Case Report of a 60-Year-Old Woman with Autoimmune Hemolytic Anaemia after Venetoclax
Background: Chronic Lymphocytic Leukaemia (CLL) is a common haematological malignant neoplasm that is characterized by proliferation of clonal B-cell lymphocytes and infiltration of blood, lymph nodes, spleen and bone marrow. Autoimmune Hemolytic Anaemia (AIHA) is a medical condition in which patient’s red blood cells are being destructed by immune system through antibodies leading to red blood cell lysis. Venetoclax is a novel BCL-2 selective inhibitor introduced amongst patients with CLL refractory to standard treatment lines. Common adverse events in Venetoclax treatment are: neutropenia, thrombocytopenia and diarrhea. Case Report: The following case study presents 60-year-old female patient that developed an autoimmune hemolytic anemia after introducing Venetoclax for CLL diagnosed nearly 13 years before and treated with many other treatment lines. AIHA was resolved after withdrawing Venetoclax and being treated with steroids, Rituximab and plasmapheresis. After that, Venetoclax was reintroduced with carefully monitored hemolysis markers as well as maintaining steroids and Rituximab treatment with good results. Conclusion: Although AIHA caused by Venetoclax is still not mentioned by producer’s summary of product characteristic (sPC), it is valuable for clinicians to have the knowledge that such adverse event may occur (diagnosed after eliminating other causes) and how it can be handled based on experiences of fellow clinicians.
Introduction
Chronic Lymphocytic Leukaemia (CLL) is the most common non-Hodkgin haematolgical malignant neoplasm amongst adults [1]. Its incidence is estimated at about 4.2 per 100 000 population in Western communities [2] and increases in population older than 80 to about 30 per 100 000 [3]. Incidence highly correlates with positive family history for CLL [4].
CLL defines as a monoclonal proliferation of B-cell line with its specific immunocytogenetic characteristics (cd23+, cd5+, cd19+, cd20+). Lymphocytes count in automatic blood smear a priori exceeds 5 G/L. Marrow is infiltrated with monoclonal B-cells in diverse patterns that no longer ha prognostic value [5]. CLL may trigger such medical conditions as cytopenias from neoplasm marrow infiltration, hypogammaglobulinaemia which results in severe infections and requires proper pharmacologic infection profilaxys [6]. For CLL characteristic is also incidence of: autoimmune haemolytic anemia’s (AIHA), immune thrombocytopenic purpura (ITP), Evans syndrome.
Autoimmune neutropenia (AIN), pure red cell aplasia (PRCA) and transformations into such other haematological neoplasms as Diffuse Large B-Cell Lymphoma (DLBCL) [Richter transformation], B-cell prolymphocyte leukaemia (B-PLL) and Hodgkin Lymphoma (HL) [7]. In CLL the risk for other neoplasms also rises; that involves skin cancer and melanoma risks, lung cancer risk and others [8].
Novel Treatment Lines are based on genetic assays in CLL [9]. The most important molecular status for treatment line choice is: hipo- /hypermethylated IgVH gene and Del (17p) or mutation in TP53 gene [10]. Creating treatment strategy requires also assessment of the patient’s fitness – which defines as lack of contradictions to receive full dose of treatment agent [11]. More general information about defining patients with CLL as fit and unfit for certain treatments routes is created by GCLLSG (German CLL Study Group) which recommends examining the patient’s renal function (as measuring eGFR) and undergoing CIRS examination (Cumulative Index Rating Scale) [12].
Amongst fit patients with hypermutated IgHV gene, without del (17p) or mutation in TP53 gene the first-line treatment is according to international CLL treatment guidelines [13] FCR (fludarabine, cyclophosphamide and rituximab) immunochemotherapy regimen in 6 cycles or BTK (Bruton kinase) inhibitor in monotherapy or with anti-CD20 antibody such as rituximab or obinutuzumab (also available in del (17p) and/or TP53 mutated cases) [13]. For unfit patients as a primary treatment or for relapsed cases of CLL possible are regimens of BR (bendamustine with rituximab) immunochemotherapy or a new therapy based on a novel agent of Venetoclax which is also a fine option of treatment for patients with Del (17p) or mutation of TP53 gene.
Venetoclax is a potent, selective BCL2 (B-Cell Lymphoma 2) inhibitor. BCL2 is an anti-apoptotic protein which tends to be overexpressed in CLL monoclonal cells. Venetoclax binds with the BH3 region in BCL2 and prevents bonding the BIM protein which results in the surge of mitochondrial outer membrane permeabilization (MOMP), activation of the Caspase cascade and the death of the cell. The most common undesirable effects reported during clinical trials when treated with venetoclax monotherapy or in combination with rituximab or obinutuzumab [14] were (>=20% recurrence): neutropenia/neutrophil count decreased, diarrhoea, nausea, anaemia, fatigue, and upper respiratory tract infection [15]. Some reports (post clinical trials) of AIHA triggered by Venetoclax ad0+d9ministration were published to the date [16, 17, 18], and as underlines the following case study-such incidents requires attention from both the clinicians and researchers in terms of finding suitable modifications to the treatment in such incident. Single incidence of AIHA which happen in the same time as introducing a new drug in our opinion should not permanently disqualify a patient from novel line of overall benefiting treatment such as Venetoclax.
Case Report
A 60-year-old woman was evaluated in the hospital because of the hemolysis that occurred 6 weeks after initiating the ambulatory treatment with Venetoclax for a relapsed chronic lymphocyte leukaemia. Nine years before current presentation (03.2012) the patient searched for medical care because of the sudden neck mass that was easily palpitated by the patient. Clinicians at the other hospital to which the patient presented to diagnosed in the physical examination cervical lymphadenopathy that was more prominent on the left side of the neck. No other symptoms were reported at the time by the patient. Initial laboratory test results showed normal count of white blood cells and other blood components but 30% of the peripheral venous blood white cells showed the phenotype resembling that of CLL clones. Biopsy of 2 enlarged (15mm) cervical nodes was notable for a hardly distinguishing lymph node structure with a big areas of infiltration of small B-cells that after immunohistochemical staining revealed monoclonal phenotype characteristic for CLL/SLL (CD 20+, CD23+, cycline D1-). The patient was under haematological observation from that period on.
On September 2014 the patient reached the treatment criteria’s for CLL as her lymphocytes count in peripheral blood rapidly surged to over 30 G/L with 97% being B-cells. Detailed assessment of clonal character of the cells revealed monoclonal phenotype in 90% of B-cells (Cd5+100% cd20+94% weak/ medium expression; cd10- ; cd22+ 72% weak expression cd23+ 97% with variable expression; Cd22/23 71%;kappa chains + 70% weak expression;
cd38+<1% with expression of<30% ; cd200+ 100% ; cd43+ 99%; cd71+ 1%). At this time patient developed also lymphadenopathy (many enlarged conglomerated cervical lymph nodes up to 50mm diameter, axillary lymph nodes conglomerates up to 34mm diameter, inguinal lymph nodes up to 27mm diameter and abdominal lymph nodes up to 40mm diameter -> which defines stage B in Binet classification). Bone marrow biopsy was notable of 70% infiltration of CLL cells. Molecular assessment revealed no Del (17p) or TP53 mutation.
Basing on these findings and overall good fitness the patient was qualified to immunochemotherapy with FCR regimen of standard 6 cycles [17] but discontinued it due to development of neutrophilia and anemia (requiring transfusion of 1 unit of PRBC = Packed Red Blood Cells). Though the FCR immunochemotherapy regimen was not completed, the patient achieved a long remission period during which she remained under surveillance of haematological outpatient clinic.
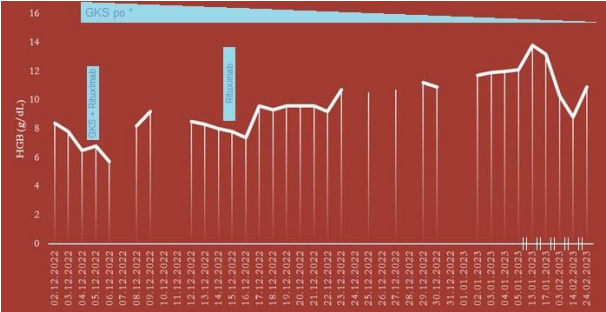
In March of 2019 the patient laboratory findings revealed clear relapse of CLL notable for white blood cell count surge to over 100 G/L and platelet count of just a 9 G/L (4. Stage of CLL in Rai classification). Patient received prednisone orally in the dose of 40mg per day due to platelet count drop. Molecular reevaluation of Del (17p) and/or TP53 mutation status remained negative. Patient started a monotherapy with bendamustine followed shortly by one cycle of RFC immunochemotherapy and one cycle of R-CD (rituximab, cyclophosphamide, dexamethasone in June 2019. Patient remained under close haematological surveillance due to moderate anemia, low platelet count of around 50 G/L on prednisone 20mg/day and intermittent neutropenia without fever treated with subcutaneous G-CSF (filgrastim). During that period (07.2019-01.2020) patient required systematic transfusions of LD-PC (leukodepleted platelet concentration) every 4-5 days and LD-PRBC (leukodepleted packed red blood cells) every 2 weeks administered in local hospital near the place of patient’s residence. On January 2020 patient was qualified to receive electrombopag treatment for refractory thrombocytopenia but was excluded from it just before the start of the course due to rising PLT count in blood smear tests. From this time patient remained under observation and required only occasional LD-PRBC transfusions last of which was administered on June 2020 (Figure 1).
Six weeks before current presentation, the patient was evaluated for signs of progression of CLL in an outpatient clinic of the hospital. A sudden surge in the lymphocyte count and moderate anemia prompted a necessity of starting new treatment with Venetoclax taken daily per os followed by Rituximab infusion after 5 weeks of treatment.
On 02.12.2022, that is one day before the presentation, patient reported debilitating lack of energy and headaches. Next day she was admitted to the hospital. Initial laboratory findings suggested autoimmune haemolytic anemia (AIHA) probably triggered by a new medication taken by the patient. Her haemoglobin concentration on admission was 7.8 g/dL, LDH (lactate dehydrogenase): 378mg/ mL, reticulocyte 4,49% of peripheral red blood cells, low haptoglobin <7,25mg/dL and positive DAT test revealing warm auto-antibodies in IgG class, cold auto-antibodies in IgM class, auto-antibodies in IgA class and complement components of C3c and C3d. Venetoclax treatment was terminated and anti-AIHA medications were given to the patient – that is methylprednisolone intravenously two days in boluses and one Rituximab infusion on the first day of methylprednisolone intake. At the same time central venous catheter was set up on patient. After 3 plasmapheresis and 4 transfusions of leucodepletion packed red blood cells (LD- PRBC) units in the following days patient’s clinical state has improved. Due to low immunoglobulin count in various classes patient remained on anti-infectious prophylaxis with trimethoprim-sulfamethoxazole and acyclovir. To prevent any further autoimmune complications, prednisone in the dose of 60mg per day was given during the rest of hospitalization (the dose has been gradually being reduced to 10mg per day when leaving the hospital) with second dose of Rituximab administered two weeks after presentation. During the second week patient developed symptoms of regional tissue infection near the central catheter with redness and tenderness around access. Blood samples for microbiological assessment was taken and empirical treatment with vancomycin and cefepime intravenously was administered. Laboratory results revealed Staphylococcus epidermidis MRSE (meticilin resistant S. Epidermidis) and Staphylococcus hominis cultures (Tables 1 & 2). Thus alteration to the antibiotic treatment was made with impanel instead of cefepime (according to the antibiogramm). After the clinical state as well as laboratory findings of the patient improved in the following day, the decision was made by the Clinic Leading Staff to try to reintroduce the Venetoclax + Rituximab CLL treatment regimen under careful observation of patient’s clinical state and signs of haemolysis. On 02.01.2023 the regimen was reintroduced and after 3 days the patient was transferred to ambulatory care which consisted of weekly full blood count and haemolytic markers assessment with haematological consultation in the clinic and elective Rituximab administration according to the treatment regimen. Full two months into reintroduction of the Venetoclax patient suffers from no haemolytic complications and her clinical state enables regular everyday functioning.
| Variable | Reference Range, Adults, This Hospital | On Presentation, This Hospital |
|---|---|---|
| RBC (mln/uL) | 3,8-5,2 | 2,3 Partially dysmorphic |
| Haemoglobin (g/dL) | 12,0-16,0 | 7,8 |
| Hematocrit (%) | 37-47 | 23 |
| MCH (pg) | 27-32 | 36,5 |
| MCHC (g/dL) | 32-36 | 36,9 |
| MCV (fl) | 80-97 | 98,9 |
| White Blood Count (G/L) | 10-Apr | 5,93 |
| -Lymphocytes (G/L) | 4-Jan | 3,38 |
| -Neutrophiles (G/L) | 1,5-7,5 | 2,42 |
| -Monocytes (G/L) | 0,1-1,3 | 0,10 |
| - Eosinophils (G/L) | 0-0,3 | 0,02 |
| -Basophils (G/L) | 0-0,2 | 0,00 |
| RET (%) | 0,54-2,02 | 4,49 |
| ALT (U/L) | 30-Jul | 27 |
| AST (U/L) | May-40 | 21 |
| Bilirubin (mg/dL) | 0,2-1,2 | 1,11 |
| Platelet count (G/L) | 150-400 | 182 |
| MPV (fl) | 6,8-11 | 9,7 |
| PDW (fl) | 10,8-16,8 | 9,8 |
| PCT (%) | 0,19-0,33 | 0,18 |
| LDH (U/L) | 135-225 | 378 |
| CRP (mg/L) | 0-10 | 5,3 |
| D Dimer (ng/mL) | 0-500 | 499 |
| NT-proBNP (pg/mL) | 0-125 | 125 |
| Troponin-I (ng/L) | 0-60 | 13 |
| Creatinine (mg/dL) | 0,5-1 | 1,18 |
Table 1: Chart of patients initial results on admission to the hospital in comparison with hospital laboratory reference ranges.
| Day of the patient’s stay | LDH (U/L) 135-225 | Bilirubin (mg/dL) 0.2-1.2 | Indirect Bilirubin (mg/ dL) 0.2-1 | Direct Bilirubin (mg/dL) <0.2 | Ret (G/L) 0.03-0.1 | Ret% 0.54-2.02 | HGB (g/ dL) | WBC (G/L) |
|---|---|---|---|---|---|---|---|---|
| 02.12.2022 | 430 | 1.08 | 0.74 | 0.34 | 0.09 | 4.49 | 8,4 | 5.93 |
| 03.12.2022 | 378 | 1.11 | 0.102 | 4.43 | 7,8 | |||
| 04.12.2022 | 0,067 | 3.72 | 6,5 | |||||
| 05.12.2022 | 296 | 1.13 | 0.044 | 2.78 | 6.8 | |||
| 06.12.2022 | 246 | 0.75 | 0.42 | 0.33 | 0.034 | 2.44 | 5.7 | 7.56 |
| 07.12.2022 | 226 | 0.75 | 0.44 | 0.31 | 0.037 | 1.81 | 6.76 | |
| 08.12.2022 | 185 | 0.73 | 0.41 | 0.32 | 0.024 | 8.2 | 3.9 | |
| 09.12.2022 | 166 | 0.54 | 0.31 | 0.23 | 0.035 | 0.97 | 9.2 | |
| 10.12.2022 | 166 | 0.52 | 0.065 | 1.35 | ||||
| 11.12.2022 | 174 | 0.64 | 2.78 | |||||
| 12.12.2022 | 184 | 0.72 | 0.47 | 0.25 | 0.109 | 8.5 | ||
| 13.12.2022 | 181 | 0.72 | 0.42 | 0.3 | 0.125 | 8.3 | ||
| 14.12.2022 | 168 | 0.69 | 0.115 | 8 | 4.67 | |||
| 15.12.2022 | 160 | 0.11 | 7.8 | 5.03 | ||||
| 16.12.2022 | 191 | 0.08 | 7.4 | |||||
| 17.12.2022 | 174 | 9.6 | ||||||
| 18.12.2022 | 177 | 9.3 | ||||||
| 19.12.2022 | 193 | 0.085 | 2.95 | 9.6 | ||||
| 20.12.2022 | 0.142 | 4.93 | 9.6 | 7.6 | ||||
| 21.12.2022 | 0.19 | 6.58 | 9.6 | 8.1 | ||||
| 22.12.2022 | 226 | 0.19 | 6.15 | 9.2 | 7.42 | |||
| 23.12.2022 | 0.46 | 10.7 | ||||||
| 24.12.2022 | ||||||||
| 25.12.2022 | 254 | 0.54 | 10.5 | |||||
| 26.12.2022 | ||||||||
| 27.12.2022 | 0.54 | 10.7 | ||||||
| 28.12.2022 | ||||||||
| 29.12.2022 | 267 | 0.54 | 0.32 | 0.22 | 0.118 | 3.6 | 11.2 | 7.97 |
| 30.12.2022 | 276 | 0.49 | 0.29 | 0.2 | 0.102 | 3.14 | 10.9 | 8.46 |
| 31.12.2022 | ||||||||
| 01.01.2023 | ||||||||
| 02.01.2023 | 267 | 0.5 | 0.3 | 0.2 | 0.085 | 2.54 | 11.7 | 7.31 |
Table 2: Haemolytical markers survived during patients stay at the hospital. WBC -White Blood Count attached as a CLL clinical co
| 03.01.2023 | 0.48 | 0.085 | 2.45 | 11.9 | 2.2 | |||
|---|---|---|---|---|---|---|---|---|
| 04.01.2023 | 285 | 0.56 | 0.072 | 2.07 | 12 | 2.06 | ||
| 05.01.2023 | 269 | 0.59 | 0.077 | 2.18 | 12.1 | 1.83 | ||
| - | ||||||||
| 13.01.2023 | 248 | 13.8 | 2.41 | |||||
| - | ||||||||
| 17.01.2023 | 255 | 0.057 | 1.49 | 13.2 | 3.78 | |||
| 03.02.2023 | 286 | 0.56 | 10.3 | 2.63 | ||||
| 14.02.2023 | 289 | 0.28 | 0.02 | 0.78 | 8.8 | 3.3 | ||
| 24.02.2023 | 293 | 0.16 | 10.9 | 8.94 |
Table 3: Haemolytical markers survived during patients stay at the hospital. WBC -White Blood Count attached as a CLL clinical co
Discussion
The drug Venetoclax administered in CLL patients is a relatively new drug and the data regarding Venetoclax induced AIHA is limited. The data provided in the product information [19, 20], the data sheets provided by EMEA [19] does not provide much information on AIHA being an adverse effect of Venetoclax therapy. Many reports for example Eudra Vigilance’s database has shown AIHA as adverse event of Venetoclax throughout Europe. A report by Stilgenbauer, et al. published in 2016 also indicated AIHA as an adverse event of Venetoclax. AEMPS report too indicated that 4.4% of patients recruited in Venetoclax clinical trials experienced AIHA as an adverse reaction of Venetoclax. The mechanism of AIHA induced Venetoclax is poorly understood, but the probable mechanism by which Venetoclax may induce AIHA is either by altering erythrocyte antigens which in turn produce antibodies which cross react with unaltered antigens. The next probable mechanism of Venetoclax induced AIHA is by association of Venetoclax with erythrocyte structures, which further would generate an antigen that would trigger an immune reaction and these remains a dilemma in clinical practice that a drug which is used to treat AIHA can de-facto in itself causes AIHA as its adverse event.
Here in the above presented case study, we have shown that the patient had AIHA evidently shown by laboratory results .now the question remains whether the AIHA was caused by clinical course of this disease. As about 5-10% AIHA of CLL can be caused by the disease itself. But there have been case studies [16, 21, 22] and certain studies where it was shown that even among 5% of patients with CLL treated with Venetoclax, AIHA can occur due to Venetoclax. In a study of 350 patients treated with Venetoclax at a daily dose of 400 mg daily, 17 patients developed AIHA due to treatment with Venetoclax. The authors ruled out other causes of AIHA and their conclusion was AIHA in the 17 patients was due to Venetoclax treatment. But in this study only 2 patients discontinued treatment with Venetoclax treatment. Observing the data, case reports, and studies from the world over us also continued the treatment for our patient with Venetoclax at the same dose after managing the AIHA exacerbation with immunosuppressive therapies (steroids, Rituximab). After attaining a good control of Autoimmune hemolysis (decrease in LDH, bilirubin levels, increase in haemoglobin levels), we again started treatment of Venetoclax safely.
Conclusion
Venetoclax - a drug administered to treat AIHA in CLL patients can in itself be a cause of AIHA. Thus a careful surveillance, analysis of the patients receiving Venetoclax is necessary whenever AIHA which occurred in a patient receiving Venetoclax is due to Venetoclax or due to disease itself and after exclusion of other factors, if it is concluded or if there is a suspicion that AIHA occurred due to Venetoclax, a short immunosuppressive therapy with say steroids or Rituximab can be administered with a good control of AIHA. Which would further allow us to continue therapy with Venetoclax? Discontinuation of Venetoclax as per data provided from case reports or studies is only necessary in a very few patients. Also it is worth mentioning that since Venetoclax induced AIHA, if it occurred should be reported to various agencies, so that physicians planning treatment with drug in future have a detailed information of this potential side effect (AIHA induced by Venetoclax), however rare and usually effectively managed by immunosuppressive drugs(Rituximab)/steroids.
References
-
Redaelli A, Laskin BL, Stephens JM, Botteman MF, Pashos CL (2004) The clinical andepidemiological burden of chronic lymphocytic leukaemia. EurJ Cancer Care (Engl) 13(3): 279-287.
-
Hallek M, Cheson BD, Catovsky D, Cappio FC, Dighiero G, et al. (2018) iwCLL guidelines fordiagnosis, indications for treatment, response assessment, andsupportive management of CLL. Blood 131(25): 2745-2760.
-
Hus I, Roliński J (2015) Current concepts in diagnosis and treatment of chronic lymphocytic leukemia. Contemp Oncol (Pozn) 19(5): 361-367.
-
Cerhan JR, Slager SL (2015) Familial predisposition and genetic risk factors for lymphoma. Blood 126(20): 2265- 2273.
-
Yoshino T, Tanaka T, Sato Y (2020) Differential diagnosis of chronic lymphocytic leukemia/small lymphocytic lymphoma and other indolent lymphomas, including mantle cell lymphoma. J Clin Exp Hematop 60(4): 124- 129.
-
Raanani P, Gafter-Gvili A, Paul M (2009) Immunoglobulin prophylaxis in chronic lymphocytic leukemia and multiple myeloma: systematic review and meta-analysis. Leuk Lymphoma 50(5): 764-772.
-
Rogers KA, Woyach JA (2016) Secondary Autoimmune cytopenias in chronic lymphocytic leukemia. Semin Oncol 43(2): 300-310.
-
Brewer JD, Habermann TM, Shanafelt TD (2014) Lymphoma-associated skin cancer: incidence, natural history, and clinical management. Int J Dermatol 53(3): 267-274.
-
Puła B, Jamroziak K, Wróbel T, Giannopoulos K, Hus I (2022) IGHV mutational status and the choiceof first-line therapy for patientswith chronic lymphocytic leukaemia. Hematology in Clinical Practice 13(1): 7-14.
-
Catherwood MA, Gonzalez D, Donaldson D, Clifford R, Mills K, et al. (2019) Relevance of TP53 for CLL diagnostics. J Clin Pathol 72(5): 343-346.
-
Costello J, Kang M, Banerji V (2021) Frontline Treatment of the Young, Fit Patient with CLL: A Canadian Perspective. Curr Oncol 28(5): 3825-3835.
-
Eichhorst B, Hallek M, Goede V (2018) Management of unfit elderly patients with chronic lymphocytic leukemia. Eur J Intern Med 58: 7-13.
-
Kay NE, Hampel PJ, Van Dyke DL, Parikh SA (2022) CLL update 2022: A continuing evolution in care. Blood Rev 54: 100930.
-
Hampel PJ, Parikh SA (2022) Chronic lymphocytic leukemia treatment algorithm. Blood Cancer J 12(11): 161.
-
Ryan CE, Davids MS, Hermann R, Shahkarami M, Biondo J, et al. (2022) MAJIC: a phase III trial of acalabrutinib+venetoclax versus venetoclax+obinutuzumab in previously untreated chronic lymphocytic leukemia or small lymphocytic lymphoma. Future Oncol 18(33): 3689-3699.
-
Carriles C, Ordóñez-Fernández L, Arias-Martínez A, Menárguez-Blanc R, Rosado-María MC (2019) Autoimmune hemolytic anemia, adverse event to venetoclax. Farm Hosp 43(5): 166-167.
-
Hadjiaggelidou C, Douganiotis G, Tsirou K, Verrou E, Triantafyllou T, et al. (2021) A rare case of autoimmune hemolytic anemia during venetoclax therapy for relapsed chronic lymphocytic leukemia. Leuk Lymphoma 62(12): 3054-3056.
-
Abdel-Samad N, Sughayar R (2021) Can Treatment with Venetoclax for Chronic Lymphocytic Leukemia (CLL) Result In Autoimmune Hemolytic Anemia? Am J Case Rep 22: e928514.
-
Stilgenbauer S, Eichhorst B, Schetelig J, Coutre S, Seymour JF, Munir T, et al. (2016) Vene- toclax in relapsed or refractory chronic lymphocytic leukaemia with 17p deletion: a multicentre, open-label, phase 2 study. Lancet Oncol 17(6): 768-778.
-
European Medicines Agency (2019) Ficha Técnica de Venetoclax (Venclyxto®).
-
Lacerda MP, Guedes NR, Yamakawa PE, Pereira AD, Fonseca ARBMD, et al. (2017) Treatment of refractory autoimmune hemolytic anemia with vene- toclax in relapsed chronic lymphocytic leukemia with del (17p). Ann Hematol 96(9): 1577-1578.
-
(2022) Informe de Posicionamiento Terapéutico de venetoclax (Venclyxto) en leucemia linfocítica crónica.
-
Wen X, He Y, Wang S, Wang L (2019) Drug-induced hemolytic crisis during ibruti- nib plus venetoclax therapy for the treatment of mantle-cell lymphoma: A rare hematologic adverse reaction. Aging Pathobiol Ther 1(1): 25-28.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies