Suety and Spreading-Stromal Hyperplasia and Hyperthecosis Ovary
Stromal hyperplasia of the ovary emerges as a nonneoplastic, functional disorder delineating nodular or diffuse proliferation of ovarian stroma. Ovarian hyperthecosis typically demonstrates proliferation of ovarian stroma along with luteinization of stromal cells. Diffuse or nodular proliferation of ovarian stroma may represent as singular cells and clusters or nodules of luteinized cells. The condition is associated with excessive androgen production with consequently elevated serum testosterone levels. In contrast to normal ovaries, ovaries with stromal hyperplasia and hyperthecosis secrete significant quantities of androstenedione which may metabolize into oestradiol with peripheral aromatization. Emerging endometrial pathology may manifest with clinical symptoms as vaginal bleeding. Alternatively, symptoms of hyperandrogenism as androgenetic alopecia or hirsutism may concur with elevated serum testosterone levels. Commonly confined to ovarian stroma, stromal hyperplasia with hyperthecosis is encountered within postmenopausal women. Condition may arise within 51 years to 64 years with average age of disease emergence at 55 years. Women within reproductive age group are infrequently implicated (< 1%)
Abbreviations
LH: Luteinizing Hormone; HAIR-AN: Hyperandrogenism, Insulin Resistance and Acanthosis Nigricans; FIGO: International Federation of Gynecology and Obstetrics; WT1: Wilm’s Tumour 1; ER: Oestrogen Receptor; PR: Progesterone Receptor; EMA: Epithelial Membrane Antigen; FSH: Follicle Stimulating Hormone.
Editorial
Stromal hyperplasia of the ovary emerges as a non- neoplastic, functional disorder delineating nodular or diffuse proliferation of ovarian stroma. Ovarian hyperthecosis typically demonstrates proliferation of ovarian stroma along with luteinization of stromal cells. Diffuse or nodular proliferation of ovarian stroma may represent as singular cells and clusters or nodules of luteinized cells. The condition is associated with excessive androgen production with consequently elevated serum testosterone levels. In contrast to normal ovaries, ovaries with stromal hyperplasia and hyperthecosis secrete significant quantities of androstenedione which may metabolize into oestradiol with peripheral aromatization. Emerging endometrial pathology may manifest with clinical symptoms as vaginal bleeding. Alternatively, symptoms of hyperandrogenism as androgenetic alopecia or hirsutism may concur with elevated serum testosterone levels.
Commonly confined to ovarian stroma, stromal hyperplasia with hyperthecosis is encountered within postmenopausal women. Condition may arise within 51 years to 64 years with average age of disease emergence at 55 years. Women within reproductive age group are infrequently implicated (< 1%) [1, 2].
Of obscure aetiology, ovaries demonstrating stromal hyperplasia and hyperthecosis secrete significant quantities of androstenedione and oestradiol, in contrast to normal ovaries. Majority of subjects with stromal hyperplasia and hyperthecosis delineate normal serum gonadotrophin levels, in contrast to polycystic ovarian syndrome [1, 2]. Stromal cellular proliferation within premenopausal and postmenopausal women appears enhanced with secretion of luteinizing hormone (LH) wherein luteinizing hormone augments androgen production within ovaries along with or devoid of stromal hyperplasia. Stromal hyperplasia and hyperthecosis is preponderantly associated with hyperinsulinemia or insulin resistance, a feature implicated in disease pathogenesis [1, 2]. Occasional instances manifest a genetic aetiology. Condition may be concordant with hyperandrogenism, insulin resistance and acanthosis nigricans (HAIR-AN) syndrome [1, 2]. Clinically, stromal hyperplasia and hyperthecosis demonstrates signs and symptoms of hyperandrogenism as deepened voice, acne, hirsutism, frontal alopecia or clitoromegaly. Additionally, features as obesity, hyperinsulinemia, acanthosis nigricans and metabolic syndrome may ensue. Enhanced possible occurrence of vaginal bleeding, endometrial hyperplasia, endometrial carcinoma, cardiovascular conditions or diabetes mellitus may be observed [2, 3]. Few subjects with stromal hyperplasia with hyperthecosis may expound hyperandrogenism, insulin resistance and acanthosis nigricans (HAIR-AN) syndrome [2, 3]. Grossly, bilateral ovaries are commonly implicated. Ovarian magnitude appears amplified. Ovarian enlargement may be nodular or diffuse wherein the ovary appears as solid and firm. Cut surface is homogeneous, grey/ white to yellow [3, 4].
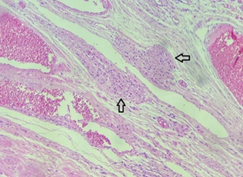
Upon microscopy, diffuse or nodular proliferation of ovarian stroma appears confined to the cortex, medulla or within cortico-medullary zones. Stromal proliferation appears comprised of spindle shaped cells disseminated within scanty, intervening collagen fibrils. Stromal hyperplasia may appear as diffuse areas or represent as a singular nodule with subsequent coalescence of nodules. Foci of hyperplasia may depict entrapped follicular derivatives [3, 4]. Stromal hyperthecosis manifests as singular cells, cell nests or nodules of polygonal, luteinized theca cells impregnated with eosinophilic or clear cytoplasm. Generally, cellular nodules < 1 centimetre diameter are encountered [3, 4].
The International Federation of Gynaecology and Obstetrics (FIGO) staging system is commonly adopted for staging benign and malignant ovarian neoplasms and is denominated as 1. Stage I: tumor confined to the ovaries. • ~Stage Ia: tumor confined to singular ovary with intact ovarian capsule, absent tumors cells upon ovarian surface and absence of malignant cells within ascites or peritoneal washings. • ~Stage Ib: tumor implicating dual ovaries while simulating stage Ia, intact ovarian capsule, absent tumor cells upon ovarian surface and absence of malignant cells within ascites or peritoneal washings. • ~Stage Ic: tumors infiltrates singular or dual ovaries along with any feature designated as • Stage Ic1: tumor associated with surgical or intraoperative spill. • Stage Ic2: tumor capsule ruptured prior to surgical intervention or tumors dissemination upon ovarian or fallopian tube surface. • Stage Ic3: appearance of malignant cells within ascites or peritoneal washings. 2. Stage II: tumor involves singular or bilateral ovaries along with tumor extension into pelvic cavity below the pelvic brim or primary peritoneal carcinoma. • ~Stage IIa: tumor extension or implants within the uterus or fallopian tubes. • ~Stage IIb: tumor extension into various pelvic intraperitoneal tissues. 3. ~Stage III: tumor implicates singular or dual ovaries or fallopian tubes with definitive cytological or histological dissemination into the peritoneum beyond pelvis along with or devoid of tumor metastasis into retroperitoneal lymph nodes. • ~Stage IIIa: tumors dissemination into retroperitoneal lymph nodes along with or devoid of microscopic tumor metastasis beyond the pelvis categorized as • Stage IIIa1: definitive cytological or histological assessment of tumor cells singularly confined to retroperitoneal lymph nodes. • Stage IIIa1(i): retroperitoneal lymph node with tumor metastasis ≤10 millimeter magnitude. • Stage IIIa1(ii): retroperitoneal lymph node with tumor metastasis >10 millimeter magnitude. • Stage IIIa2: discernible microscopic evidence of extra- pelvic extension superior to the pelvic brim with tumour extension into peritoneal cavity along with or absence of tumor metastasis into retroperitoneal lymph nodes. • Stage IIIb: discernible or macroscopic tumor metastasis into peritoneal cavity beyond the pelvis ≤2 centimeters in greatest dimension along with or devoid of tumor metastasis into retroperitoneal lymph nodes and tumor extension into capsule of liver and spleen. • Stage IIIc: discernible macroscopic tumor extension into extrapelvic tissue or peritoneal cavity >2 centimeters in greatest dimension along with or devoid of metastasis into retroperitoneal lymph nodes in addition to tumor extension into capsule of liver and spleen. 4. Stage IV: tumour is associated with distant metastasis in the absence of metastases into peritoneal cavity. • ~Stage IVa: pleural effusion with disseminated tumour cells. • ~Stage IVb: tumour associated with distant metastases. • ~Tumor metastasis into visceral parenchyma and metastases to extra-abdominal organs, inguinal lymph nodes and lymph nodes extending beyond abdominal cavity [3, 4].
Additionally, bilateral ovarian tumours may represent as stage I disease although are associated with distant metastases in ~30% subjects. Besides, majority of ovarian cancers represent as stage III lesions [3, 4].
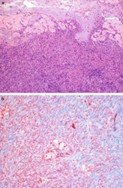
Stromal hyperplasia with hyperthecosis ovary appears immune reactive to Wilm’s tumour 1 (WT1) antigen, oestrogen receptor(ER), progesterone receptor (PR), CD56, inhibin, calretinin or FOXL2. Tumour cells appear immune non-reactive to cytokeratin AE1/AE3, epithelial membrane antigen (EMA), cytokeratin MNF116 or CD10 [5, 6].
Stromal hyperplasia and hyperthecosis requires segregation from neoplasms as ovarian fibroma, normal ovary, steroid cell tumor not otherwise specified (NOS), luteinized thecoma associated with sclerosing peritonitis, sex cord stromal tumour not otherwise specified (NOS), pregnancy luteoma, massive ovarian oedema and fibromatosis, Krukenberg’s tumour or low grade endometrial stromal sarcoma [5, 6]. Cogent demarcation is necessitated from adrenal neoplasms and androgen secreting ovarian tumors. Stromal hyperplasia and hyperthecosis may be suitably discerned and mandates clinical assessment for features as hirsutism, alopecia or deepened voice [5, 6]. Serological assessment is required to ascertain elevated serum testosterone, androgen and oestrogen levels. Besides, normal or suppressed luteinizing hormone (LH), normal dehydroepiandrosterone (DHEA), DHEA sulphate (DHEAS), 17 hydroxyprogesterone (17 OHP) and normal progesterone or prolactin levels may be observed [5, 6]. Upon imaging, enlarged ovaries devoid of hyper-vascularization are encountered [5, 6]. Morphological features are pathognomonic and beneficially employed for prospective therapy wherein bilateral salpingo- oophorectomy surgical samples may be subjected for cogent evaluation [5, 6]. Augmented serum androgen, testosterone, oestrogen levels, normal or suppressed leutinizing hormone (LH), follicle stimulating hormone (FSH) and normal serum androstenedione or dehydroepiandrosterone sulphate (DHEAS) may be encountered. Lipid profile expounds enhanced serum low density lipoprotein (LDL), triglycerides and decimated high density lipoprotein (HDL) along with hyperandrogenemia [5, 6]. Ultrasonography depicts enlarged ovaries in the absence of hyper-vascularization. Severe instances demonstrate bilateral expansion of ovarian stroma along with solid ovaries. Additionally, amplified age specific ovarian volume and ovarian nodules or cysts may be observed. Notwithstanding, quantifiable ovarian follicles appear normal, in contrast to polycystic ovarian syndrome [5, 6]. T2 weighted magnetic resonance imaging (MRI) expounds a homogeneous, hypo-intense signal along with mild ovarian enhancement [5, 6]. Postmenopausal females with stromal hyperplasia and hyperthecosis may appropriately be managed with bilateral oophorectomy. Subjects unfit for surgical intervention with several comorbid conditions may be subjected to extended duration of gonadotropin releasing hormone agonist therapy. Young women necessitating fertility preservation may be managed with extended administration of gonadotropin releasing hormone agonists [5, 6]. The benign, non-neoplastic ovarian stromal hyperplasia with hyperthecosis delineates enhanced ovarian volume and is concurrent with elevated possible emergence of carcinoma endometrium. Thus, exclusion of malignant metamorphosis is necessitated. Cogent therapy is employed in order to decimate possible occurrence of neoplastic transformation [5, 6, 7, 8].
References
-
Geist SH, Gaines JA (1942) Diffuse luteinization of the ovaries associated with the masculinization syndrome. Am J Obstet Gynecol 43(6): 975-983.
-
Metzker LS, Ferreira LAC, Borges JCN, Guzzo MF, Ferreira RN, et al. (2023) Postmenopausal Hyperandrogenism due to Ovarian Hyperthecosis. Case Rep Obstet Gynecol 2023: 2783464.
-
Yousaf S, Nizar R, John L, Simpson A (2023) A Case of Ovarian Hyperthecosis in a Postmenopausal Woman. JCEM Case Rep 1(6): luad148.
-
Shah S, Torres C, Gharaibeh N (2022) Diagnostic Challenges in Ovarian Hyperthecosis: Clinical Presentation with Subdiagnostic Testosterone Levels. Case Rep Endocrinol 2022: 9998807.
-
Lozoya AT, Monfort IR, Martin JE, Garcia AJ, Hidalgo IN, et al. (2020) Ovarian Stromal Hyperplasia: A Rare Cause of Postmenopausal Hyperandrogenism. J Menopausal Med 26(1): 39-43.
-
Bahaeldein E, Brassill MJ (2018) Utilisation of gonadotrophin-releasing hormone (GnRH) analogue to differentiate ovarian from adrenal hyperandrogenism in postmenopausal women. Endocrinol Diabetes Metab Case Rep 2018: 18-0084.
-
Image 1 Courtesy: Wiley online library.
-
Image 2 Courtesy: Basic medical key.
- How to Identify and Overcome Barriers in Developing Blood Systems?
- Why Was Transfusion Medicine Not Recognized as a Clinical Discipline?
- Outcomes of Lenalidomide Relapsed/Refractory Patients
- Is Transfusion Always Necessary?
- The Logistics of Production and Use of Blood and Blood Components
- The Challenge for Component Therapies