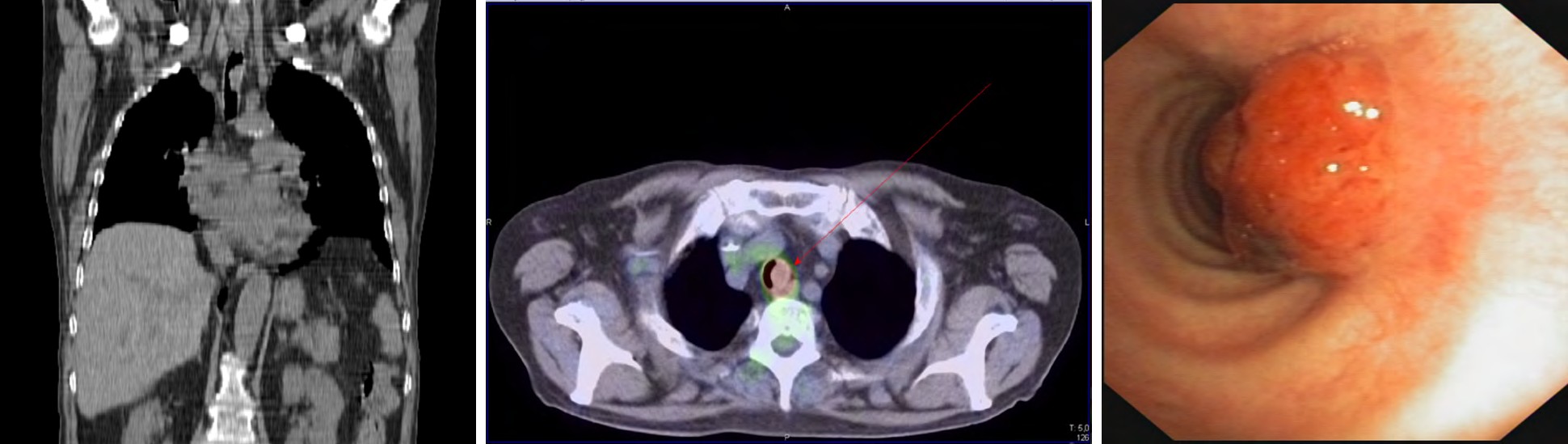
Shazia et al. illustrated the case of a 16-year-old patient with an EL found during the investigations for the relapse of a previous known HL. Bronchoscopy revealed a necrotic endobronchial mass. The first sampling was non-diagnostic and on the basis on the strong suspicion for malignant disease, it was repeated showing CD-30 positive HL cells, underlying the need to maintain a high level of suspicion towards these kind of lesions [27]. Abid, et al. [21] described a similar case in a 40-year-old-man, with concomitant HL skeletal metastasis at the time of diagnosis, stressing the importance of a complete initial staging. In a personal case (Figure 1) a mixed cellularity HL was diagnosed by endobronchial biopsy in a 60-year-old male as an EL located in the proximal sector of the right superior bronchus (non-published data). Biopsy confirmed a CD30, PAX5 e MUM1 immunoreactivity.

Non-Hodgkin’s Lymphoma
Most of the extra nodal presentations of non-Hodgkin’s lymphoma (NHL) involve skin, stomach, brain, and small intestine [28]. The NHL group represents the entities with the largest volume of pubblished evidence regarding presentation as an EL, both in the adult and paediatric age. NHL of the lung encompasses 3.6% of extra nodal lymphomas and 0.3% of primary lung neoplasms [29]. Reports vary as to how stringent the inclusion criteria for defining EL are. The most common histological subtype of primary pulmonary lymphoma (PPL) is that of indolent lymphoma mainly of mucosa-associated lymphoid tissue (MALT) type [30].
Endobronchial NHL can be divided into two types: 1) submucosal infiltrates originating from haematogenous or lymphangitic spread in the presence of systemic lymphoma; 2) adjacent airway involvement by a localized mass due to direct spread from adjacent lymph nodes [29]. Primary isolated endobronchial NHL is rare, with very few reports in the current literature. An accurate staging, considering the indication for complete blood count, bone marrow and cerebral spinal fluid evaluation, selective computed tomography, magnetic resonance imaging and skeletal scintigraphy should follow the diagnosis [31].
Endobronchial mucose-associated lymphoid tissue (MALT) lymphomas are considered to be the most frequent type of primary pulmonary lymphoma (PPL) [32]. Lymphomas of the bronchus associated lymphoid tissue (BALT) can be observed in the 25-85 year age group, often involving patients within the sixth decade of life and affecting both sexes with the same incidence [33]. The presenting thoracic CT findings have been described as three patterns: 1) solitary intraluminal nodule; 2) several tiny nodular protrusions; and 3) diffuse wall thickening [10]. Erbaycu published the case of a 32-year-old woman admitted for dyspnoea on exertion and different polypoid ELs in the left main bronchus with a diagnosis of low-grade BALT lymphoma, the patient did well with systemic therapy [34]. Hashemi presented a 61 year-old man with a localized EL in the right lower bronchus and consensual atelectasis the right lower lobe. On fiberoptic bronchoscopy, the right bronchus intermedius was completely obstructed by an easily bleeding mass. A diagnosis of BALT lymphoma was made. The surgical route was not considered, as pneumonectomy would have been indicated due to the proximity to the right main bronchus. The patient was then treated with radiotherapy (total 30 Gy), resulting in total remission of the tumour [35]. Liao described a 85-yar old woman presenting with haemoptysis, diffuse intrabronchial nodularity and responsive to rituximab therapy [36].
Hardavella, et al. illustrated the case of an 80-year-old man with a prior history of prostate cancer with a right main bronchus occlusion and mediastinal lymphadenopathy. A large mass sampled during bronchoscopy revealed a large B-cell NHL, showing how central airways malignant hematologic diseases should be taken in consideration even in older patients with a previous a previous malignancy in their medical history [37]. Other descriptions of endobronchial large B-cell NHL both as infiltration from a mediastinal mass and a primitive EL have been published by Sahin [38], Thomas [39], Solomonov [40], Zamboni [41], Sousa [42], Han [43], Meka M, et al. [44]. Argüder, et al. instead illustrated an interesting case in which a patient treated for Hodgkin’s lymphoma 18 years earlier developed a B-phenotype NHL with diffuse endobronchial distribution, which was found to be very well responsive to chemotherapy [45].
Anaplastic large cell lymphoma (ALCL) commonly presents as a nodal disease, but Bhalla described a the presentation as a lung mass with focal bronchial infiltration [5]), while Chen published a case with a primitive distal tracheal involvement treated with chemotherapy since both upper and lower diaphragm lymph nodes and bone structures were involved at initial staging [46]. Kanthan, et al. described the case of paediatric primary ALCL, presenting as a right main bronchus lesion causing complete right lung atelectasis and firstly diagnosed as an Ewing Sarcoma. In fact, approximately 80% of ALK-positive ALCLs express CD99, an antigen also present in Ewing’s sarcoma, highlighting how the quality and quantity of the histological material must be sufficient for the pathologist to carry out all the necessary investigations [47]. An aspect to underline again for ALCL is the need to obtain sufficient tissue material in order to evaluate both the immunohistochemical aspects and the translocation state of the ALK gene, as its expression is an important prognostic factor [48]. Of peculiar interest is the report by Mikowski, describing the case of a 60-year-old man with LLC and recurring lingular pneumonia who on bronchoscopy was found to have an EL whose specimens oriented for a diagnosis of ALCL, consistent with Richter’s
transformation. The mass was treated with Nd-YAG laser to restore airway patency and with subsequent chemotherapy [3].
Burkitt’s lymphoma causes some of the most aggressive manifestations of haematological disorders within the central airways. This type of lymphoma very often affects young patients, with a non-negligible percentage of HIV- positive individuals [49]. From the endoscopic point of view, they cause obstructing lesions with rapid dimensional evolution and occasional immediate risk to life. In a personal case (Figure 2) a diagnosis was made during an emergency rigid bronchoscopy for acute dyspnoea in a patient with a central airway lesion (non-published data). The obstruction was relieved using laser devascularisation followed by a coring out technique. The tissue evaluation confirmed Burkitt’s lymphoma.
Reports relating to mantle cell lymphoma (MCL) are quantitatively meager but noteworthy. The first report was proposed by Figgis [50], then Miyoshi brought to the attention the case of a 70-year-old woman whose cause of death was a rapidly progressive respiratory failure due to diffuse stenosis of the major bronchi of both lungs due to intramural and intraluminal infiltration of MCL cells [51]. This type of lymphoma presents with a diffuse distribution within the central airways, with easily bleeding lesions which are difficult to treat locally by endoscopic techniques, as reported by Katono [52].
Pulmonary T-cell lymphomas (PTLD) are more rarely described as EL. The first case was reported by Ferrer who concluded that T-cell lymphomas may present as an EL before the skin manifestations even appear [53]. Another PTLD case presented as an EL was described by Matsumoto in association with chronic pyothorax [54].
Plasmacytoma
Extramedullary plasmacytoma (EMP) is an uncommon condition defined by the presence of neoplastic plasma cells outside the bone marrow. It typically affects the head and neck region, and central airway involvement is very rare [55]. Bussy published the case of a 58-year old man with a history of multiple myeloma, presenting with pulmonary nodules and a central EL extended from the proximal bronchus intermedius to the right lower lobe bronchus. The biopsy suggested the tumor was of plasma cell origin with light chain restriction [56]. Local therapy for this entity has been proposed by Brackett, who performed the first documented laser treatment in an endobronchial plasmacytoma [57]. In the case exposed by LeNoir surgery was performed due to a non-diagnostic bronchial biopsy. A mediastinal lymphadenectomy and a workup for multiple myeloma were performed too and were negative [58].
Amyloidosis
Amyloidosis is characterized by the abnormal extracellular deposition of insoluble fibril proteins. The localized form is limited to a single organ such as bladder, skin, heart, or lung [59]. Most cases of respiratory amyloidosis have been described in three forms: 1) diffuse interstitial amyloidosis; 2) nodular parenchymal amyloidosis; 3) tracheobronchial amyloidosis [60]. Most of the clinical cases in the literature were initially diagnosed as bronchial asthma [61]. Tanriverdi described the case of a 68-year-old followed for non-responsive asthma for two years. A chest CT was performed, showing a tracheal exophytic lesion. Histopathological evaluation revealed that the mass was consistent with a diagnosis of tracheobronchial amyloidosis. The patient underwent rigid bronchoscopy and the lesion was removed by mechanical resection following both Nd- YAG laser and argon plasma coagulation [60]. Lal published a similar case, initially diagnosed as bronchial asthma. Following a CT scan of the chest, bronchial thickening with calcification of the wall and moderate stenosis of the left upper lobe was reported. Fiberoptic bronchoscopy was done, which showed a yellowish colour, nodular tumor like lesion in left upper, lobe bronchus. A biopsy showed pink amorphous material with green birefringence under polarized light, suggesting amyloidosis. Serum and urine electrophoresis, autoimmunity and an echocardiogram showed no significant findings and the patient was diagnosed with primary localized endobronchial amyloidosis [62]. Other reports descbribe a diffuse bronchial thickening as the first presentation modality [63]. Fiorelli described a case in which an endobronchial laser resection was performed for therapeutic purposes with the subsequent positioning of a self-expanding tracheo-bronchial metal stent [64].
Diagnosis
The diagnosis of central airways hematologic malignancies is a challenge in the clinical practice because symptoms and radiological findings are always non- specific. The appearance of respiratory symptoms (dry or productive cough, dyspnea, haemoptysis, chest pain or stridor) especially of subacute onset in haematological patients or with suspected haematological pathology should induce prompt evaluation with imaging techniques (chest X-ray, chest computed thomography scan, positron emission tomography) and functional respiratory tests as spirometry. Common clinical feature of haematological diseases as cervical and axillary lymphadenopathies, fever, weight loss, night sweats and recurrent infections may be presenting features as well. After careful evaluation for potential infectious aetiologies, the diagnosis for an EL has to be considered, since early intervention can be curative [65]. The presence of a radiological diagnosis of pneumonia does not exclude the presence of an EL as the infectious events are favoured by bronchial occlusion, by the immunosuppression induced by the underlying disease and by chemotherapy or immunosuppressive therapy if already started [3].
Functional respiratory test will show an obstructive functional pattern due to both focal polypoid lesions and diffuse narrowing of the bronchial lumen [18]. Once the suspicion of an EL becomes concrete, bronchoscopy allows the localization and sampling aimed at the final diagnosis. Both bronchoalveolar lavage, cytological and histological samples can be acquired in order perform tissue diagnostic tests, to look for clonality and immunophenotype [66].
Local Treatment
After careful initial staging, the patient is evaluated for the indication of induction therapy or a more intensive consolidation cycle. Although hematologic diseases are frequently not considered surgically approachable, there is a role for local intervention in the management of these diseases and a consultation with the pulmonology team should be considered. Interventional pulmonology procedures are the gold standard in this setting as airway interventions offer therapeutic benefit when other modalities of treatment are limited. The goal can be both curative and palliative in order to improve quality of life, relieving dyspnoea and resolving recurrent infectious episodes.
Rigid Bronchoscopy and Laser Therapy
Bronchoscopy is the mainstay to approaching an EL under direct vision and it allows tissue sampling. Rigid bronchoscopy is a traditional procedure, which must be performed under general anaesthesia [67]. It allows complete control of the patient’s airway and allows the passage of larger instruments and cameras to diagnose and treat airway disease [68, 69]. The rigid barrel of the rigid bronchoscope has a bevelled tip which allows resection of the exophytic lesions present within the airways, while ensuring a local haemostasis mechanism given by the compression of the metal body of the instrument on the mucosa [70].
Thermal laser vaporization treatment has been reported as a successful method of relieving central airway obstruction [71]. The laser beam-induced coagulation helps with the devascularisation of the lesion favouring its subsequent mechanical removal. In fact, bronchial debulking is safer and more rapid if laser therapy is combined with mechanical coring, which allows the resection of the EL, in turn reducing the need for laser-time-exposure [72, 73]. For peripheral lesions treated with a flexible bronchoscope, the laser can carbonise the lesion, which is then removed with biopsy forceps or a cryoprobe [74, 75, 76]. The evidence is stronger for non-small and small cell lung cancer, but tumor localization, morphology and respiratory symptoms are similar in endobronchial hematologic malignancies and the same treatments could be proposed if the patient is adequately informed.
Photodynamic Therapy
The premise of photodynamic therapy (PDT) is the selective retention of a porphyrin by tumor cells. When activated by laser light at the proper wavelength, this agent generates toxic oxygen-free radicals, which in turn cause tumor necrosis. Photodynamic therapy has been proven an effective modality for treating bronchogenic carcinoma and oesophageal carcinoma [77].
Bahram, et al. described the case of an endobronchial presentation of nodular sclerosing classic Hodgkin lymphoma, treated with PDT aimed at relieving the obstruction before induction of specific therapy [78].
Stenting
Endobronchial stenting is a palliative temporary or definitive solution for central airway lesions [79, 80]. Stenting can be proposed as a rapid solution to progressing dyspnoea and must be associated with tumor-specific therapy. Stent removal following specific therapy must always be considered in order to improve the quality of life of the patient and mitigate the risk of stent migration after a significant response to systemic therapy, causing the shrinkage of the malignant lesion. Schmidt et al. described 5 consecutive cases in patients with malignant lymphoma who presented with severe dyspnoea. Nine stents were implanted into the trachea or main bronchi. After stenting, patients underwent tumor-specific therapy. In 4 patients (80%), stents could be removed after successful tumor-specific therapy, which led to an improvement in the size of the stenosis after an average interval of 26 days [81].
Conclusion
Because of the dramatic prognostic implications, an endobronchial presentation of a hematologic malignancy, despite its uncommon occurrence, should be considered in the differential diagnosis of a central airway lesion, especially in a patient with cough, haemoptysis, atelectasis, hilar, or mediastinal lymphadenopathy. Bronchoscopy and adequate tissue sampling play the central role in diagnostics. Due to the rarity of these lesions, guidelines for management are largely consensus-based rather than evidence-based and the optimal therapy remains to be determined. Before, in conjunction with or following tumor-specific therapy, palliative treatment to relieve respiratory symptoms associated with the critical airway obstruction should be undertaken at tertiary centres with experience in rigid bronchoscopy, laser therapy, and advanced endoscopic techniques.
References
-
Akça A, Karadoğan M, Yildiz DK, Çorapçioğlu F, Anik Y (2015) Endobronchial recurrence of non-Hodgkin’s lymphoma mimicking foreign body aspiration. Interv Med Appl Sci 7(3): 129-131.
-
Pinto LM, Udwadia ZF (2009) A 12-year-old girl with Hodgkin’s disease presenting as a non-resolving pneumonia and an endobronchial nodule. The Indian journal of chest diseases & allied sciences. 51(4): 241- 243.
-
Milkowski DA, Worley BD, Morris MJ (1999) Richter’s transformation presenting as an obstructing endobronchial lesion. Chest 116(3): 832-835.
-
Pavlov N, Pavlov V, Culić S, Armanda V, Siebert R, et al. (2013) Endobronchial ALK+ anaplastic large-cell lymphoma resembling asthma in a 13-year-old girl. J Pediatr Hematol Oncol 35(1): 4-6.
-
Bhalla R, McClure S (2003) Pathologic quiz case: a 17-year-old adolescent girl with a short history of dyspnea. Endobronchial, anaplastic large cell lymphoma, T-cell phenotype. Arch Pathol Lab Med 127(12): 430- 431.
-
Escobosa Sánchez OM, Herrero Hernández A, Acha García T (2009) Endobronchial anaplastic large cell lymphoma in childhood. Anales de pediatria (Barcelona, Spain: 2003) 70(5): 449-452.
-
Kobayashi T, Hyodo M, Honda N (2013) Primary endobronchial Burkitt’s lymphoma in a child: a case report. Int J Pediatr Otorhinolaryngol 77(5): 875-878.
-
Calvillo Batllés P, Carreres Polo J, Sanz Caballer J, Salavert Lletí M, Compte Torrero L (2015) Hematologic neoplasms: interpreting lung findings in chest computed tomography. Radiologia 57(6): 455-470.
-
Filly R, Blank N, Castellino RA (1976) Radiographic Distribution of Intrathoracic Disease in Previously Untreated Patients with Hodgkin’s Disease and Non- Hodgkin’s Lymphoma. Radiology. 120(2): 277-281.
-
Yoon RG, Kim MY, Song JW, Chae EJ, Choi CM, et al. (2013) Primary endobronchial marginal zone B-cell lymphoma of bronchus-associated lymphoid tissue: CT findings in 7 patients. Korean J Radiol 14(2): 366-374.
-
Harris B, Geyer AI (2017) Diagnostic Evaluation of Pulmonary Abnormalities in Patients with Hematologic Malignancies and Hematopoietic Cell Transplantation. Clin Chest Med 38(2): 317-331.
-
Choi MH, Jung JI, Chung WD, Kim YJ, Lee SE, et al. (2014) Acute Pulmonary Complications in Patients with Hematologic Malignancies. RadioGraphics 34(6): 1755- 1768.
-
Chen GL, Wu CH, Perng WC (2017) Endobronchial Lesion in Eosinophilic Granulomatosis with Polyangiitis. Iran J Allergy Asthma Immunol 16(6): 561-564.
-
Corsello BF, Lohaus GH, Funahashi A (1983) Endobronchial mass lesion due to sarcoidosis: complete resolution with corticosteroids. Thorax 38(2): 157-158.
-
Green RA, Nicholas NJ (1959) Pulmonary Involvement in Leukemia. American Review of Respiratory Disease 80(6): 833-844.
-
Sajiai H, Fikal S, Serhane H, Aitbatahar S, Amro L, et al. (2015) Endobronchial location of acute lymphoblastic leukemia phenotype T. Pan Afr Med J 21: 5.
-
Berkman N, Polliack A, Breuer R, Okon E, Kramer M (1992) Pulmonary Involvement as the Major Manifestation of Chronic Lymphocytic Leukemia. Leuk Lymphoma 8(6): 495-499.
-
Nudel M, Baran Marszak F, Bossard JB, Dubois R, Dapvril H, et al. (2019) Characterisation of a new clinical presentation of chronic lymphocytic leukaemia: symptomatic bronchial involvement, a study from the FILO group. Br J Haematol 186(5): 126-130.
-
Maw M, Harvey M, Harrington Z, Baraket M, Montgomery R, et al. (2015) Endobronchial deposits of chronic lymphocytic leukemia-an unusual cause of central airway obstruction. Respirol Case Rep 3(2): 41-43.
-
Chernoff A, Rymuza J, Lippmann ML (1984) Endobronchial lymphocytic infiltration: Unusual manifestation of chronic lymphocytic leukemia. The American Journal of Medicine 77(4): 755-759.
-
Abid HM, Khan JM, Lone NM (2018) Hodgkin’s Lymphoma presenting as an obstructing endobronchial mass-A rare presentation. BMJ Case Rep 2018.
-
Montero C, Deben G, de la Torre M, Álvarez A, Verea H (2004) Síndrome de Pancoast e infiltración tumoral endobronquial como primera manifestación de un linfoma de Hodgkin. Archivos de Bronconeumología 40(6): 287-289.
-
Lluch Garcia R, Briones Gomez A, Castellano EM, Sanchez Toril F, Lopez A, et al. (2010) Primary pulmonary Hodgkin’s lymphoma. Canadian respiratory journal 17(6): 106-108.
-
L Hoste RJ, Filippa DA, Lieberman PH, Bretsky S (1984) Primary pulmonary lymphomas. A clinicopathologic analysis of 36 cases. Cancer 54(7): 1397-1406.
-
Malur PR, Gaude GS, Bannur HB, Anurshetru SB, Suranagi VV, et al. (2009) Primary endobronchial Hodgkin’s disease. Lung India: official organ of Indian Chest Society 26(4): 136-138.
-
Trédaniel J, Peillon I, Fermé C, Brice P, Gisselbrecht C, et al. (1994) Endobronchial presentation of Hodgkin’s disease: a report of nine cases and review of the literature. Eur Respir J 7(10): 1852-1855.
-
Awan S, Wahla AS (2014) An unusual presentation of endobronchial Hodgkin’s lymphoma. J Coll Physicians Surg Pak 24(3): 221-223.
-
Chua SC, Rozalli FI, O Connor SR (2009) Imaging features of primary extranodal lymphomas. Clinical radiology 64(6): 574-588.
-
Rush WL, Andriko JA, Taubenberger JK, Nelson AM, Abbondanzo SL, et al. (2000) Primary anaplastic large cell lymphoma of the lung: a clinicopathologic study of five patients. Mod Pathol 13(12): 1285-1292.
-
Cadranel J, Wislez M, Antoine M (2002) Primary pulmonary lymphoma. European Respiratory Journal 20(3): 750-762.
-
Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, et al. (2014) Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non- Hodgkin lymphoma: the Lugano classification. J Clin Oncol 32(27): 3059-3068.
-
Zucca E, Bertoni F (2016) The spectrum of MALT lymphoma at different sites: biological and therapeutic relevance. Blood 127(17): 2082-2092.
-
Thieblemont C, Berger Fo, Dumontet C, Moullet I, Bouafia F, et al. (2000) Mucosa-associated lymphoid tissue lymphoma is a disseminated disease in one third of 158 patients analyzed. Blood 95(3): 802-806.
-
Erbaycu AE, Karasu I, Ozdemirkiran FG, Yücel N, Ozsöz A, et al. (2004) Endobronchial low-grade MALT lymphoma causing unilateral hypertranslucency. Monaldi Arch Chest Dis 61(4): 237-240.
-
Hashemi SM, Heitbrink MA, Jiwa M, Boersma WG (2007) A patient with endobronchial BALT lymphoma successfully treated with radiotherapy. Respiratory medicine 101(10): 2227-2229.
-
Liao TY, Lin CC, Yuan CT, Lin CK, Ho CC (2020) Mucosa- associated lymphoid tissue lymphoma with isolated endobronchial involvement. Respirol Case Rep 8(8): e00672.
-
Hardavella G, Thalassinos N, Anastasiou N (2009) Primary endobronchial non-Hodgkin lymphoma in an 80-year-old patient with prostate cancer. Interact Cardiovas Thorac Surg 9(4): 739-740.
-
Sahin F, Fener N, Yildiz P (2012) Endobronchial metastases of fibrosarcoma and non-Hodgkin’s lymphoma. Arch Iran Med 15(8): 520-522.
-
Thomas N, Royce R, Garlapati V, Platsky V, Tang H, et al. (2016) Diffuse Large B-Cell Lymphoma Presenting as an Endobronchial Mass: A Case Report and Review of Literature. Journal of Hematology 5(3): 106-109.
-
Solomonov A, Zuckerman T, Goralnik L, Ben Arieh Y, Rowe JM, et al. (2008) Non-Hodgkin’s lymphoma presenting as an endobronchial tumor: report of eight cases and literature review. Am J Hematol 83(5): 416-419.
-
Zamboni M, Sousa AMCd, Lannes DC, Gonçalves CMC, Cunha ET, et al. (2004) Linfoma não-Hodgkin endobrônquico. Jornal Brasileiro de Pneumologia 30(1): 53-55.
-
Sousa A, Lannes D, Gonçalves C, Cunha E, Cordeiro S, et al. (2004) Endobronchial involvement in non-Hodgkin’s lymphoma. Jornal Brasileiro de Pneumologia 30(1): 53- 55.
-
J Han KL, Roh M, Kim W (2011) Non-Hodgkin’s Lymphoma Presenting as an Endobronchial Polypoid Mass: A Case Report J Korean Soc Radiol 64(2): 147-150.
-
Meka M, Mirtcheva RT, Fishman D, Ghesani M (2009) Type two or localized endobronchial non-Hodgkin lymphoma. Clin Nucl Med 34(10): 656-658.
-
Argüder E, Hasanoğlu HC, Karalezli A, Aknc S, Dilek I (2012) Endobronchial involvement in non-Hodgkin lymphoma. Journal of Bronchology & Interventional Pulmonology 19(2): 142-144.
-
Kim DH, Ko YH, Lee MH, Ree HJ (1998) Anaplastic large cell lymphoma presenting as an endobronchial polypoid mass. Respiration 65(2): 156-158.
-
Kanthan R, Senger JL, Miller G (2014) Isolated pediatric endobronchial primary anaplastic large cell lymphoma. Journal of Pediatric Surgery Case Reports 2(2): 66-69.
-
Zhang Y, Wang L, Huang J, Qian J, Jin J (2012) Anaplastic large cell lymphoma presenting as an endobronchial polypoid mass. Leuk Lymphoma 53(10): 2078-2079.
-
Richert Boe KE, Bagby GC (1988) Burkitt’s lymphoma presenting as an endobronchial lesion. Am J Med 85(6): 864-866.
-
Figgis P, Rainer S, Ma D, Glanville A (2003) Endobronchial mantle cell lymphoma. Intern Med J 33(5-6): 261-262.
-
Miyoshi I, Togitani K, Kuwayama Y, Daibata M, Matsumoto M, et al. (2007) Bilateral endobronchial involvement in mantle cell lymphoma. Internal medicine (Tokyo, Japan) 46(7): 429-30.
-
Katono K, Shirasawa M, Harada S, Niwa H, Nakahara Y, et al. (2016) Endobronchial involvement of mantle cell lymphoma: A case report. Respir Med Case Rep 19: 77- 79.
-
Ferrer G, Gutierrez G, Schwartz AM, Delaney MD (2010) Peripheral T-cell lymphoma with endobronchial involvement. J Bronchology Interv Pulmonol 17(2): 169- 170.
-
Matsumoto S, Fujimoto N, Fuchimoto Y, Asano M, Yano T, et al. (2015) Endobronchial T-cell lymphoma in a patient with chronic pyothorax. Respirol Case Rep 3(2): 44-47.
-
Terzi A, Furlan G, Zannoni M, Adovasio A, Gorla A (1996) Endobronchial extramedullary plasmacytoma. Report of one case. Lung Cancer 16(1): 95-100.
-
Fernández Bussy S, Labarca G, Folch E, Majid A (2013) Extramedullary endobronchial plasmacytoma. BMJ case reports 2013: bcr2012007354.
-
Brackett LE, Myers JR, Sherman CB (1994) Laser treatment of endobronchial extramedullary plasmacytoma. Chest 106(4): 1276-1277.
-
LeNoir B, Bruner ET, Denlinger CE, Gibney BC (2019) Extramedullary Plasmacytoma of the Right Main Bronchus. Ann Thorac Surg 108(2): 119-120.
-
Newton RC, Kemp SV, Yang GZ, Darzi A, Sheppard MN, et al. (2011) Tracheobronchial amyloidosis and confocal endomicroscopy. Respiration 82(2): 209-211.
-
Tanrıverdi E, Özgül MA, Uzun O, Gül Ş, Çörtük M, et al. (2016) Tracheobronchial Amyloidosis Mimicking Tracheal Tumor. Case reports in medicine 2016: 1084063.
-
Kang HW, Oh HJ, Park HY, Park CK, Shin HJ, et al. (2016) Endobronchial amyloidosis mimicking bronchial asthma: a case report and review of the literature. Open medicine (Warsaw, Poland) 11(1): 174-177.
-
Lal A, Akhtar J, Khan MS, Chen Y, Yaron G (2018) Primary endobronchial amyloidosis: A rare case of endobronchial tumor. Respir Med Case Rep 23: 163-166.
-
Gibbaoui H, Abouchacra S, Yaman M (2004) A case of primary diffuse tracheobronchial amyloidosis. Ann Thorac Surg 77(5): 1832-1834.
-
Fiorelli A, Accardo M, Galluccio G, Santini M (2013) Tracheobronchial amyloidosis treated by endobronchial laser resection and self expanding Y stent. Arch Bronconeumol 49(7): 303-305.
-
Kiani B, Magro CM, Ross P (2003) Endobronchial presentation of Hodgkin lymphoma: a review of the literature. The Annals of Thoracic Surgery 76(3): 967- 972.
-
Zompi S, Couderc LJ, Cadranel J, Antoine M, Epardeau B, et al. (2004) Clonality analysis of alveolar B lymphocytes contributes to the diagnostic strategy in clinical suspicion of pulmonary lymphoma. Blood 103(8): 3208-3215.
-
Lin CY, Chung FT (2016) Central airway tumors: interventional bronchoscopy in diagnosis and management. J Thorac Dis 8(10): 1168-1176.
-
(2003) Rigid Bronchoscopy. Chest 123(5): 1695-1696.
-
Kim H (2017) Bronchoscopic Management of Central Airway Obstruction. Journal of Thoracic Oncology 12(11): 1626-1627.
-
Rosell A, Stratakos G (2020) Therapeutic bronchoscopy for central airway diseases. Eur Respir Rev 29(158): 190178.
-
Pierce RJ, Mestitz H, Simpson LW, Daniel FJ (1990) Endobronchial resection with the Nd-YAG laser--two years experience in an Australian unit. Aust N Z J Med 20(2): 120-126.
-
Khemasuwan D, Mehta AC, Wang KP (2015) Past, present, and future of endobronchial laser photoresection. J Thorac Dis 7(4): 380-388.
-
Dutau H, Breen D (2010) Endobronchial laser treatment: An essential tool in therapeutic bronchoscopy. European Respiratory Monograph 48: 149-160.
-
Bolliger CT, Sutedja TG, Strausz J, Freitag L (2006) Therapeutic bronchoscopy with immediate effect: laser, electrocautery, argon plasma coagulation and stents. Eur Respir J 27(6): 1258-1271.
-
El Badrawy MK, Shalabi NM, Hewidy AA, Fouda AM (2015) Sequential use of cryoextraction postelectrocautery for airway recanalization using fiberoptic bronchoscopy. Egyptian Journal of Bronchology 9(3): 269-275.
-
Pajares V, Torrego A, Granell M, Szafranska J, Mozos A, et al. (2013) Recurrent endobronchial diffuse large B-cell lymphoma. Diagnosed by cryoprobe. Arch Bronconeumol 49(5): 210-212.
-
Moghissi K, Dixon K, Stringer M, Freeman T, Thorpe A, et al. (1999) The place of bronchoscopic photodynamic therapy in advanced unresectable lung cancer: experience of 100 cases. Eur J Cardiothorac Surg 15(1): 1-6.
-
Kiani B, Magro CM, Porcu P, Starns M, Heerema N, et al. (2003) Polypoid endobronchial Hodgkin lymphoma with an initial response to photodynamic therapy. Ann Thorac Surg 76(3): 940-942.
-
Wilhelm K, Schild H, Düber C, Mitze M, Schlegel J, et al. (1996) Stent implantation as a palliative therapeutic measure in stenosing tumors of central airways. RoFo 164(6): 496-501.
-
Semaan R, Yarmus L (2015) Rigid bronchoscopy and silicone stents in the management of central airway obstruction. J Thorac Dis 7(4): 352-362.
-
Schmidt B, Massenkeil G, John M, Arnold R, Witt C (1999) Temporary tracheobronchial stenting in malignant lymphoma. Ann Thorac Surg 67(5): 1448-1450.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies