Association of Methylene Tetrahydrofolate Reductase Gene A1298C (Rs1801131) Polymorphism with Myocardial Infarction among Sudanese Patients
Background: Myocardial infarction (MI) is among the leading causes of mortality worldwide. Variations in folate metabolism including genetic polymorphisms in the key metabolic enzymes had showed influences in the MI process. Objectives: To determine whether the C1298A transition in the Methylene Tetrahydrofolate Reductase (MTHFR) gene is associated with increased risk for MI among Sudanese patients. Material and methods: This is a hospital based case control study in which a total of 140 Sudanese subjects were enrolled, 70 patients with myocardial infarction and 70 age- and sex matched healthy volunteers as a control group. Genomic DNA was extracted by (QIA gene, Korea) kits and the SNPs genotypes were determined using polymerase chain reaction followed by restriction fragment length polymorphism (PCR- RFLP). Data of this study were collected using a structured interview questionnaire and analyzed by statistical package for social sciences (version 21). Results: The frequency of the AA genotype was higher in the patients group compared with control (96%, 71% respectively); while the AC genotype was higher in the control (20%, 5% respectively), while the CC genotype was not observed in this study population. The frequencies of A and C alleles were 0.68 and 0.02 respectively in MI patients while frequencies were 0.60 and 0.10 respectively in the control group. No statistically significant association was observed between MTHFR genotypes and MI (P. values = 0.4 and 0.1 for AA and AC genotypes respectively). Conclusion: In this study population, the A1298C MTHFR polymorphism is not associated with the risk of MI among the Sudanese population.
Introduction
Coronary artery disease (CAD) is a group of disorders involved thrombotic lesion in coronary artery; these includes acute coronary syndrome (ACS) of acute myocardial infarction (AMI) and unstable angina, chronic coronary syndrome of chronic stable angina. Diagnosis of such disorders is still a challenge despite the considerable progress in the diagnostic modalities [1]. Many risk factor are involved in the pathogenesis of coronary atherosclerosis, acting either in single way or in synergistic effect, these are -not limited to -smoking, obesity, diabetes mellitus, and hypercholesterolemia [2, 3].
Myocardial ischemia that results from a perfusion- dependent imbalance between supply and demand leads to myocytes necrosis which develops progressively depending on different factors (organ, species, cardiac work, duration of ischemia, collateral blood flow, etc) [4]. MTHFR is an important enzyme involved in folate metabolism; it catalyzes the conversion of 5, 10-methylenetetrahydrofolate (5, 10- MTHF) in 5-methyltetrahydrofolate (5-MeTHF), the latter representing the active form of folate that is involved in re-methylation of homocysteine to methionine. MTHFR gene was mapped on human chromosome 1p36.3; it has 11 exons and exhibits multiple polymorphisms in general population, some of them with altered function in homozygous individuals. However, two polymorphisms of the MTHFR gene are found with higher frequency: 677C>T and 1298A>C; these polymorphisms are thermolabile variants of the normal gene and determine the accumulation of homocysteine in circulatory system and the decrease of folic acid concentration. The second MTHFR polymorphism involves an adenosine to cytosine substitution at base pair 1298 (1298A>C), causing a glutamate to alanine substitution in the MTHFR protein. The polymorphism is located in exon 7, within the presumptive regulatory domain [5]. The 1298A>C mutation results in decreased MTHFR activity, with a stronger effect in the homozygous than in the heterozygous state, yet with a lesser impact than that of 677C>T [6]. Some previously published data show a frequency of 1298 CC genotype of 10% and an allele frequency of 1289C of
36% among distinct populations [7]. The 677C>T and 1298A>C mutations are found in regions encoding the N-terminal catalytic and the C-terminal regulatory domains of the protein, respectively [8]. The effects of the 1298A>C mutation on plasma concentrations of homocystin remain controversial; as some studies showed significant influence of this polymorphism on plasma homocystin level [9], while others have either not found any effect [10] or observed an association with even lower levels of plasma homocystin in homozygous individuals [11].
Methodology
This is a hospital-based case-control study conducted at Sudan Heart Center, Khartoum, Sudan. A total of 140 subjects were enrolled for this study; among them 70 patients had a confirmed diagnosis of MI (based on results of serum Tropnin test: >99th percentile URL, and echocardiography) and 70 age- and sex-matched apparently healthy volunteers- as a control group. Venous blood samples were collected from all participants in Ethylene diamine tetra acetic acid (EDTA). Genomic DNA was isolated using QIA gene kits (KOREA) and stored at -30°C until genotyping is carried out. MTHFR A1298C polymorphism was analyzed by Allele-Specific Polymerase Chain Reaction (AS-PCR) followed by restriction enzyme. For PCR amplification, A reaction mixture of 25μl was prepared for each sample, containing 5μl genomic DNA, 1μL of each of the forward (5’GCAAGTCCCCCAAGGAGG-3’), reverse (5’GGTCCCCACTTCCAGCAT-3’), [12] (MACROGEN, KOREA), 5μL master mix (MAXIME PCR PRE-MIX KIT (I-TAQ), INTRON, KOREA), and 18μL sterile distilled water. The amplification program consists of initial denaturation at 95ºC for 1 minutes; then 30 cycles [each consists of denaturation at 95ºC for 30 second, annealing at 61ºC for 30 second, and extension at 72ºC for 30 second], and a final extension at 72ºC for 7 minutes. PCR products were incubated over night with MboII restriction enzyme (Thermo SCIENTIFIC) then the product was separated on 3% agarose gel electrophoresis containing ethidium bromide with a 100 bp DNA ladder (SOLIS BIODYEN, ESTONIA) run with each batch of samples and the size of the fragments was determined under UV transilluminator (SYNGENE, JAPAN).
Patient’s data were collected using a structured interview questionnaire and analyzed by statistical package for social science (SPSS), version 21. The qualitative data were presented as frequency and percentage. Quantitative data were presented as Mean± SD. Association between qualitative variable was tested by Chi-square (X2) and Fisher’s exact tests. Multivariate logistic regression analysis was used for the prediction of MI risk as dependent variable with a set of predictors including MTHFR genotype and other MI risk factors. The allele frequencies and their accordance with Hardy Weinberg Equilibrium (HWE) were calculated using the conventional formulas. The study was approved by the scientific research committee, faculty of medical laboratory sciences, Karary University Khartoum, Sudan. Written informed consent was taken from each subject before participation.
Results
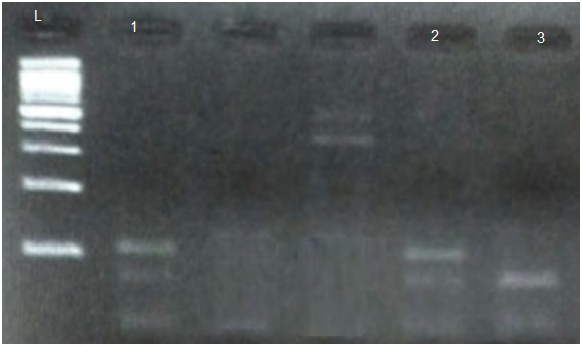
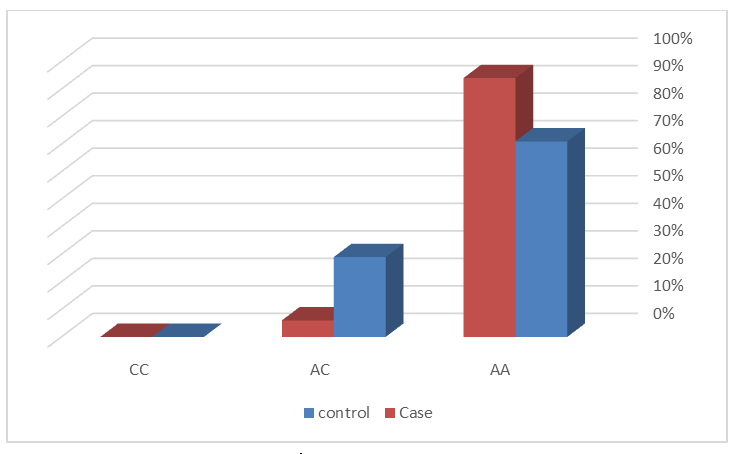
The mean age of participants in this study is 58.4 ± 12.4 years, ranging from 40 to 88 years. The results of PCR amplification yielded amplicons of length 143bp for A1298C polymorphism Figure 1. Post digestion results showed 77 and 28bp bands for AA genotype, 105, 77 and 28 bp for AC genotype as shown in Figure 2. The AA genotype frequency is 94% in the MI group and 71% in the controls, while AC genotype frequency is 6% in patients group and 29% in controls. There was no subject with CC genotype in both patients and control group Figure 3. The frequency of an allele was 0.68 in the patients with MI and 0.60 in the control group, while the frequency of T Allele was 0.02 in the patients with MI and 0.1 in the control group. All genotypes frequencies are in accordance with HDW equation (P values > .05).

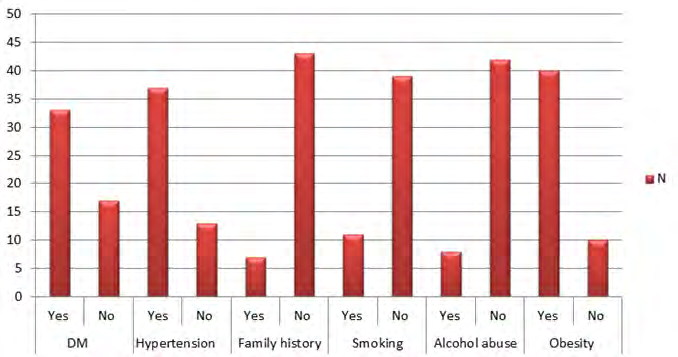
The results of the current study showed no statistically significant difference in genotype between patients and controls (P. values: AA= 0.7 and AC= 0.9). Moreover, there were no statistically significant difference in the age group and gender of patients with genotype (P. values = 0.5 and 0.2 respectively). All the patients had at least one known risk factor for MI these include, 50 (71%) DM, HTN and obesity, 18(25%) had smoker and 10(14%) were alcohol users (Figure 4). In addition the Multivariate regression analysis revealed no interaction between MI risk factors in case and control (Table 1).
Characteristic Patients Control p. value
N 70 70
Hypertensive non hypertensive 50:20:00 0.048611111 0.612
Alcohol abuse; non-alcohol abuse 0.458333333 0.048611111 0.447
Genotype AA 94% 71% 0.4
Age 58.4 ± 12.4 58.6 ± 12.6 0.5
Sex( male: female) 35:35:00 35:35:00 0.2
Diabetic; no diabetic 50:20:00 0.048611111 0.287
Obese; non obese 50:20:00 0.048611111 0.824
Smoker: nonsmoker 18:52 0.048611111 0.558
AC 6% 29% 0.1
Table1: Logistic regression showing interactions of MI risk factors.
Discussion
Myocardial infarction is the consequence of atherosclerotic plaque disposition on the coronary artery wall. Its manifestation depends on interactions between environmental and genetic risk factors; the present study was conducted to investigate the association between MTHFR gene polymorphism (A1298C) and the risk of MI among the Sudanese population. The results showed that, the frequency of AA, genotype in patients was higher than controls (94%, 71% respectively); the frequency of AC genotype is lower in patients compared with controls (5%, 20% respectively), while CC genotype was not observed in this study population. There was no statistically significant association between MTHFR gene polymorphism (A1298C) and MI. Previous studies in different populations showed inconsistent results regarding the association of this polymorphism with risk of MI. In north Indian for A1298C locus [13], the AA was more frequent in patients than control (43%, 33%) respectively and AC was more frequent in controls than patients (35%, 53%). Also Eftychiouet C, et al. [14] MTHFR AA, AC and CC genotypes frequencies in the MI group were not significantly different from the control group. In addition according to Eftychiou, et al. [15] the existence and extent of disease are not significantly associated with MTHFR A1298C polymorphisms. Also logistic regression analysis done by Nasiri, et al. [12] showed that; A1298C locus is not associated with increased susceptibility to MI.
On the other hand, there are fewer studies disagree with our finding which reported a significant association between CC genotype and risk of MI [13]. The result of the present study showed no statistically significant difference in the age group of patients with different A1298C polymorphic variants, this indicating that MTHFR gene polymorphism does not affect the age of incidence of MI. Similar results were reported by Tripathi, et al. [16] Hmimech, et al. [17] Glue, et al. [18] and Anderson, et al. [19]. All of them reported no association between age, and A1298C genotypes in patients with MI. In contrast, Butler, et al. [13] and Nishhama, et al. [20] suggested that the age of patients may be associated with MI occurrence. The current study showed no statistically significant association between gender and A1298C genotype. Some studies agree with this finding like [16, 17], while others disagree with this finding [20].
In the present study, there is no interaction between A1298C polymorphism and the conventional MI risk factors including (DM, HTN, and smoking, obesity and alcohol abuse) was reported. This finding was in agreement with a study by Anderson, et al. [19] who also reported no significant association between A1298C polymorphisms and any other risk factor among patients with acute coronary syndrome. Also Kerkeni M, et al. [13] found no statistically significant association of smoking with MI risk, in addition [17] no statistically significant association of diabetic, smoker, hypertension and obesity with MI risk. At the other hand, this finding disagrees with the finding of Gluec, et al. [18] who observed strong statistically significant association of smoking, diabetes and hypertension with MI.
Conclusion
The present study concludes that there is no statistically significant association between MTHFR A1298C polymorphism and risk of MI among the Sudanese patients.
Acknowledgements
Authors acknowledges Dr. Salah gumaa for valuable help and support in samples genotyping, also acknowledgements are extended to the Sudan heart center staff for their great effort during sample collection.
References
-
Lippi G, Montagnana M, Salvagno GL, Guidi GC (2006) Potential value for new diagnostic markers in the early recognition of acute coronary syndromes. CJEM 8(1): 27-31.
-
Trip MD, Cats VM, Capelle FJV, Vreeken J (1990) Platelet hyperreactivity and prognosis in survivors of myocardial infarction. New Engl J Med 322(22): 1549-1554.
-
Boos CJ, Lip GYH (2007) Assessment of mean platelet volume in coronary artery disease - what does it mean? Thromb Res 120(1): 11-13.
-
Alpert JS, Thygesen K, Antman E, Bassand JP (2000) Myocardial Infarction Redefined—A Consensus Document of The Joint European Society of Cardiology/ American College of Cardiology Committee for the Redefinition of Myocardial Infarction. J Am Coll Cardiol 36(3): 959-969.
-
Goyette P, Pai A, Milos R, Frosst P, Tran P, et al. (1998) Chen Gene structure of human and mouse methylenetetrahydrofolate reductase (MTHFR). Mammalian Genome 9(8): 652-656.
-
Van der Put NM, Gabreëls F, Stevens EM, Smeitink JA, Trijbels FJ, et al. (1998) A second common mutation in the methylenetetrahydrofolate reductase gene: an additional risk factor for neural tube defects? Am J Hum Genet 62(5): 1044-1051.
-
Vekemans BC, Coudé M, Muller F, Oury JF, Chabli A, et al. (2002) Methylenetetrahydrofolate reductase polymorphism in the etiology of Down syndrome. Pediatr Res 51(6): 766-767.
-
Weisberg IS, Jacques PF, Selhub J, Bostom AG, Chen Z, et al. (2001) The 1298ARC polymorphism in methylenetetrahydrofolate reductase (MTHFR): in vitro expression and association with homocysteine. Atherosclerosis 156(2): 409-415.
-
Kang SS, Wong PW, Susmano A, Sora J, Norusis M, et al. (1991) Thermolabile methylene tetrahydrofolate reductase: an inherited risk factor for coronary artery disease. Am J Hum Genet 48(3): 536-545.
-
Lievers KJ, Boers GH, Verhoef P, Heijer MD, Kluijtmans LA, et al. (2001) A second common variant in the methylenetetrahydrofolate reductase (MTHFR) gene and its relationship to MTHFR enzyme activity, homocysteine, and cardiovascular disease risk. J Mol Med 79(9): 522- 528.
-
Friedman G, Goldschmidt N, Friedlander Y, Yehuda AB, Selhub J, et al. (1999) A common mutation A1298C in human methylenetetrahydrofolate reductase gene: association with plasma total homocysteine and folate concentrations. J Nutr 129(9): 1656-1661.
-
Butler SJ, Akam L, Sinha N, Agarwal S, Mastana S, et al (2018) Association of methylenetetrahydrofolate reductase (MTHFR) C677T and A1298C polymorphisms with coronary artery disease (CAD) in a North Indian population. Cogent Medicine 5: 1478477.
-
Kerkeni M, Addad F, Chauffert M, Myara A, Gerhardt M, et al. (2006) Hyperhomocysteinemia, methylenetetrahydrofolate reductase polymorphism and risk of coronary artery disease. Ann Clin Biochem 43(Pt 3): 200-206.
-
Eftychiouet C, Antoniades L, Makri L, Koumas L, Costeas PA, et al. (2012) Homocysteine Levels and MTHFR Polymorphisms in Young Patients with Acute Myocardial Infarction: A Case Control Study. Hellenic J Cardiol 53(3): 189-194.
-
Nasiri M, Roostaei A, Ehsanian Z (2014) Association of Methylenetetrahydrofolate Reductase (MTHFR) Gene C677T and A1298C Polymorphisms with Myocardial Infarction from North of Fars Province. Res Mol Med 2(3): 36-40.
-
Tripathi R, Tewari S, Singh PK, Agarwal S (2010) Association of homocysteine and methylene tetrahydrofolate reductase (MTHFR C677T) gene polymorphism with coronary artery disease (CAD) in the population of North India. Genet Mol Biol 33(2): 224-228.
-
Hmimech W, IdrissiHH, DiakiteB, Baghdadi D, Korchi F, et al. (2016) Association of C677T MTHFR and G20210A FII prothrombin polymorphisms with susceptibility to myocardial infarction. Biomed Rep 5(3): 361-366.
-
Gulec S, Aras O, Akar E, Tutar E, Omürlü K, et al. (2001) Methylenetetrahydrofolate Reductase Gene Polymorphism and Risk of Premature Myocardial Infarction. Clin Cardio 24(4): 281-284.
-
Andresion MG, Botto N, Cocci F, Battaglia D, Antonioli E, et al. (2003) Methylenetetrahydrofolate reductase gene C677T polymorphism, homocysteine, vitamin B12, and DNA damage in coronary artery disease. Hum Genet 112(2): 171-177.
-
Nishihamaet K, Yamada Y, Matsuo H, Segawa T, Watanabe S, et al. (2007) Association of gene polymorphisms with myocardial infarction in individuals with or without conventional coronary risk factors. Int J Mol Med 19(1): 129-141.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies