Incidence of Adverse Transfusion Reaction and Practices for its Prevention
Transfusion reactions are the untoward event towards blood products. Although majority of transfusion reactions are uneventful sometimes it may have life threatening events. This study was conducted to estimate the incidence and determine the nature of blood transfusion reactions in our hospital. It also aims to find practices which could prevention such reactions. All the Adverse transfusion reactions were investigated in detail in the blood bank for the clerical errors, immunohematology workup and classified according to their nature. A total of 38308 units of components were issued to various departments in the hospital. Total 61 transfusion reactions were reported to the blood bank following transfusion of components only (0.16%). The most common type of transfusion reaction among all the ATRs was febrile nonhemolytic transfusion reaction (44%), followed by allergic (39%). Fever and chills, rigors were the most common symptom. Other reactions were dyspnoea, rashes and tachycardia. Avoiding unnecessary transfusion, red cell modification like leukofitration for FNHTR, red cell washing for allergic reactions and anaphylactoid reactions and implementing Patient Blood Management are tools to decrease transfusion reactions.
Introduction
Blood has no substitutes. Every year millions of blood components are transfused across the globe. Blood components transfusions are lifesaving and relatively safe procedure. However it is not entirely free of risks and hazards. The potential adverse transfusion reactions associated with any blood transfusion may range from mild to life threatening. Knowledge of these ATRs helps not only in their easy identification and management but also it alerts us to prevent its occurrence by taking precautionary and adequate measures. Haemovigilance is defined as “a set of surveillance procedures covering the whole transfusion chain (from the collection of blood and its components to the follow-up of recipients), intended to collect and assess information on unexpected or undesirable effects resulting from the therapeutic use of labile blood products, and to prevent their occurrence or recurrence” [1]. Haemovigilance was first launched in France in 1994 and followed by other countries [2]. Haemovigilance program of India (HvPI) was launched in 2012. The lack of proper and strict Haemovigilance systems throughout the country makes it difficult to assess the true and actual incidence of these reactions. The purpose of this study was to estimate the incidence and pattern of transfusion-related adverse events in our centre. We also analysed the measures and practices which can prevent transfusion-related adverse events.
Methodology
The study was conducted in the Department of Transfusion Medicine at JIPMER, Pondicherry, a tertiary healthcare centre in Southern India. Data was collected retrospectively from departmental transfusion reaction records. Review period was from May 2020–April 2021. Records of all the events related to adverse events were tabulated and analyzed. All transfusion reactions during this period were included in this study. As per hospital policy, 100% components were prepared and no whole blood was issued to patients at our centre. Clerical check was performed by blood bank technologist before transfusing the blood component. Patients were monitored at ward from the start of each transfusion till the end. If there is any event of a transfusion reaction, a filled up transfusion reaction reporting form was sent to the blood bank along with left over blood product bag & post-transfusion patient blood and urine samples. The reaction forms includes patient details, component details, amount of blood volume transfused, time of start of the blood transfusion, and time when the transfusion was stopped due to an adverse event. Details of clinical signs and symptoms (i.e., fever, chills, hypotension, rigors, cola ¬colour urine, rashes, respiratory discomfort, and any other untoward events developed during transfusion or the following transfusion) are thoroughly recorded. Patient’s vital signs, volume of urine passed and any history of previous transfusion given to the patient was obtained. Further workup for confirmation of transfusion reaction was carried out in the Transfusion Medicine Department. Patient’s blood sample and blood component(s) were checked for clerical errors. Any abnormal mass or clot if present in the blood bag was also checked. Repeat ABO blood grouping & Rh typing, repeat cross matching, screening for irregular antibodies was done and was compared with the pretransfusion sample. In case of a suspected hemolytic transfusion reaction—DAT (Direct Antiglobulin Test), Qualitative and Quantitative estimation of plasma Haemoglobin %, Serum Bilirubin and Peripheral blood smear examination for the presence of schistocytes and spherocytes. Colour of the urine is noted. In case of red urine, it is centrifuged to distinguish between hematuria and hemoglobinuria. Blood sample from the residual blood bag were sent for sterility testing to the microbiology laboratory. Investigations for renal function tests, liver function tests, and complete blood count are sent to the respective laboratory by the clinician in charge. Once transfusion reaction workup is completed, categorization of transfusion reaction was done on basis of reported signs and symptoms, workup results and investigation reports as defined in American Association of Blood Bank (AABB) Technical manual [3] and the data were submitted to the Haemovigilance Programme of India (HvPI) after imputability assessment since 2017. All the collected data were entered into a Microsoft Excel spreadsheet and necessary statistical analysis was done.
Results
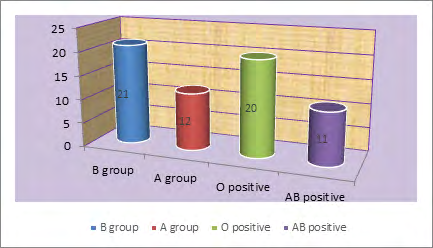
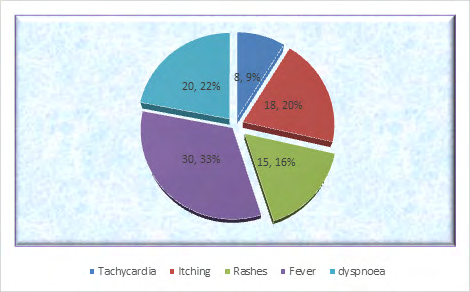
Total of 38304 blood components was issued to various wards during the study period. These comprised packed red blood cells 14221(37.12%), fresh frozen plasma (FFP) 10328(26.96%) and Random Donor platelets (RDP) 12143(31.71%) (Table1). Frequency of ATR during study period was 0.16 %. Out of 61 reactions reported 27(44%) were Females and 35 (56%) were seen in males. Mean age was 37year (range 5 to 79 years). Average transfusion reaction rate with PRBC was 0.32%, RDPs had reaction rate of 0.04%. In contrast, average reaction rate with fresh frozen plasma (FFP) was 0.06%. FNHTR were the most commonly encountered ATR (Table 2). Fever (33%) and chills & rigors (23%) were the most common symptom noticed in ATR followed by dyspnoea (16%), rashes (11%) and tachycardia (9.6%). Maximum number of ATRs were seen in blood Group B followed by O, A and AB (Figures 1 & 2).
| PRBC | FFP | RDP | SDP | CRYO | Total units |
|---|---|---|---|---|---|
| 14221 (37.12%) | 10328 (26.96%) | 12143 (31.71%) | 605 (1.58%) | 1007 (2.63%) | 38304 (100%) |
| 46 (0.32%) | 7 (0.06%) | 5 (0.04%) | 1 (0.16%) | 2 (0.19%) | 61 (TR-0.16%) |
Table 1: Components Issued & Transfusion Reactions.
| PRBC | RDP | FFP | SDP | CRYO | TOTAL | |
|---|---|---|---|---|---|---|
| FNHTR | 25 | 2 | - | - | - | 27 (44.3%) |
| TACO | 2 | - | 2 (3.3%) | |||
| TRALI | 1 | 1 (1.6%) | ||||
| Allergic | 12 | 4 | 5 | 1 | 2 | 24 (39.4%) |
| HTR | - | 0 | ||||
| Sepsis | 0 | |||||
| Non-specific | 7 | 7 (11.4%) | ||||
| TOTAL | 46 (75.4%) | 7 (11.5%) | 5 (8.2%) | 1 (1.6%) | 2 (3.3%) | 61 (100%) |
Table 2: Type of ATRs with respect to component transfusion.
Discussion
Transfusion reaction management and prevention are essential aspects of blood safety. The Haemovigilance network in France reported a rate of 0.25 incidents/100 blood components between 1994 and 1998 [2]. According to 2001 report of a Haemovigilance system of the Canadian province of Quebec, the incidence of ATR was 0.35% for labile blood components [4]. Incidence of ATR in our Centre was 0.16%. In a similar study done by Bhattacharya, et al. [5] the prevalence of transfusion reactions was found to be 0.18%, Chakravarty-Vartak U et al., reported 0.16% ATR out of 30,470 units issued over the period of two years [6].
In the present study FNHTR (44.3%) is the most common ATR followed by Allergic (39.4%), TACO (3.3%), and TRALI (1.6%). Pahuja, et al. [7], Mukherjee, et al. [8] in their study showed FNHTR were most common TR followed by allergic. Ramanathan, et al. study shows FNHTR (53%) as a most common ATR followed by allergic TR (39%), Anaphylactic reaction (3%), TACO 2%, TRALI 1% and non-immune haemolytic transfusion reactions (1%) [9]. Most common reaction noted in Chakravarty-vartak U, et al. was febrile reaction followed by allergic reaction [6] Bhattacharya, et al. shows similar results [5]. In contrast, Chavan SK, et al. reported that allergic (55.6%) is common than FNHTR (33.3%) [10]. Kumar P, et al. also reported allergic reaction (55.1%) as commonest followed by FNHTR (35.7% [11]. Low rates of reaction in our study can be attributed to use of leukoreduction by buffycoat method of component preparation. As universal leukodepletion is not economically feasible in a resource limited setting, buffy coat removal can be an alternative.
The overall incidence of allergic reactions in studies varies from 0.2% to 3% [12]. In the present study, 0.32% with red cells, 0.04% with platelets, and 0.06% with FFP (Table 1). Tanz, et al. in their study on leukodepleted component found the rate to be as low as 0.06% [13]. Single case of TRALI was seen in the study giving incidence of 0.005%. TRALI
reported in various studies in western literature ranged from 0.001% to 0.008% [14]. TRALI sometimes under diagnosed as it mimics clinical conditions which cause acute lung injury and due to lack of investigations to meet criteria of TRALI in resource limited setups. TACO was seen in 2 cases in our study giving an incidence of 0.008%.The incidence per unit was higher after red cell transfusion as most cases transfusion was done for severe anemia and cases were at extreme of age. Careful monitoring of patient fluid balance helps in diagnosing and management of TRALI.
Acute hemolytic reaction due ABO mismatch, cross match incompatibility, or any irregular antibodies was not reported during the study period. A case of pseudo hemolytic reaction to transfusion of frozen RBC present as HTR. Causes of pseudo hemolytic reactions are excess freezing or heating of red cell, exceeding storage time, temperature, chemically adding incompatible solutions/drugs, applying external excessive pressure on blood bag during transfusion. Single case of bacterial contamination was not encountered in our Maintains of quality control in collection and component separation could be the reason. Similar to our study Kumar et al in their study found males to be more affected than female [11]. A 75.4% of TR occurred with PRBC transfusion, 11.5% with platelet concentrate, 5 (8.2%) with FFP transfusions. Ramanathan et all study shows 80% of TR occurred with PRBC transfusion, 11.80% with FFP, 6.40% with PC and 1.80% with PRP transfusions [9]. Chavan SK, et al. reported 57.77% TR with WB and 42.22% with PRBC in their study. No TR was reported with PRP and FFP transfusions [10].
Most of the transfusion reactions were noted within 15 min of starting blood transfusion. Mean volume of blood transfused was 75 ml. The attending staff should be more vigilant during this period, and temperature and pulse should be noted after 15 min of starting of transfusion for each unit. In present study, we noticed fever, chills and rigor tachycardia, were the most common signs reported in ATR similar to findings of Ramanathan & Chakravarty-Vartak U, et al. Highest rate of transfusion reaction was in blood group B followed by O but no association was found (P > 0.05).
Conclusion
Adverse Transfusion reaction can be decreased with practices of recipient Haemovigilance. This includes appropriate donor selection, use of leukoreduction filters for required cases, use of buffy coat removal method for component preparation, strict bed side patient monitoring etc. Implementation of programme for rational use of blood and creating awareness regarding blood components with appropriate transfusion reaction reporting helps in using blood components safely.
References
-
Mafirakureva N, Khoza S, Mvere D, Chitiyo ME, Postma MJ, et al. (2014) Incidence and pattern of 12 years of reported transfusion adverse events in Zimbabwe: a retrospective analysis. Blood Transfus 12(3): 362-367.
-
Andreu G, Morel P, Forestier F, Debeir J, Rebibo D, et al. (2002) Hemovigilance network in France: Organization and analysis of immediate transfusion incident reports from 1994 to 1998. Transfusion 42(10): 1356-1364.
-
Saran RK (2003) Adverse effects of blood transfusion. Transfusion Medicine Technical Manual. 2nd (Edn.), New Delhi: Directorate General of Health Services pp: 127- 129.
-
Robillard P, Karl Itaj N (2002) Incidence of adverse transfusion reactions in the Quebec Hemovigilance System. Vox Sang 83: 120.
-
Bhattacharya P, Marwaha N, Dhawan HK, Roy P, Sharma RR (2011) Transfusion related adverse events at the tertiary care center in North India: An institutional hemovigilance effort. Asian J Transfus Sci 5(2): 164-170.
-
Chakravarty Vartak U, Shewale R, Vartak S, Faizal F, Majethia N (2016) Adverse reactions of blood transfusion: A study in a tertiary care hospital. Int J Sci Study 4(2): 90-94.
-
Pahuja S, Puri V, Mahajan G, Gupta P, Jain M (2017) Reporting adverse transfusion reactions: A retrospective study from tertiary care hospital from New Delhi, India. Asian J Transfus Sci 11(1): 6-12.
-
Mukherjee S, Sahoo D, Ramnath A, Maiti R (2018) A pilot study analysis of transfusion‑related adverse events at the tertiary care hospital in Eastern India: Encourages the establishment of institutional hemovigilance program. Glob J Transfus Med 3(1): 76-77.
-
Ramanathan, Meena, Sushama (2019) Reporting Adverse Transfusion Reactions Section in a Teritary Care Centre, Kerala, India. National Journal of Laboratory Medicine 8(3): 8-10.
-
Chavan SK, Patil G, Rajopadhye P (2016) Adverse blood transfusion reactions at tertiary care hospital. Int J Res Med Sci 4(6): 2402-2407.
-
Kumar P, Thapliyal R, Coshic P, Chatterjee K (2013) Retrospective evaluation of adverse transfusion reactions following blood product transfusion from a tertiary care hospital: A preliminary step towards hemovigilance. Asian J Transfus Sci 7(2): 109-115.
-
Stainsby D, Jones H, Asher D, Atterbury C, Boncinelli A, et al. (2006) Serious hazards of transfusion: A decade of hemovigilance in the UK. Transfus Med Rev 20(4): 273- 282.
-
Tanz WS, King KE, Ness PM (2001) Reevaluation of transfusion reaction rates associated with leukocytereduced red blood cells. Transfusion 41: 7.
-
Webert KE, Blajchman MA (2003) Transfusion related acute lung injury. Transfus Med Rev 17(4): 252-262.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies