Post Cyclone Idai Evaluation of the Integrated Management of Acute Malnutrition (IMAM) Programme for Children under Five in Chimanimani, Zimbabwe
Background: Natural disasters like cyclones have been shown to cause food insecurity and infectious diseases leading to malnutrition. Objective: To evaluate the point prevalence of severe acute malnutrition (SAM) and moderate acute malnutrition (MAM) and post cyclone Idai Integrated Management of Acute Malnutrition (IMAM) response in Chimanimani district. Methods: A stratified random sampling method was used to select mother/child pairs who were IMAM beneficiaries. Clinic level records and reports on admissions and treatment outcome statistics were collected. Stories of most significant change (MSC), Focus Group Discussions (FDG) and Key Informants interviews were conducted. Results: At baseline, 74 children were admitted as malnourished, 25 had SAM and 49 had MAM, the number reduced to 45 with 13 SAM and 32 MAM four months post cyclone. The impact of the intervention was measured by the quality of treatment outcomes. The average cure rate from April to December for MAM was 79%, defaulter rate 19%, non-recovery 0%, died 2% and for SAM, cure rate 82%, defaulter rate 13%, died 0% and non-recovery 5%. The cure rate, non-recovery rate and death rate were in line with the SPHERE minimum standards Conclusion: The prevalence of SAM and MAM were highest two months after the cyclone with a marked reduction of cases 4 months post cyclone. The cure, death and non-recovery rate outcome indicators were desirable; however, defaulter rate compromised the effectiveness of the IMAM programme. These findings warrant the strengthening and establishment of effective defaulter follow up systems in displaced and hard to reach areas.
Introduction
Natural disasters can lead to outbreaks of infectious diseases because of change of living conditions for the affected population. Potential infectious diseases and risk factors reviewed between 2000 and 2011 due to natural disasters such as tropical cyclones, tornados and earthquakes showed that they lead to infectious diseases including diarrheal diseases and typhoid fever [1]. Food insecurity and infectious diseases lead to increase in nutrient loss and a decrease in nutrient intake. This factor may lead to an increase in mortality and morbidity for children under the age of 5 [2].
El Nino is a climate patten that describes the unusual warming of surface waters in the eastern Pacific Ocean. El nino also produces widespread and severe change in climate [3]. In 2015 Zimbabwe was severely affected by El Nino as erratic rainfall was received. This affected food security, nutrition, health, agriculture, livelihoods, hygiene, and sanitation [4]. Exacerbating the situation in 2019 Chimanimani, Nyanga, Makoni, Mutasa, Chipinge, Buhera and Mutare rural districts were hit by heavy rains with high winds caused by cyclone Idai. The cyclone caused subsequent deaths, floods, riverine and destruction of property together with livelihoods. Cyclone Idai affected the elderly, pregnant mothers, young children and the disabled. It left most people homeless; it also destroyed their food stocks and granaries [5]. The highest level of destruction was experienced in Chimanimani district at Ngangu Township and Koppa growth point where mudslides and floods were experienced respectively. Due to the high magnitude, of the disaster, an inter-agency team that comprised of non-governmental organizations and local government agencies (MoHCC) was formed. Its mandate was to assist in a coordinated manner that promoted integration of activities preventing duplication of efforts in one area. Best practices for nutrition are essential since the elderly, children and the youth constitute the greatest number of people in the continent [6].
Emergency interventions prioritize survival, nutrition interventions highly concentrate on the treatment of acute malnutrition through food distributions, therapeutic feeding, and supplementary feeding [7]. A well-organized response plan is vital in saving lives. This research explored the nature and impact of the nutrition interventions in cyclone-affected areas in Chimanimani district Zimbabwe.
Disasters result in increase in prevalence of malnutrition with increased susceptibility among the vulnerable groups especially children under-five and it is even more lethal in combination with infectious diseases for example diarrhoea and killer diseases that children are affected with. The recent Zimbabwe National Nutrition Survey indicated that the Global Acute Malnutrition at a national level was at 0.21% with inter-district variances (MAM 2.3%, SAM 0.2% for Zimbabwe and MAM 0.9%, SAM 0.8 for Chimanimani district [8]. The current prevalence of wasting in Chimanimani is 1.9% which is below WHO cut off values (Acceptable (<5%) [9]. However, following the disaster, it is expected that these prevalence percentages will increase. The study evaluated prevalence of malnutrition, effectiveness, relevance, and coverage of the nutrition response.
The purpose of this study was to assess the malnutrition post-disaster situation and nutrition interventions put in place to inform emergency preparation plans in the future hence reduce the impact of similar disasters and for the prioritization of primary health care delivery system in the absence of pre-disaster surveillance data. The research focused on post-cyclone Idai nutrition interventions for children under the age of five years in Chimanimani district. The results obtained could be helpful to health providers in emergency preparedness and implementation of improved- nutrition related interventions before and after disasters, and it will equip different organizations and the government at policy-making and implementation of nutrition-related programs.
Research questions
- What is the point prevalence of SAM and MAM in Chimanimani district?
- How effective is the IMAM programme?
- What modifications were made to the generic IMAM programming to meet the emergency needs?
Objectives of the study
Broad objective: To evaluate the point prevalence of acute malnutrition and the post cyclone Idai IMAM response in Chimanimani district.
The specific objectives of the study are:
- To determine point prevalence of SAM and MAM among the children under five in Chimanimani district.
- To assess the IMAM outcome indicators of nutrition response against the standards in Chimanimani district.
- To examine the modifications in IMAM programming in the emergency context.
Methodology
Study Setting
The study was conducted in Chimanimani district, which is found in Manicaland Province in Zimbabwe. According
to ZIMSTAT population figures by age group the district constitutes of 25197 children under five [10]. The study was conducted in the most affected areas, Ngangu Township and Koppa growth point in Chimanimani District. Ngangu Township has a total of 1124 children under-five and Koppa growth point 2063. According to Cyclone Idai situation report, 209 Ngangu and Koppa were the most affected areas in Chimanimani district, as they received mudslides and floods respectively.
Study design
The study encompassed both qualitative and quantitative methods. A participatory approach was used in the evaluation of the IMAM programme. Focus Group Discussions (FGDs) were conducted with mothers of the IMAM beneficiaries, a total of 8 FGDs were conducted, three with young mothers aged 18-29 years, two with older mothers aged 30-45 years and three with mixed ages. Each group had 10 participants. Stories of most significant change (MSCs) were conducted in form of interviews using a questionnaire to point of saturation. A total of 10 MSCs were gathered. A total of 15 key informant interviews were conducted. Programmers and implementers of the projects were interviewed to establish modifications in IMAM programming following the emergency.
Study population and Sampling
A stratified random sampling method was used to select mother/child pairs who were beneficiaries of the interventions. Mothers were grouped into two groups those aged 18-29 and those aged 30-45. Ten mothers were randomly selected in each group per health facility. Stakeholders of the nutrition interventions being implemented in Chimanimani district. Study population comprised of MoHCC, NGOs, community leaders and mothers of children under five IMAM beneficiaries. Inclusion criteria: Mothers with children under the age of 5 years who were beneficiaries visiting Family Child Health Clinic (FCHC) at Chimanimani Hospital and Ngorima clinic were included in the study. Mothers who were not beneficiaries to interventions or were not available during the cyclone were excluded.
Data collection and Tools
IMAM indicators based on health facility records and reports on admissions and treatment outcome statistics were used. Surveillance data from the start of interventions was collected at three months and six months’ intervals. Village level records on screening statistics were collected to assess programme coverage. An MSC guide with a question ‘During the last six months, in your opinion, what was the most significant change that took place for the children under the age of five regarding the programs that were implemented”? Focus Group Discussion (FGD) guide was used for FDGs. Key Informant questionnaire was used for key informants’ interviews with health workers.
Data Analysis
Data was collected, processed and analysed, IMAM indicators were analysed through calculations and comparison with sphere standards. Analysis of MSC stories were done using content analysis (themes/words) by Microsoft excels. And descriptive analysis for qualitative data. SPSS software was used to calculate descriptive statistics such as standard deviation and mean.
Ethical considerations
Ethical approval was granted by the Medical Research Council of Zimbabwe (MRCZ/B/1836) and Ministry of Health and Child Care before the study commenced. Signed informed consent was sought from each participant after explaining study procedures.
Results
Demographic data of Key informants
A total number of 15 health workers were interviewed which included five nurses, three nutritionists, one nutrition assistant, and six nutrition ward coordinators. They had a mean age of 41±15.3 years. The interviewee consisted of seven males and eight females, nine of them were married and six were single. There had a mean working experience of 12.2±9.3 years.
Challenges in assisting children under the age of five
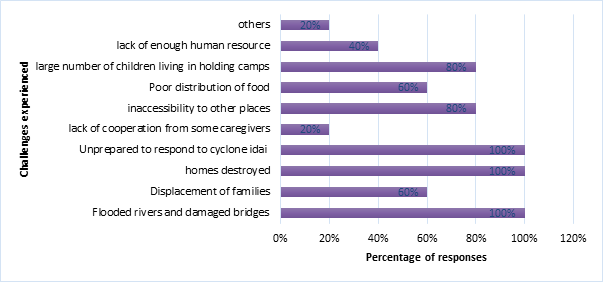
Figure 1 below indicates the challenges faced in trying to assist children under five. The common problems identified were that of flooded rivers and damaged bridges, destruction of homes and lack of emergence preparedness all of which were indicated by all the participants(n=15) Lack of human resources had 40% response which was attributed to inaccessibility of other places. Lack of cooperation from caregivers had a 20% response.
Impact of cyclone Idai in Chimanimani district
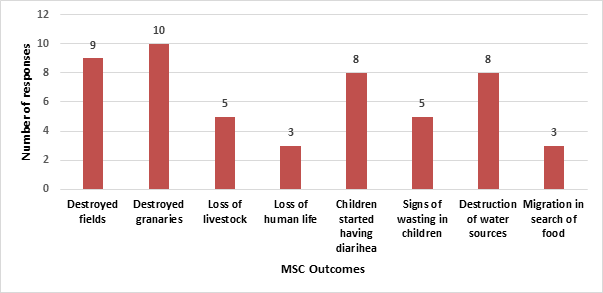
Figure 2 below shows that from 10 MSCs collected on impact of cyclone Idai in Chimanimani district. Destruction of granaries, fields, water sources and children suffering from diarrhoea had the highest responses which indicate they occurred to majority of the population in different villages. Migration in search of food and loss of life had the least responses.
Outcomes of programmes initiated after the disaster in Chimanimani
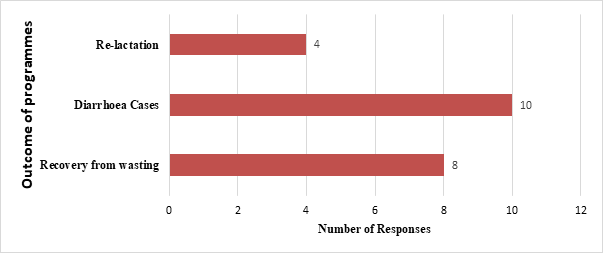
Figure 3 below indicates the significant outcomes identified through the MSCs. Decrease in diarrhoea cases had the highest response rate which shows that most of population saw the impact of the interventions done. Four interviewees reported they saw re-lactation after interventions.
Example of MSC Story
Mrs Samu (resident of koppa growth point) “2019 was the most difficult year for my family. Before we experienced the devastating cyclone Idai I and my family we used to grow crops and practice animal rearing and it would be enough to feed my children. My two children were in good health we rarely had cases of illness, in March 16, 2019 we were affected by cyclone Idai that had heavy rains and winds, which destroyed the fields, granaries, damage infrastructure which resulted in loss of livestock’s and human life. Few days after experiencing cyclone children started having diarrhea and signs of wasting would be observed this was in the first month before we had received any assistance. After one month we started receiving assistance in forms of water guard to treat water since most water sources had been destroyed. We also received assistance from Unicef, Ministry of Health and Child Care, WFP and Red cross as they introduced supplementary feeding program, where all children under five received Corn Soya Bland porridge and Tsabana porridge. We received vaccination against Cholera this targeted everyone. Programs that were done helped to reduce cases of diarrhea in children in our community. We received assistance for three months and with all the help I could see the restoration of my child’s health he started gaining weight and playing around with other kids”.
Program modifications
Table 1 below shows responses from key informant interviews of what was done on conventional IMAM against emergency. It shows that emergency IMAM reaches more children in the community than conventional.
| Emergency IMAM | |
|---|---|
| Targeted supplementary feeding | Blanket Supplementary feeding program |
| Dry feeding | Wet and Dry feeding |
| Treatment by case identification | Vaccination campaigns against cholera and rubella, total reach 16136 |
| Vitamin A supplementation done at clinic level | Mass Vit A Campaigns, total reach 37431 |
| Clinic level vaccinations | Community based mass vaccinations |
| MNPs distributed at clinic level | MNPs distribution at clinic and community level |
| Monthly screening of under-fives (total reach 8600) | Mass Active screening campaign was done, a total reach of 13845 children under the age of five were screened of acute malnutrition using the mid-upper arm circumference (MUAC) tape, which a coverage of 67%. |
Table 1: Program modifications to IMAM during emergency.
IMAM Indicators
Table 2 below shows a high cure rate between April and June, then a decrease in cure rate from July to September and improvement in cure rates from October to December for both clinics. There was also a significant increase in defaulter rate for Chimanimani Rural Hospital (10%) and Ngorima Clinic (44%) from July to September.
| Outcome indicator | April-June% | July-September% | October-December% | Average % | SPHERE % | |
|---|---|---|---|---|---|---|
| Ngorima Clinic | Cure rate | 80 | 56 | 100 | 79 | >75 |
| MAM admissions Chimanimani Rural Hospital | Death rate | 7 | 0 | 0 | 2 | <3 |
| MAM admissions Chimanimani Rural Hospital | Defaulter rate | 13 | 44 | 0 | 19 | <15 |
| MAM admissions Chimanimani Rural Hospital | Non recovery rate | 0 | 0 | 0 | 0 | <10 |
| MAM admissions Chimanimani Rural Hospital | Death rate | 0 | 0 | 0 | 0 | <3 |
| MAM admissions Chimanimani Rural Hospital | Cure rate | 79 | 80 | 86 | 82 | >75 |
| MAM admissions Chimanimani Rural Hospital | Defaulte rate | 16 | 10 | 14 | 13 | <15 |
| MAM admissions Chimanimani Rural Hospital | Non recovery rate | 5 | 10 | 0 | 5 | <10 |
Table 2: Health facility-based data for IMAM indicators per three months’ interval for MAM and SAM admissions at Ngorima clinic a
Trend in SAM and MAM Cases Post Cyclone
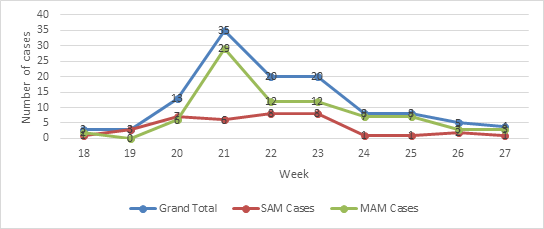
Figure 4 below shows an increase in MAM cases two months’ post cyclone an improvement in in the MAM cases 4 months post cyclone. There was also a slight increase in SAM cases 2 months’ post cyclone and then decreased 4 months post cyclone.
Programmes Initiated in Response to Cyclone Idai in Chimanimani
Vaccination campaigns, supplementary feeding programme, active screening campaigns, Vitamin A supplementation, distribution of micronutrient powders and village health worker capacity building were done.
Discussion
This study sought to evaluate the point prevalence of acute malnutrition and the post cyclone Idai IMAM response in Chimanimani district. It found that prevalence of SAM and MAM were highest early post cyclone. IMAM was able to reach 13845 children under five in Chimanimani, and treatment outcome indicators were above the sphere minimum standards except for defaulter rate. The IMAM programme contributed to significant changes to the health of the beneficiaries.
Impact of Cyclone Idai in Chimanimani District
A state of unusual, unforeseen and sudden events which requires immediate measures to reduce its adverse effects is called an emergency. Disaster this is the state of misfortune which affects the normal functioning of the community, resulting in loss of resources and displacement of families and affecting the ability to cope up using their resources [11]. The findings from this study revealed that there was destruction of fields, destruction of granaries, loss of livestock’s, loss of human life, destruction of water sources and destruction of infrastructure [12]. Which corresponds to a report done on Assessment of the Impact of Cyclone Eline in Zimbabwe on the Food, Agriculture and Natural Resource Sector in Zimbabwe? The results showed loss of crops by floods, increase in vegetable and food prices making affordability impossible, destruction of property (houses, bridges and toilets) and loss of granaries resulting to food stock losses and post-harvest losses and losses due to poor storage facilities [13].
Food insecurity leads to inadequate food intake and is linked to diseases. Normal biological processes of the body can be affected by poor food intake that it affects the general function of the organs in the body. The decrease in the normal functioning of the body leaves an individual more susceptible to the infectious diseases, due to weakened immune system. Diarrhea and vomiting reduce the bioavailability of nutrients due to the fact that food is not being adequately digested [14].
On a policy-making and implementation perspective, a new model is needed. The government of Zimbabwe is proposing an Integrated Emergency Operations Centre (IEOC) at national level, which suggests movement towards the necessary institutional development. This reform impetus triggered by the disaster is the basis for the following policy and programmatic considerations, which include a need for: Setting up social and child protection systems that are sensitive to disaster situations to take care of children and other vulnerable people, provision of shelter, and extending education and health assistance during and after disasters [15].
Nutrition Programmes Employed during Cyclone Idai - Nutrition Specific Programmes
Nutrition-specific interventions are simply defined as interventions done to address the immediate determinants of foetal, child nutrition and development. Nutrition-specific interventions include exclusive breastfeeding, Vitamin A supplementation, food fortification and dietary diversity promotion [16].
Just after the cyclone, blanket child supplementary feeding program was introduced. Wet feeding was introduced to children in camps and dry rations given to those in communities who had not been displaced. Monthly rations of corn soya blend were issued with assistance from WFP. The programme duration was 6 months [5]. A similar approach was used in five districts in Northern Kenya for four months, following a disaster were a blanket supplementary feeding programme was introduced which included monthly rations of oil and corn soya blend [17]. Vitamin A supplementation for children under five was also done for a period of 7 months. The supplementation was for all children under-five who were due and over-due for Vitamin A supplementation. Distribution of micronutrients powders (MNPs) was done by VHWs, at community level. MNPs and Vitamin A supplementation played a major role in zero reports in affected areas on micronutrient deficiency symptoms for children under-five’ [18]. A similar approach was used in Bangladesh were micronutrient powders were used as food supplements. The prevalence in stunting was low among the group that consumed at least 75% of MNPs sachet in comparison to those that consumed less [19].
The quality and quantity of food consumed are vital aspects, in terms of nutritional intake as it affects development and growth amongst children under-five [20]. After earthquakes experienced in July 2019 in kern and Bernardino counte California, which damaged roadways, commercial structure, and homes school feeding program for lunch and breakfast were put in place to reduce the incidence of malnutrition. Supplemental Nutrition Assistance Program (SNAP) was put in place it allowed households in affected areas to request replacements of SNAP benefits. These meant that food lost because of earthquake and aftershock were replaced through replacements of SNAP benefits [21]. The research reviewed similar strategies as those used in Chimanimani. Both methods helped to improve the nutrition status of children under five in the respected areas.
Nutrition Sensitive Programmes
Nutrition-sensitive interventions these are interventions that has an influence on the underlying determinants of nutrition [22]. During the emergency period vaccination campaigns against cholera, deworming and active screening campaigns, where early case finding of malnutrition cases were done. These interventions lasted for 6 months and there had a great impact as zero cases of cholera were recorded after the interventions [5]. A similar approach was used in Vanuatu Islands after been affected by cyclone Pam. They managed to do distributions of diarrheal disease treatment kits and purification tablets for water, deworming treatment and measles vaccination campaigns were done targeting the under 5. One month after the interventions were done those that were affected by cyclone Pam still faced challenges that were life-threatening due to the lack of continued supply of safe water, food and growing outbreaks of diseases [23]. The affected groups in Chimanimani district require support from policy makers to collaboratively come up with policies that helps with continuing supply of assistance until the area have fully recover from the disaster to prevent outbreaks of disease.
Modifications to IMAM Programme
Modifications to the generic IMAM programme included, blanket feeding of all children under five and inclusion of pregnant, lactating women. The IMAM programme was integrated with mass vaccination campaign against cholera, construction of new safe water sources and distribution of water guard. Majority of the mothers interviewed through MSCs and FDGs reported that early post cyclone most of the children suffered from diarrhoea. The mothers revealed that they were drinking water from unprotected water sources, and using bush toilet system due to destruction of infrastructure. Destruction of infrastructure led to poor sanitation practices hence diarrhoea cases increased, late post cyclone after interventions of vaccinations, distributions of water guard tablets and building of safe water sources had been implemented the cases dropped. These modifications concur with similar case of Cyclone Pam in Vanuatu were diarrhoea disease treatment kits, and 190 000 water purification tablets were distributed and it improved the situation [23].
IMAM is a program designed to address acute malnutrition. The aim of the IMAM program is to integrate management of acute malnutrition into the on-going routine health services [24]. The integration of IMAM programme and mass vaccination campaign against cholera, construction of new safer water and distribution of water guard had a great impact on IMAM Indicators outcome. The number of MAM cases decreased during early post cyclone to late post cyclone. Integration allowed health workers to continue monitoring and evaluation of the IMAM programme, hence it led to decrease in MAM and SAM cases and there was sustainability. This agrees to a study on nutrition interventions for children less than 5 years following natural disasters, were the author noted that sustainability in long run can be achieved if interventions are integrated with health promotion activities and community mobilization [19]. Another study done in India have shown that integrating CMAM initiatives with water, sanitation and hygiene (WASH) programmes will provide a thorough approach to problems of malnutrition. In the study, states with over 80% access to toilets, recorded the lowest levels of child malnutrition in comparison with states with little access to toilets they recorded high rates of child malnutrition [25]. Modification of IMAM programme ensured that both mothers and child receive adequate food to reduce malnutrition. Vaccination against cholera and distribution of water guard tablets reduced cases of diarrhoea hence improving health of the beneficiaries.
Challenges in Programming
Amid a disaster it is very difficult to begin creating coordination from the start example developing nutrition tools, identifying stakeholders and assigning responsibilities and roles among stakeholders. Any delay results in more human suffering as well as costs. Therefore, it is more cost effective to raise the minimum programmatic and coordinating capacity to address the more regular development issues, which can then be more easily scaled- up at times of emergency. The key to preparedness actions involves the establishment of an integrated and functional coordination mechanism at all levels that’s the sub-national and national level, and the development of a nutrition response plan in emergency situations [26].
In early post cyclone number of MAM cases had occurred raised to 49 this can be attributed to that; the rivers were flooded, and bridges were damaged which prevented caregivers from reaching to the nearest clinic for assistance. Lack of preparedness when the district was affected by cyclone Idai that’s they lacked required nutritional commodities to address different nutritional needs. Example some health facilities were out of stock in terms of nutrition commodities such as RUSF and RUTF to help undernourished children.
IMAM Outcomes
Through integration with other programs active screening campaigns were conducted children under-five were checked for malnutrition using MUAC and oedema check. All malnourished children were admitted at UNICEF- supported OTP and the performance of the OTP was within the SPHERE standards except for defaulter rate. In an effort to reduce defaulter rate, Nutrition ward coordinators worked closely with VHWs to ensure all of the children under-five admitted in OTP receive home visits [18]. Children were screened for malnutrition at food distribution site, camps and health facilities and those due or overdue for vitamin A supplementation would receive their dose [27]. This made the IMAM programme effective in trying to reach all children within the district.
The average defaulter rate from April to December for Ngorima clinic was 19% which is above the SPHERE standard that states that defaulter rate (<15%) is considered acceptable levels of performance [28]. The higher number in defaulter rate from MSCs was reported by mothers interviewed to be as a result of destruction of bridges and roads which made it difficult to access health facilities and another issue was migration in search for food. Through the FDGs it was reported that there was poor distribution of food commodities in other sites which might have force other mothers to migrate to places where they could find food. Programme evaluation report in South Sudan on outpatients it reported that defaulter rate of 15% was observed as a result of heavy rains which had damaged infrastructure making mother and child to walk long hours to health [29]. Similar results were also observed on a programme evaluation report in Afghanistan on outpatient SAM treatment intervention, were 23.8% defaulter rate was observed which was relatively high compared to the SPHERE standards based on interviews conducted with mothers they reported that at centres there was insufficient food distribution and illness of mother resulted at 23.8% [30].
Conclusion and Recommendations
Conclusions
There was an increase in MAM cases just after the disaster which decreased after the first initial response and few SAM cases were recorded in Chimanimani two months after the disaster. The interventions done in Chimanimani district targeting children under the age of five addressed most of the needs following a disaster. The study also established lack of emergence preparedness as the response to the disaster took a lot of time and clinics were out of stock in terms of nutrition commodities prior to the disaster. The IMAM program and supplementary feeding program were both a success however there is need to increase supplementary feeding program time line as it was done only for six months this would help to address issues of stunting and some families are still household insecure. Developmental nutrition would now help to address issues of malnutrition in Chimanimani district as their past the recovery phase where they were relying on food aid. There is now need for long term sustainable projects such as sustainable agriculture.
Recommendations
1) There is need for trainings in developmental nutrition, emergence nutrition and disaster preparedness by MOHCC [5]. 2) There is need for further study and comparison with other affected districts for future. 3) Cyclone Eline was experienced in the region in 2000 and lack of documentation and research on the outcomes and interventions affected cyclone post response therefore there is need for proper documentation of outcomes and interventions. 4) The MoHCC need to make sure all health facilities are always adequately stocked with nutrition commodities.
Disclosure of Potential Conflicts of Interest
We declare that there is no conflict of interest
Acknowledgements
The authors would like to extend great appreciation to MoHCC Chimanimani district staff, Shylet Jonga and Mr Simon Kiarie Karanja for technical support which made this research possible.
References
-
Kouadio IK, Aljunid S, Kamigaki T, Hammad K (2014) Prevention and control measures Infectious diseases following natural disasters. Expert Review of Anti- infective Therapy 10(1): 95-104.
-
FAO, IFAD, UNICEF (2018) The state of food security and nutrition in the world, Rome, Italy, pp: 25
-
Geographic N (2015) El Niño _ National Geographic Society, USA.
-
UNDP (2017) El Niño-Southern Oscillation (ENSO) cycle events and their impacts in Zimbabwe. Zimbabwe Resilience Building Fund, Harare.
-
MoHCC, WHO, (2019) Situation report on cyclone idai issue 0015.
-
O’Connor M, Burkle F, Olness K (2016) Infant feeding practices in complex emergencies: A case study approach. Prehospital and Disaster Medicine: A case study approach. Prehospital and Disaster Medicine16(4): 231-238.
-
WHO, UNHCR, UNICEF (2004) Food and Nutrition Needs Food. First Edition. Geneva, pp: 5
-
Food and Nutrition Council (2018) Zimbabwe National Nutrition Survey Report.
-
Onis O, Arimond M, Webb P, Croft T, Saha K, et al. (2018) Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutrition 21(1): 175-179.
-
ZIMSTAT, UNFPA (2020). Manicaland province district population projections report. Harare.
-
International ACF (2012) Emergency nutrition- A handbook for developing an emergency nutrition intervention strategy. Action Contre La Faim, Paris, pp: 25-30.
-
GFDRR, World Bank (2019) Zimbabwe rapid impact and needs assesement (RINA).
-
Agritex, USAID, FAO, WFP (2000) Assessment of the impact of cyclone Eline (February 2000) on the Food, Agriculture and Natural Resource Sector in Zimbabwe.
-
Schmidt CW (2014) Beyond Malnutrition the role of sanitation in stunted growth. Environmental Health Perspectives 122(11): 298-303.
-
Chatiza K (2019) Cyclone Idai in Zimbabwe -An analysis of policy implications for post-disaster institutional development to strengthen disaster risk management.
-
IFPRI 2016 Global Nutrition Report (2016) From Promise to Impact: Ending Malnutrition by 2030. Washington, DC.
-
Hall A, Maragwo O, Victoria S, Ndumi A (2011) The Practical Challenges of Evaluating a Blanket Emergency Feeding Programme in Northern Kenya. PLoS ONE 6(10): 5-7.
-
UNICEF (2019) Cyclone Idai Zimbabwe Humanitarian Situation Report No 2.
-
Pranil MSP, Dhital R, Subhani H (2016) Nutrition interventions for children aged less than 5 years following natural disasters : a systematic review. BMJ Open 6: e011238.
-
Fenn B (2014) Malnutrition in Humanitarian Emergencies. London school of hygiene and tropical medicine, pp: 4.
-
USDA (2019) California Disaster Nutrition Assistance _ USDA-FNS. Available at: California Disaster Nutrition Assistance _ USDA-FNS.html.
-
Marie Ruel, Harold Alderman, and the Maternal and Child Nutrition Study Group (2013) Maternal and Child Nutrition 3 Nutrition-sensitive interventions and programmes : how can they help to accelerate progress in improving maternal and child nutrition.
-
WHO (2015) WPRO_ A month after Cyclone Pam, Vanuatu continues to face health challenges, Port Vila.
-
The Republic of Uganda MoH (2010) Integrated Management of Acute Malnutrition Guidelines. Uganda, pp: 2-237.
-
AIDF (2015) Meeting the Nutrition Needs of Children in Disaster and Development _ Food Security.
-
Macias YF (2019) Nutrition coordination mechanisms : the whats , whys and wherefores. Nutrition exchange.
-
UNICEF (2020) Cyclone Idai Zimbabwe Humatarian Situation Report No 8.
-
Team ANC Coor-dination and PND/MoPH (2019) Afghanistan Nutrition cluster Annual Report.
-
Akparibo R, Booth A, Lee A (2017) Recovery, relapse and episodes of default in the management of acute malnutrition in children humanitarian emergencies:A systematic review.
-
Qarizada NA, Mustaphi P, Oketch A, Jecinter, Safi S (2018) Scale- up of IMAM service in Afghanistan.
- Lessons to Learn: Trees are More than the Lungs of the World
- Community Forestry Enterprises as a Model for Sustainable Forest Development: The Case Of The "Baja Tarahumara" in Chihuahua, Mexico
- Ecological and Socio-Economic Impacts of Chromolaena odorata and Mesosphaerum suaveolens, Two Invasive Alien Species in Central and Southern Benin, West Africa
- Epigenetic Sustainability: Modeling the Human Factor as a Natural Resource through Science 4.0 and the NR3C1 Biological Pilot
- Growth-at-Risk: A Framework for Assessing Economic Vulnerability
- The Rural Territory as a Socioecological System for the Management of Public Policy for Sustainable Rural Development