Long Term Results of Stem Cell Therapy in Patients with Peripheral Arterial Disease (PAD)
Peripheral Arterial Disease (PAD) is still a challenging condition affecting millions of people and leading to amputation or death. In patients with non reconstructable disease or failed revascularization, stem cell therapy (SCT) could help in promoting angiogenesis and limb salvage. However, there is limited data about the long-term benefits of SCT in such patients. Aim of this study is to evaluate the long-term survival and clinical outcomes in PAD patients who underwent stem cell therapy. All patients who underwent stem cell therapy using intramuscular injections of autologous bone-marrow mononuclear cells (BM-MNCs) for the treatment of PAD between January 2011 and November 2020 were include in the study. Electronic medical records (EMRs) and Telephonic phone follow up was used to get baseline clinical characteristics and follow up data. Out of 3627 PAD patient, 41 patients underwent stem cell therapy procedure between January 2011 to November 2020. Mean age was 48 years (range, 21 to 75 years) and 37 patients (90.24%) were males. The median follow-up period was 4.66 years (range, 6 months – 9.9 years). Indication for SCT was rest pain, gangrene or non-healing ulcer due to either non reconstructable disease or failed revascularization. All patients were given antiplatelets and statin therapy. Out of 41 PAD patients, 7 patients were lost to follow up. In the remaining, 34 patients, 29 (70.73%) patients were alive, and 5 patients were dead. Overall, 10 (24.39%) patients underwent ipsilateral amputation and 4 patients had persistent claudication pain. In the remaining patients’ ulcers healed and has no residual pain. Amputation free survival was 75.61%. The benefits of Autologous BM-MNCs stem cell therapy are sustained even in the long term with overall survival rate was 85.29% and the amputation free survival was 75.61% and should be considered for all CLI patients irrespective of age.
Kereena Chukka1*, Prem Chand Gupta1, Vamsikrishna Yerramsetty1, Sudheer Volluri2 and Gnaneswar Atturu1
Keywords: Peripheral Arterial Disease (PAD); Critical Limb Ischemia (CLI); Stem Cell Therapy
Introduction
Peripheral Arterial Disease (PAD) is still a challenging condition affecting millions of people worldwide, leading to amputation or death. The number of PAD patients has increased by nearly a quarter in the past decade. It’s
become a major public health challenge associated with immobility, decline functionally, cardiovascular, and adverse limb events [1, 2]. Most of the PAD cases are asymptomatic; about a quarter of PAD patients present with intermittent claudication (IC), progress to critical limb ischemia (CLI) with rest pain and gangrene leading to amputation. Due to the advancement of PAD disruption of blood supply occurs from several weeks to months [3]. For PAD patients, Risk factor control, antiplatelet and statin drugs and excersie training [4, 5, 6, 7] are the common conventional treatments at an early stage. But the Reconstruction of the blood circulation using endovascular or open surgical approaches will be required in more advanced stages of PAD [8, 9]. Prognosis of the disease is very poor at 5-year survival rate; it’s about less than 50%. Amputation is the last choice when both surgery and interventional therapy is not possible. Amputation has about 25~50% of mortality rate of which 5~20% in perioperational period, and the re-amputation rate is up to 30% [10].
In spite of all the treatments certain group of patients will not have any further viable options requiring limb amputation (No option PAD/CLI). Novel and more effective methods including stem cell therapy (SCT) have emerged as a promising alternative for treatment of disorders related to limb ischemia Schiavetta A, et al. [11], Wang ZX, et al. [12] Stem cell therapy (SCT) could help in promoting angiogenesis and limb salvage. However, there is limited data about the long-term benefits of SCT in such patients. Therefore, this study was conducted to evaluate the long-term survival and clinical outcomes in PAD patients who underwent stem cell therapy.
Methods
Study Population and Data Collection
Prospectively collected clinical data was retrospectively analyzed. All patients who underwent stem cell therapy using intramuscular injections of autologous BM-MNCs for the treatment of PAD between January 2011 and November 2020 were included in the study. Electronic medical records (EMRs) and Telephonic phone follow up was used to get baseline demographic, clinical characteristics and follow up features of the treated limb were reviewed. The clinical outcome measures including the rate of freedom from major amputations of the treated limb, major adverse events, all-cause mortality, and the ulcer healing rate were also reviewed. Major amputation was defined as amputations proximal to ankle. Inclusion criteria: CLI patients with rest pain, gangrene or non-healing ulcer due to either non reconstructable disease or failed revascularization who had received BM-MNCs SCT were included in the study.
Exclusion criteria: Estimated survival less than 6 weeks, known bone marrow disease patients, CKD patients on dialysis were excluded in the study.
BM MNC Harvesting and Implantation
BM-MNCs were harvesting and implanted in PAD patients using a standard protocol. In brief, 300 to 300ml of bone marrow was aspirated from the right iliac bone of the patient under general anesthesia and BM-MNCs were immediately isolated using a CS3000-Plus blood-cell separator (Baxter, Deerfeld, IL) to obtain a final volume of 50 mL approximately. One mL of BM-MNCs was implanted intramuscularly into each of a total of 40 sites with a 3×3-cm grid using a 22-gauge needle at a depth of 1.5 cm into the Calf of the ischemic leg.
Statistical Analysis
The data was collected using a standard proforma in excel sheet for analysis. Statistical analysis using descriptive statistics was performed with SPSS software version 24.0 for Windows (SPSS Inc., CR). Categorical variables were reported as percentages and/or frequencies, and continuous variables as ranges.
Results
Baseline Characteristics
Table 1 shows the baseline characteristics of patients who underwent BM-MNCs SCT. Out of 3627 PAD patient, 41 patients underwent BM-MNCs SCT procedure between January 2011 to November 2020. Mean age was 48 years (range, 21 to 75 years), 37 patients (90.24%) were males, 39.02% patients were former smokers and 17.07% of the cases were active smokers. Average BMI was 25.58 (range between 15.57 to 40.45). The median follow-up period was 4.66 years (range, 6 months – 9.9 years). Indication for SCT in all patients was critical limb ischemia (Rest pain, gangrene or non-healing ulcer) with either non reconstructable disease or failed revascularization. 10 (24.39%) patients were on antiplatelet therapy alone, 20 (48.78%) patients were on both antiplatelet and anticoagulation, and 11 (26.82%) patients were on antiplatelet and statins. 29 out of 41 patients had one or more revascularization procedures before SCT. Out of 41 PAD patients, 7 patients were lost to follow up. In the remaining, 34 patients, 29 (70.73) patients were alive, and 5 patients were dead due to myocardial infraction, stroke and other cardiac related issues. 10 (24.39%) patients underwent ipsilateral amputation resulting in an amputation free survival rate of 75.61%. 4 patients had residual pain requiring regular analgesia. In the remaining patients’ ulcers have healed and has no significant pain. The follow up results with timelines was shown in Figure 1.
| Characteristics | Total number (percentage) |
| Mean Age in years | 48 years (range, 21 to 75 years) |
| Male | 37 (90.24) |
| Average BMI (kg/m2) | 25.58 |
| Comorbidities | |
|---|---|
| Smoking | |
| Active smokers | 7 (17.07) |
| Former smokers | 16 (39.02) |
| Non-smokers | 16 (39.02) |
| Habit of chewing Paan/Gutka | 2 (4.87) |
| Hypertension (HTN) | 2 (4.87) |
| Type II diabetes mellitus (T2 DM) | 2 (4.87) |
| Coronary artery disease (CAD) | 1 (2.43) |
| Multiple comorbidities (combination of two or more diseases including HTN/CAD/DM/DVT/CKD/COPD) | 17 (41.46) |
| Nil | 18 (43.90) |
| Treated Limb | |
| Right | 18 (43.90) |
| Left | 22 (53.65) |
| Bilateral | 1 (2.43) |
| Number of major Amputations to the involved limb after SCT | 10 (24.39) |
| Medical history | |
| On antiplatelet therapy alone | 10 (24.39) |
| On both antiplatelet and anticoagulation | 20 (48.78) |
| On antiplatelet and statins | 11 (26.82) |
| Surgical History | |
| Bypass | 6 (14.63) |
| Stenting | 1 (2.43) |
| Sympathectomy | 1 (2.43) |
| Surgical thrombectomy | 4 (9.75) |
| Total available patients for follow-up | 34 (82.92) |
| Lost to Follow-up | 7 (17.07) |
| Alive | 29 (70.73) |
| Death | 5 (12.19) |
Table 1: Baseline Characteristics of SCT patients (n=41).
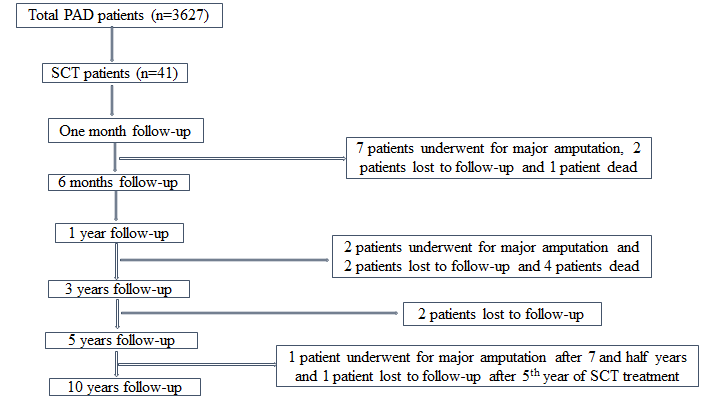
Figure1: Flow-Chart of Patients Follow-up Information.
Discussion
The results of this study with follow up extending up to 10 years, confirms the beneficial role of SCT in patients with failed or non reconstructable peripheral arterial disease. Currently, SCT is being used to improve clinical symptoms and preserve the limb viability of PAD patients who have no option other than amputation [13]. Stem cell therapy for limb ischemia was introduced in early 2000. Tateishi-Yuyama E, et al [14] reported the efficacy of intramuscular implantation of autologous BM-MNCs in patients with critical limb ischemia (CLI) in 2002. They found that SCT increased collateral vessel formation leading to improvement in ischemic symptoms. Since then, many studies reported the benefits of harvesting stem cells from different sources and administering locally using different regimens for no-option PAD patients.
Several studies have clearly shown that the SCT of autologous BM-MNCs implantation improves clinical symptoms and major amputation-free survival rate in PAD patients [14, 15, 16]. The Therapeutic Angiogenesis by Cell Transplantation (TACT) trial showed that SCT of BM- MNCs leads to extension of the amputation-free period, improvement in pain while walking and ulcer size Tateishi- Yuyama E, et al. [14], Matoba S, et al. [15] studied the clinical characteristics of PAD patients who underwent BM-MNCs implantation and reported that at 3 year follow up survival rate was 80% and amputation free rate was 60%. Yusoff, et al. [16] found that, in 10 years follow up amputation free rate was 70.4%, and survival rate was 50.2% respectively. In our study the major amputation-free survival rate is 75.61% and higher compared to other studies.
In contrast to the above studies, Rigato M & Kondo K, et al. [17, 18] studies reported that SCT using BM-MNCs does not alter the mortality rate of patients with PAD. This difference in outcomes between studies could be due to variations in protocols for harvesting and implanting SCTs in trials [19, 20, 21, 22, 23, 24]. Some of the limitations of this study include being a retrospective observational study, single center experience and relatively small number of patients (n=41). Also, it was not possible to gather information regarding the quantity and quality of BM-MNCs implantation (cells per ml).
Conclusion
PAD patients who underwent SCT had a 75.61% amputation free survival and an overall survival rate of 85.92%. The present study has shown that SCT using autologous BM-MNC has the potential to modify the natural history of intractable PAD and should be considered in all patients irrespective of age.
References
-
Fowkes FG, Diana Rudan, Igor Rudan, Victor Aboyans, Julie O Denenberg, et al. (2013) Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet 382(9901): 1329-1340.
-
Higashi Y, Tetsuro Miyata, Hiroshi Shigematsu, Hideki Origasa, Masatoshi Fujita, et al. (2017) Two-year follow-up of vascular events in peripheral arterial disease treated with antiplatelet agents: a prospective observational multicenter cohort study (SEASON). Sci Rep 7(1): 6095.
-
Kinlay S (2016) Management of critical limb ischemia. Circ Cardiovasc Interv 9(2): e001946.
-
Steffen LM, Duprez DA, Boucher JL, Ershow AG, Hirsch AT, et al. (2008) Management of peripheral arterial disease. Diabetes Spectr 21(3): 171-177.
-
Fokkenrood HJ, Bendermacher BL, Lauret GJ, Willigendael EM, Prins MH, et al. (2013) Supervised exercise therapy versus non-supervised exercise therapy for intermittent claudication. Cochrane Database Syst Rev 23(8): CD005263.
-
Robertson L, Andras A (2013) Prostanoids for intermittent claudication. Cochrane Database Syst Rev 30(4): CD000986.
-
Adam DJ, Beard JD, Cleveland T, Bell J, Bradbury AW, et al. (2005) Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Te Lancet 366(9501): 1925-1934.
-
Bradbury AW, Adam DJ, Bell J, Forbes JF, Fowkes FG, et al. (2010) Bypass versus angioplasty in severe ischaemia of the leg (BASIL): multicentre, randomised controlled trial. Health Technol Assess. 14(14): 1-210.
-
Frangogiannis NG (2018) Cell therapy for peripheral artery disease. Curr Opin Pharmacol 39: 27-34.
-
Sprengers RW, Moll FL, Verhaar MC (2010) Stem cell therapy in PAD. Eur J Vasc Endovasc Surg 39(S1): S38-S43.
-
Schiavetta A, Maione C, Botti C, Gennaro Marino, Stefano Lillo, et al. (2012) A phase II trial of autologous transplantation of bone marrow stem cells for critical limb ischemia: results of the Naples and Pietra Ligure evaluation of stem cells study. Stem Cells Transl Med 1(7): 572-578.
-
Wang ZX, Li D, Cao JX, Yi-Shan Liu, Min Wang, et al. (2014) Efficacy of autologous bone marrow mononuclear cell therapy in patients with peripheral arterial disease. J Atheroscler Thromb 21(11): 1183-1196.
-
Higashi Y, Murohara T (2017) Terapeutics angiogenesis. Cardiology & Angiology, Springer Nature, Berlin.
-
Tateishi-Yuyama E, Hiroaki Matsubara, Toyoaki Murohara, Uichi Ikeda, Satoshi Shintani, et al. (2002) Terapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: a pilot study and a randomized controlled trial. Te Lancet 360(9331): 427-435.
-
Matoba S, Tetsuya Tatsumi, Toyoaki Murohara, Tsutomu Imaizumi, Yousuke Katsuda, et al. (2008) Long-term clinical outcome afer intramuscular implantation of bone marrow mononuclear cells (Terapeutic Angiogenesis by Cell Transplantation [TACT] trial) in patients with chronic limb ischemia. Am Heart J 156(15): 1010-1018.
-
Yusof FM, Masato Kajikawa, Shogo Matsui, Haruki Hashimoto, Shinji Kishimoto, et al. (2019) Review of the long-term efects of autologous bone-marrow mononuclear cell implantation on clinical outcomes in patients with critical limb ischemia. Sci Rep 9(1): 7711.
-
Rigato M, Monami M, Fadini GP (2017) Autologous cell therapy for peripheral arterial disease: systematic review and meta-analysis of randomized, nonrandomized, and noncontrolled studies. Circ Res 120(8): 1326-1340.
-
Kondo K, Kenji Yanishi, Ryo Hayashida, Satoshi Shintani, Rei Shibata, et al. (2018) Long-term clinical outcomes survey of bone marrow-derived cell therapy in critical limb ischemia in Japan Circ J 82(4): 1168-1178.
-
Fadini GP, Agostini C, Avogaro A (2010) Autologous stem cell therapy for peripheral arterial disease meta-analysis and systematic review of the literature. Atherosclerosis 209(1): 10-17.
-
Ozturk A, Yasar Kucukardali, Fatih Tangi, Alev Erikci, Gunalp Uzun, et al. (2012) Terapeutical potential of autologous peripheral blood mononuclear cell transplantation in patients with type 2 diabetic critical limb ischemia. J Diabetes Complications 26(1): 29-33.
-
Samura M, Tohru Hosoyama, Yuriko Takeuchi, Koji Ueno, Noriyasu Morikage, et al. (2017) Terapeutic strategies for cell-based neovascularization in critical limb ischemia. J Transl Med 15: 49.
-
Peeters Weem SM, Teraa M, de Borst GJ, Verhaar MC, Moll FL, et al. (2015) Bone marrow derived cell therapy in critical limb ischemia: A Meta-analysis of Randomized Placebo Controlled Trials. Eur J Vasc Endovasc Surg 50(6): 775-783.
-
Pignon B, Marie-Antoinette Sevestre, Lukshe Kanagaratnam, Gilles Pernod, Dominique Stephan, et al. (2017) Autologous bone marrow mononuclear cell implantation and its impact on the outcome of patients with critical limb ischemia: results of a randomized, double-blind, placebo-controlled trial. Circ J 81(11): 1713-1720.
-
Dong Z, Tianyue Pan, Yuan Fang, Zheng Wei, Shiyang Gu, et al. (2018) Purifed CD34+ cells versus peripheral blood mononuclear cells in the treatment of angiitis-induced no-option critical limb ischaemia: 12-Month results of a prospective randomised single-blinded non-inferiority trial. EBioMedicine 35: 46-57.
-
Gao Wei, Dawei Chen, Guanjian Liu, Xingwu Ran (2019) Autologous stem cell therapy for peripheral arterial disease: a systematic review and meta-analysis of randomized controlled trials. Stem Cell Research & Therapy 10(140): 12-14.
- Research Progress of Induced Pluripotent Stem Cells and Their Clinical Application Prospects
- Nishan Al-Kamal is the Starting Point of A Feminist Scientist
- Current Concepts and Future Perspectives of Stem Cell Therapy in Peripheral Arterial Disease
- Stem Cell and Oxidative Stress-Inflammation Cycle
- Adipose Derived Mesenchymal Stem Cells Origin, Characteristics and Promises
- Mitochondria Targeted Antioxidants can Improve In Vitro Embryo Production in Buffalo