Funnel and Vessel-Duct Adenoma Breast
Duct adenoma appears as an exceptionally discerned, benign tumefaction comprised of distorted glandular articulations circumscribed within a fibrous tissue capsule and intermingled within a sclerotic stroma. Initially scripted Azzopardi and Salm in 1984, the adenomatous lesion is configured of miniature and intermediate ducts disseminated within peripheral breast tissue. Alternative nomenclature of sclerosing papilloma is not recommended.
Editorial
Duct adenoma appears as an exceptionally discerned, benign tumefaction comprised of distorted glandular articulations circumscribed within a fibrous tissue capsule and intermingled within a sclerotic stroma. Initially scripted Azzopardi and Salm in 1984, the adenomatous lesion is configured of miniature and intermediate ducts disseminated within peripheral breast tissue. Alternative nomenclature of sclerosing papilloma is not recommended.
Neoplasm appears as a solitary, well circumscribed, solid proliferation of tubules enmeshed within fibrous tissue stroma with circumscribing thickened wall constituted of fibro-elastotic tissue. Occasionally, multi-nodular lesions may be expounded. Neoplasm may be contemplated as a sclerotic variant of intra-ductal papilloma associated with obliteration of papillary projections. Tumefaction may exemplify focal calcification, haemorrhage, infarction, squamous metaplasia, apocrine metaplasia or epithelial hyperplasia. Circumscribing stroma delineates myxoid or chondroid alterations. Centric scar may be discerned. Neoplasm may enunciate a pseudo- infiltrative pattern of progression.
The infrequently discerned duct adenoma emerges within adult subjects > 60 years. Generally, implicated subjects lack a distinctive family history or personal history of concordant invasive carcinoma breast [1, 2]. Duct adenoma demonstrating tubular morphology may occur as a component of Carney’s complex. In contrast to intra-ductal papilloma, duct adenoma arises within miniature to intermediate ducts confined to peripheral breast parenchyma. Exceptionally, enlarged or major sub-areolar ducts may be implicated. Lesions are preponde rantly unilateral. Duct adenoma associated with Carney’s complex may arise within bilateral breasts [1, 2]. Duct adenoma is posited to arise from intra-ductal papilloma confined to miniature and intermediate ducts. Concurrent with repair processes of the stroma, papilloma may undergo sclerosis with consequent decimation of arborizing papillary architecture [2, 3]. Alternatively, direct expansion of hyperplastic process as sclerosing adenosis arising within miniature and intermediate ducts or coexisting intra-ductal papilloma may contribute to disease emergence. Centric stromal zone demonstrates degenerative alterations, akin to radial scar.
Duct adenoma of breast emerges as a proliferative lesion with genetic concurrence to papilloma. As encountered with papilloma, genetic mutations within AKT1 E17K gene may activate PIK3CA pathway which is pre-eminently accountable for cellular proliferation, cell survival, angiogenesis and cellular mobilization [2, 3]. Duct adenoma evaluated by next generation sequencing exhibits repetitive missense mutations, especially within genes as AKT1, GNAS and PIK3CA. Breast papilloma frequently expounds genetic mutations within AKT1 gene, there by indicating a concurrence of duct adenoma with aforesaid lesions. Alternatively, duct adenoma may be comprised of intra-ductal papilloma demonstrating secondary sclerosis [2, 3].
Clinically, duct adenoma represents as palpable lump. Uncommonly, nipple discharge may occur. Exceptionally, neoplasm may preliminarily be discerned as an anomaly upon mammography [2, 3].
Cytological smears are significantly cellular. Smears display innumerable branching, flattened, cohesive sheets and regularly disseminated clusters of ductal epithelial cells.
Enlarged stromal fragments of purple hue are intensely associated with epithelial cell clusters, thereby configuring intercellular dissemination of finger-like hyaline structures or globules. A population of singular cells, naked nuclei, histiocytic cells and apocrine cells appear admixed with tumour cell component. Tumour cells display miniature, punched out intracytoplasmic vacuoles. Tumour cell nuclei appear spherical or ovoid and are impregnated with bland nuclear chromatin [3, 4].
Grossly, tumefaction represents as a solid, grey/ white or whitish, lobulated nodule of magnitude varying from 0.5 centimetres to 5.0 centimetres with an average diameter of 0.85 centimetres. Tumefaction may be solitary or occasionally display multiple, adjacent nodules. Multinodular tumefaction ensues due to implication of various segments of a singular ductal system. Cut surface is granular and exhibits a centric, greyish focus of softened parenchyma. Gritty texture and streaks of elastic tissue appear reminiscent of duct carcinoma [3, 4].
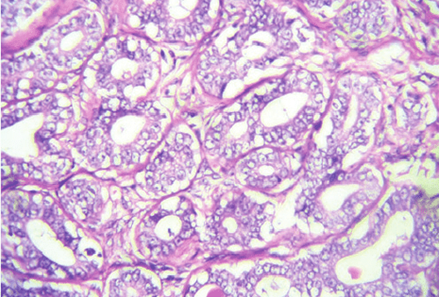
Upon microscopy, a well circumscribed, solitary or infrequently multinodular, intra-ductal lesion is enunciated. A thickened, concentric wall of fibro-elastotic tissue appears to circumscribe the neoplasm. Adenomatous segment of duct adenoma exemplifies a solid architecture comprised of proliferating tubules enmeshed within a fibrous tissue stroma. Neoplastic glands configure as spherical to elliptical, elongated or branched glandular articulations. Clusters of epithelial cells and myoepithelial cell may be discerned although myoepithelial cell aggregates may be inconspicuous [3, 4]. Columnar or spindle shaped ductal epithelial cells configure the neoplasm. Cellular and nuclear atypia is absent. Mitotic figures are sparse to absent. Morphological alterations as cystic dilatation of glands, epithelial hyperplasia, apocrine metaplasia, squamous metaplasia, eosinophilic secretions or laminated calcific aggregates may be discerned. Encompassing fibrous tissue stroma is moderate and may exemplify myxoid alterations, prominent focal hyalinization and exceptionally discerned cartilaginous metaplasia. Frequently, focal compression of glands may ensue, akin to lesions of sclerosing adenosis [3, 4].
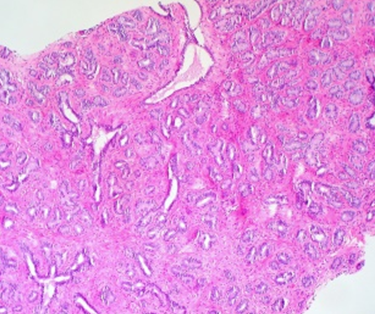
Glandular structures appear distorted and entrapped within the sclerotic wall with consequent emergence of pseudo-infiltrative pattern. Foci of glandular proliferation appear to protrude into encompassing tissue with the articulation of a ‘pushing’ tumour margin. Duct wall may delineate foci of dystrophic calcification and periductal aggregates of chronic inflammatory cells [3, 4].
Stellate tumour configuration expounds centric foci of fibroelastosis along with entrapped epithelial tubules and peripheral distension of glandular elements, thereby simulating a radial scar. Secondary alterations as haemorrhage or infarction may occur. Morphological features as arborizing papillary fronds, as observed within intra-ductal papilloma, focal myoepithelial hyperplasia or adenomyoepithelioma, appear absent [4, 5].
Staging of carcinoma breast as per American Joint Committee on Cancer (AJCC) 8th edition [3, 4].
Primary Tumour
TX: Primary tumour cannot be assessed T0: No evidence of primary tumour Tis: Tumour appearing as ductal carcinoma in situ, Paget’s disease, encapsulated papillary carcinoma and solid papillary carcinoma ~Tis (DCIS) appearing as ductal carcinoma in situ devoid of invasive carcinoma ~Tis (Paget) appearing as Paget’s disease devoid of invasive carcinoma T1mi: Tumour ≤ 1 millimetre magnitude T1a: Tumour > 1 millimetre and ≤ 5 millimetre magnitude T1b: Tumour > 5 millimetre and ≤ 10 millimetre magnitude T1c: Tumour > 10 millimetre and ≤ 20 millimetre magnitude T2: Tumour > 20 millimetre and ≤ 50 millimetre magnitude T3: Tumour > 50 millimetre magnitude T4a: Tumour extension into chest wall and devoid of infiltration into pectoralis muscle T4b: Tumour associated with oedema as peau d’orange, cutaneous ulceration and ipsilateral satellite cutaneous nodules T4c: Tumour demonstrating features of T4a and T4b T4d: Tumour demonstrating inflammatory carcinoma which implicates > 1/3 of cutaneous surface of breast and is discerned upon clinical examination.
Regional Lymph Nodes
NX: Regional lymph nodes cannot be assessed N0: Regional lymph node metastasis absent N0(i-): Regional lymph node metastasis absent upon histological assessment or immunohistochemistry N0(i+): Regional lymph nodes depicting isolated tumour cells or a cluster of tumour cells ≤ 0.2 millimetre diameter or < 200 cells N0(mol+): Regional lymph nodes delineating tumour cells upon reverse transcriptase polymerase chain reaction (RT- PCR) and non-discernible upon light microscopy N1mi: Regional lymph nodes with micro-metastasis or tumour deposit > 0.2 millimetre and ≤ 2.0 millimetre or ≤ 0.2 millimetre and > 200 cells N1a: Regional lymph node metastasis within one to three 3 axillary lymph nodes with minimally a singular tumour deposit > 2.0 millimetre diameter N1b: Regional lymph node metastasis into internal mammary sentinel lymph node with tumour deposit > 2.0 millimetre diameter N1c: is constituted of combined N1a and N1b N2a: Regional lymph node metastasis into 4 to 9 axillary lymph nodes with minimally a singular tumour deposit > 2.0 millimetre diameter N2b: Regional lymph node metastasis within clinically palpable internal mammary lymph nodes and axillary lymph nodes devoid of tumour deposits N3a: Regional lymph node metastasis into ≥ 10 axillary lymph nodes with minimally a singular tumour deposit > 2.0 millimetre magnitude or metastasis into infra-clavicular lymph nodes N3b: Regional lymph node metastasis into internal mammary lymph nodes as discerned upon imaging and tumour stage appearing as N1a or N1b N3c: Regional lymph node metastasis into ipsilateral supraclavicular lymph nodes
Distant Metastasis (M)
M0: Distant metastasis absent M1: Distant metastasis present with magnitude of histological tumour deposits > 0.2 millimetres y: adoption of preoperative radiotherapy or chemotherapy r: recurrent tumour stage Luminal cells of duct adenoma breast appear immune reactive to keratin. Myoepithelial cells appear immune reactive to S100 protein, actin and p63. Intact myoepithelial cells immune reactive to p63 or smooth muscle myosin heavy chain (SMMHC) may be discerned which excludes true neoplastic invasion. Basement membrane appears immune reactive to laminin or type IV collagen. Stromal component composed of spindle shaped cells or myo-fibroblasts appear immune reactive to actin or vimentin.
Tumour cells demonstrate a heterogeneous staining pattern with CK5/6 and oestrogen receptors Neoplastic cells are immune non-reactive to p53.
Duct adenoma exemplifies minimal Ki67 proliferative index [5, 6].
Duct adenoma requires segregation from neoplasms as intra-ductal papilloma, tubular adenoma or fibroadenoma breast [5, 6].
Duct papilloma may simulate duct carcinoma upon clinical assessment, imaging features and evaluation of fine needle aspiration cytology smears or core needle biopsy samples [6, 7].
Surgical excision of the lesion is frequently recommended as tumefaction simulates duct carcinoma on morphological assessment and radiographic evaluation.
Upon imaging, duct adenoma breast may indicate lesions of papilloma, fibroadenoma or duct carcinoma. Mammography expounds a well-defined or inadequately defined tumour mass with coexistent calcification. Alternatively, tumefaction may be devoid of calcification.
Ultrasonography exemplifies a well-defined, spherical, hypoechoic tumour nodule with shadowing and posterior image enhancement. Contrast enhanced magnetic resonance imaging (MRI) expresses a smooth tumour perimeter regardless of discernible histological foci of neoplastic pseudo-invasion [6, 7].
Comprehensive surgical extermination of the neoplasm can be optimally employed with curative intent. Subsequent to cogent surgical extermination, the benign duct adenoma appears devoid of enhanced possible emergence of tumour reoccurrence or malignant transformation. However, malignant metamorphosis into apocrine carcinoma or epithelial- myoepithelial carcinoma is documented [6, 7].
References
-
Daly C, Puckett Y (2024) New Breast Mass. Stat Pearls International. Treasure Island, USA.
-
Weigelt MA, Sciallis AP, McIntire PJ, Jennifer SK, Steven DB, et al. (2023) Nipple Adenoma: Clinicopathologic Characterization of 50 Cases. Am J Surg Pathol 47(8): 926-932.
-
Skaribas EE, Tschen J (2023) Growth of a Nipple Adenoma after Estrogen Replacement Therapy. Cureus 15(12): e50843.
-
Park SK, Samat SH, Whitelock CM, Thais F (2023) Syringomatous adenoma of the nipple: A case series and systematic review. Clin Case Rep 11(6): e7521.
-
Joo GJ, Carter GJ, Berg WA (2023) Tubular Adenoma of the Breast: Radiologic-Pathologic Correlation. J Breast Imaging 5(6): 703-711.
-
Combi F, Palma E, Montorsi G, Anna G, Silvia S, et al. (2023) Management of nipple adenomas during pregnancy: a case report. Int Breastfeed J 18(1): 19.
-
Ajmal M, Khan M, Fossen K (2024) Breast Fibroadenoma. Stat Pearls International. Treasure Island, USA.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies