Low Dose Factor VIII Prophylaxis in Hemophilia: Indian Perspective
Important complications of hemophilia are bleeding and joint deformity. Episodic treatment of hemophilia with Factor VIII arrests bleeding but not joint deformity. Thus there is a need to administer Factor VIII prophylactically to prevent bleeding and joint deformity. Apart from high dose prophylaxis practised in developing countries, low dose prophylaxis with 10-15 IU/ kg body weight twice/thrice a week is found to be quite effective in resource limited tropical country like India. Significant reduction in musculo-skeletal, visceral bleeding and joint deformity has been observed from various centres in India. Country wide awareness, including at district level, has happened now in India. Factor VIII is more freely supplied by Govt. agencies now.
Introduction
The two agonizing problems with severe hemophilia are episodic bleeding and arthropathy. Pioneer prophylaxis regimens were developed in Sweden in the 1960s. One of the pioneers in factor prophylaxis was Swedish scientist, Inga Marie Nilsson [1]. It is no longer now debatable that state- of-art-therapy for hemophilia is prophylaxis. Over the years various dosage schedules were evolved: [2].
- High dose regimens (Nilsson IM, 1958, Sweden) 25- 40U/kg 3 times a week / alternate day
- Intermediate dose (Van Creveld S.,1968, Netherlands) 15-25U/kg 2-3 times a week
- Low dose (developing countries) 10-20U twice a week
- Very low dose: 10 units/kg twice a week High/intermediate-dose prophylaxis protocols are not feasible in Indian setting because of the huge cost involved. Low dose protocols are more suitable in developing countries [2]. A landmark study from Italy, Esprit Study published in 2011 showed FVIII prophylaxisis significantly reduces arthropathy [3]. The Current WHO Recommendation states, the first choice of treatment of hemophilia is prophylactic therapy.
Factor VIII Prophylaxis In India
Definition for Severity of Hemophilia
Severe hemophilia - <1% FVIII level (spontaneous bleed), Moderate – 1-5% (spontaneous bleed unlikely), Mild - >5%
The Rationale of Prophylactic Therapy
Aim: To convert severe hemophilia i.e. <1% FVIII level to moderate one i.e. >1% FVIII level. It can be achieved by adding FVIII as low as 1U/kg/day (7-10 U/kg/week). Thus thrice a week dosage (adequate to maintain FVIII trough throughout) is practised.
Whom to give prophylaxis (WFH: guidelines for the
management of hemophilia, June 2018)
Primary prophylaxis: Before joint damage starts i.e. soon after first bleed in a child.
Secondary prophylaxis: Ideal age – Before 3 years of life (may be extended to 5 years).
Intermediate Prophylaxis: To children before examinations, contact sports competitions.
Government Institutions Where Such Facilities are Available are As Below
- R & R Army Hospital, New Delhi - Reduced bleed from 15 to one in a year (personal communication from Brig. Ajay Sharma).
- ESI hospital, Kolkata, West Bengal – Practices giving injections on fixed days (3 times a week) in the hemophilia clinic.
- Factor VIII more freely supplied by Govt. agencies in West Bengal at district level now.
- Jawaharlal Institute of Postgraduate Medical Education & Research (JIPMER), Puducherry.
- King George Medical University of Health Sciences (KGMUHS), Lucknow - Factor VIII more freely supplied by Govt. agencies now in Uttar Pradesh, even at district level.
- SMS Medical College, Jaipur, Rajasthan.
Result: After 11 Months of Observation
Private institutions
- Christian Medical College, Vellore
- Sahyadri Hospital, Pune
- Amrita Institute of Medical Sciences (AIMS), Kerala
Pondicherry
In 2012, 26 patients were studied for factor prophylaxis at JIPMER, Pondicherry, and author’s parent institute [4] (Figure 1).
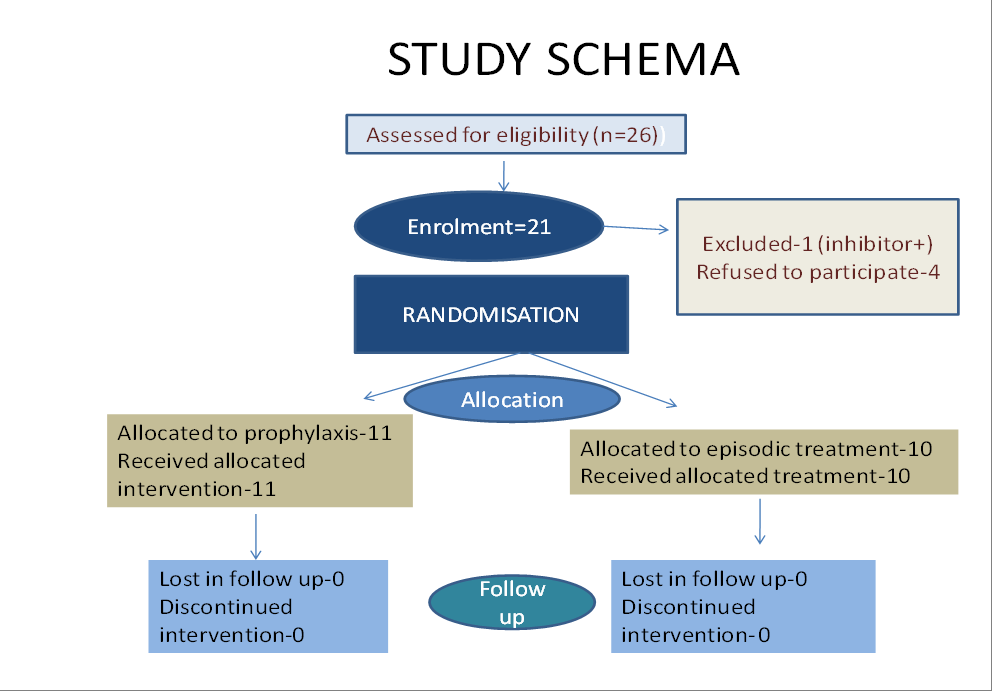
| PROPHYLAXIS GROUP (N=11) | EPISODIC TREATMENT GROUP (N=10) | STATISTICAL SIGNIFICANCE (p VALUE) | |
|---|---|---|---|
| Overall bleeds patient / month Mean ± SD | 0.185 ±0.183 | 0.787 ±0.457 | <0.05 |
| Joint bleeds/ patient/ month Mean ± SD | 0.08 ±0.13 | 0.48 ±0.34 | <0.05 |
| Pettersson score (baseline) Median (range) | 0 (0-2) | 0.5 (0-2) | Not significant |
| Pettersson score (end of study) Median (range) | 0 (0-2) | 1.0 (0-2) | Not significant |
| Number of emergency visits to hospital Median (min-max) | 1 (0-7) | 9 (1-15) | <0.05 |
| School absenteeism (days) Median (min-max) | 3 (0-30) | 25 (2-70) | <0.05 |
| Total factor usageMean ±SD | 14992.7±4057.3 | 11750 ± 7583.6 | Not significant |
| Factor VIII usage/ kg/month | 87.51 ± 12.86 | 56.32 ±49.74 | Not significant |
Table 1: Result: After 11 months of observation. No FVIII inhibitor noted in the study (Verma et.al A randomized study of very lo
Conclusion: Conclusion of this study was that low dose factor prophylaxis is significantly effective in reducing number of joint bleeds. Children can be initiated with a twice weekly prophylaxis regimen. Risk of inhibitor growth is not directly associated to low dose factor prophylaxis. This form of treatment significantly reduces days of school absenteeism and emergency hospital visits. Considering overall benefits, low dose prophylaxis seems to be cost effective. However the intriguing fact is only three in prophylactic group had factor trough >1% even though improvement was experienced in all the patients. This probably suggests that spontaneous bleed starts at a level of <1%, which could not be measured with available conventional equipments.
Christian Medical College (CMC) Hospital, Vellore
In a study at CMC, 26 patients with severe hemophilia A (FVIII <1%) were enrolled. Patients were administered 10-15 IU/kg two times/week for 8 months. The annualized bleeding rate (AdBR) was:
- before prophylaxis - 3 (1-5)
- after prophylaxis 0 (range: 0-3) No patient had any target joint involvement. At end of the study, it was concluded that with low “doses of ~15 IU/kg 2 times/week, the” AdBR can be brought down significantly [5].
Amrita Institute of Medical Sciences (AIMS), Kerala
There was an extensive work done on hemophilia in Kerala. In a particular research study, most children had been started on minimum-dose prophylactic treatment (PT) with plasma derivative CFC (Clotting component concentrate). Factor VIII concentrate was” provided at a dose of 20-40 IU/kg with two split doses in “a week for haemophilia A. The mean age at clinical audit entry was 7.64 (SD±2.46) years. The mean consumption of CFCs was 7.69 (SD± 6.29) IU/kg/week for ODT and 33.99 (SD± 26.41)/kg/week for PT. Overall bleed and joint bleed was significantly less in prophylactic group. Table 2 below displays significantly low bleeding rate in prophylactic therapy group as compared to that in episodic therapy group. Currently factor prophylaxis is being practiced even in district headquarters in Kerala, West Bengal and other states of India [6].
| Study | Bleeding Rate | Duration & type of bleed | P value | |
|---|---|---|---|---|
| Episodic (ET) | Prophylactic (PT) | |||
| Goudier, et al. Tunisia | 7 (0-50) median & range | 0.5 (0-120) median & range | Bleed rate per year | |
| Wu, et al. China | 9.9 (mean) | 1.7 (mean) | Joint bleed for 12 weeks | |
| Tang, et al. China | 2.4 ± 1.9 (mean±SD) | 0.5±0.8 (mean±SD) | Joint bleed /month | <0.01 |
| Verma, et al. India [4] | 0.787±0.46 (mean±SD) | 0.185±0.18 (mean±SD) | Overall bleeds/patient/month | <0.05 |
| Sidharthan, et al. India [6] | 11.27±6.29 (mean±SD) | 0.91±1.64 (mean±SD) | Overall bleeds for 6 months | 0.005 |
Table 2: Change in bleed rate – episodic versus prophylaxis therapy.
ESI Hospital, Sealdah, Kolkata
(Personal Communication: Told by Dr Santanu Basu, Consultant Haematologist, Kolkata) In India, Factor VIII prophylaxis was first introduced in ESI hospital, Kolkata in 2010. It is interesting to note that schedule was introduced initially for just convenience, so that episodic treatment could be avoided and haphazard treatment could be streamlined.
| 106 | |
|---|---|
| VIII deficiency | 84 |
| IX deficiency | 22 |
| Number on prophylaxis | 104 |
| Number of Patients with inhibitors | 6 |
| Age group on prophylaxis: | 2-53 years, median ~ 20 years |
| Home therapy Outcome after prophylaxis: | Yes |
| Annual Bleeding episodes - | |
| Before prophylaxis | 10-50, median 30 |
| After prophylaxis | 0-16, median 2.1 |
| ABR : Annual Bleeding rate | 93.6% reduction |
| School/ work absenteeism | Nil |
Table 3: Experience at ESI Hospital, Kolkata.
SMS Medical College, Jaipur, Rajasthan
This hospital based observational prospective, analytic study was conducted at SMS Medical College, Jaipur, and Rajasthan during April 2016 to November 2017. During the propylaxis, factor was given in dose of 10 IU/kg/body weight twice a week. Seventy adult patients including 58 hemophilia A patients were included in the study. During observation period, 129 and 74 episodes of bleed occurred in moderate and severe hemophilics respectively. In prophylaxis period, only 40 and 26 episodes of bleed occurred in moderate and severe hemophics respectively. The episodes of bleeds were decreased by 68.99% and 64.86% in moderate and severe hemophilics respectively during prophylaxis period (p<0.05). The duration of absenteeism from work/school was reduced by 53.73% during prophylaxis period compared to observation period (279 vs 603) [7].
Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow
Of late, Govt of UP has made factor VIII available in several centres of Uttar Pradesh, which is being used for prophylaxis purpose. Short term prophylactic factor infusions were given to some patients who were undergoing physiotherapy and also to wheel chair bound patients with hemophilia. It was emphasised to government the need for proper availability of FVIII for prophylaxis purpose. Starting prophylaxis with lower dose causes significant reduction in bleed. Currently factor prophylaxis is being practiced even in district headquarters in Kerala, West Bengal and other states of India. India has the second highest number of patients with hemophilia in the world. As has been observed earlier, if not treated early, the repeated bleeding into joints, bones muscles may lead to synovitis, arthritis and permanent joint deformities. The bleeding itself can lead to wasting and atrophy of muscles [8].
Conclusion
Low dose factor VIII prophylaxis with a dose of 10-15 units twice/thrice a week is effective. Significant reduction in musculo-skeletal, visceral bleeding and joint deformity has been observed. A country-wide awareness, including at district level, has happened. Factor VIII is more freely supplied by Government agencies now. Further, preliminary observation from this review suggests that spontaneous bleed in hemophilia may be prevented even with FVIII level <1%.
References
-
Berntorp E (2013) History of prophylaxis: Commemorative Article. Haemophilia 19: 163-165.
-
Coppola A, Franchini M (2013) Target of prophylaxis in severe haemophilia: more than factor levels. Blood Transfus 11(3): 327-329.
-
Gringeri A, Lundin B, Von Mackensen S, Mantovani L, Mannucci PM, et al. (2011) A randomized clinical trial of prophylaxis in children with hemophilia A (the ESPRIT Study). J Thromb Haemost 9(4): 700-710.
-
Verma SP, Dutta TK, Mahadevan S, Nalini P, Basu D, et al. (2016) A randomized study of very low-dose factor VIII prophylaxis in severe haemophilia—a success story from a resource limited country. Haemophilia 22(3): 342-348.
-
Abraham A, Apte S, Singh AS, Subramaniam K, Korula A, et al. (2017) Meaningful reduction of annual bleeding rate with lower dose prophylaxis in minimally treated children with hemophilia in India . Blood 130(Supply 1).
-
Sidharthan N, Sudevan R, Narayana PV, Mathew S, Raj M, et al. (2017) Low‐dose prophylaxis for children with haemophilia in a resource‐limited setting in south India - A clinical audit report. Haemophilia 23(4): e382-e384.
-
Singh A, Mehta S, Goyal LK, Mehta S, Sharma BS (2019) Low dose prophylaxis vis-à-vis on-demand strategies for hemophilia: A cost-effective and disability attenuating approach. J Assoc Physicians India 67(11): 52-55.
-
Phadke S (2011) Hemophilia care in India: A review and experience from a tertiary care centre in Uttar Pradesh. Indian J Hematol Blood Transfus 27(3): 121-126.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies