Morphometric Study of the Vertebral Body and Pedicle of Typical Cervical Vertebrae Using Radiological Image
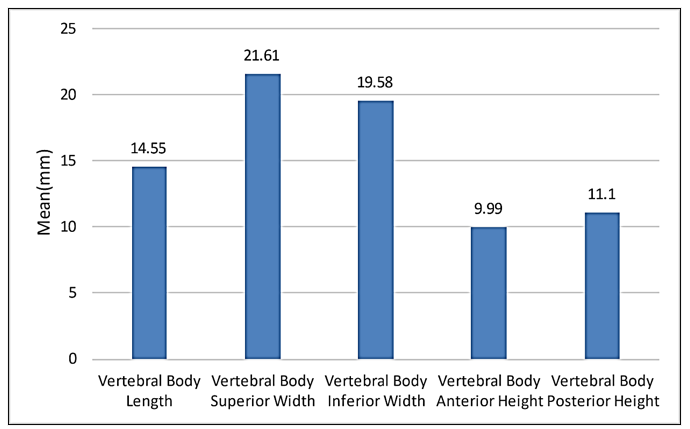
Introduction: Accurate knowledge of cervical vertebral body dimensions is essential for effective diagnosis and treatment of cervical spine disorders. The anteroposterior diameter is a critical measurement for anterior bicortical screw fixation. Vertebral osteophytes, commonly seen on the anterolateral margins of the lower cervical vertebrae, are age-related degenerative changes that may cause neurovascular compression. Large osteophytes can compress the vertebral artery as it crosses the uncinate process, potentially resulting in dysphagia, sleep apnea, or spinal nerve root compression.Objectives: To assess the morphometric dimensions of the vertebral body and pedicle in typical cervical vertebrae and toobserve the presence of osteophytes.Materials and Methods: This study was conducted on 100 dry human typical cervical vertebrae of unknown age and sex.Morphometric parameters of the vertebral body and pedicle were measured using a digital vernier calliper in millimeters.Measurements included anteroposterior and transverse dimensions.Results: The average vertebral body length was 14.55 ± 2.14 mm; anterior height 9.99 ± 1.35 mm; posterior height 11.1 ±1.4 mm; superior width 21.61 ± 2.81 mm; and inferior width 19.58 ± 3.2 mm. Pedicle length and height were statisticallysignificant, whereas pedicle width was not. Osteophytes were observed on the vertebral bodies.Conclusion: Morphometric data are valuable for surgical planning in anterior cervical reconstruction and enhance the safetyof transpedicular screw insertion. These findings also have relevance in anthropological research.
Abbreviations
CPS: Cervical Pedicle Screw; VBL: Vertebral Body Length; VBSW: Vertebral Body Superior Width; VBIW: Vertebral Body Inferior Width; VBAH: Vertebral Body Anterior Height; PL: Pedicle Length.
Introduction
The body of cervical vertebrae plays a vital role in managing and treating diseases related to the cervical vertebral column by knowing the accurate dimensions. Anteroposterior diameter is a crucial measurement for anterior biocritical screw fixation [1]. Vertebral osteophytes are age-related degenerative changes in the vertebral body [2] typically seen on the anterolateral margins of the lower cervical vertebrae [3, 4]. Increased body mass and intense activity, particularly in men, can lead to intervertebral disc degeneration and osteophyte development [2]. The high compressive load-bearing has been linked to the development of spinal osteophytes [4]. Age-related degenerative alterations in the spine lead to vertebral osteophytes [2]. It frequently appears on the lower cervical vertebrae’s anterolateral margins [3]. The oesophageal segment gets compressed at C5/C6 on the cricoid cartilage due to tiny osteophytes [5]. The vertebral artery passes over the vertebral uncinate process due to large osteophytes, which can cause sleep apnea and dysphagia [6]. Anatomists and physicians are commonly aware of osteophytes in the vertebral column. Except for the seventh, which had them on its superior border, the maximum frequency was discovered on the sixth typical cervical vertebrae. They are typically found on the other vertebrae’s inferior border [3, 4].
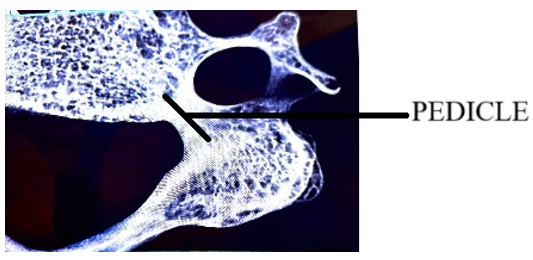
The pedicles are short, cylindrical projections that extend backward from the body and meet the lamina posteriorly. The spinal nerves pass via the intervertebral foramina, which are formed by the intervertebral notch on the superior and inferior aspects of the pedicle. The precise dimensions of the pedicles—both in length and width— are vital for selecting the appropriate screw size during surgical procedures like transpedicular fixation. If these dimensions are not accurately known, there is an increased risk of damaging neurovascular structures during surgery [7]. Additionally, osteophytes can cause narrowing of the vertebral canal, leading to compression of the spinal nerve roots as they pass through the pedicles. This compression can result in neurological symptoms [8, 9]. In the posterior cervical treatments such as general localization, cervical pedicle screw (CPS) fixation, and neve root decompression utilizing foraminotomy, it is essential to comprehend pedicle morphology. Knowledge of the shape of the cervical pedicles is crucial to preventing injury to the spine, nerve root, or vertebral artery, during surgery on the cervical posterior region.
There have been reports of variations in cervical spine morphometries among various ethnic and demographic groupings. These variations impact the surgical procedure to prevent pedicle breach and other issues. The surgical method for repairing the cervical pedicle screws will therefore be facilitated by knowledge of the anatomy of the cervical pedicles [10]. Understanding the morphometry of the vertebral body and pedicle is imperative to diagnosing diseases such as cervical canal stenosis or spinal cord tumors [11], figuring out the pathogenic abnormalities in the cervical spine, and identifying the typical reasons why changes in the cervical spine cause headaches and pain in the neck, chest, shoulder, arm, and other regions [12].
Materials and Methods
Sample Selection
A total of 100 dry, normal cervical vertebrae from the Department of Anatomy were used in the study. The vertebrae used in the study were part of a larger collection of cadaveric specimens, for which ethical approval was obtained from the institution’s ethics review board. The specimens included cervical vertebrae from individuals of varied age groups, with the primary inclusion criteria being that the vertebrae were well-preserved and free from significant pathological changes such as fractures or severe osteophyte formation. Vertebrae from C3 to C6 levels were included, as these levels are most commonly involved in clinical procedures such as screw fixation and decompression surgeries.
Measurement Procedure: Morphometric dimensions were carefully measured using a digital vernier caliper (accuracy: 0.01 mm) to ensure precision in each measurement. Both the superior and inferior aspects of the vertebral body and pedicles were measured.
Vertebral Body Measurements:
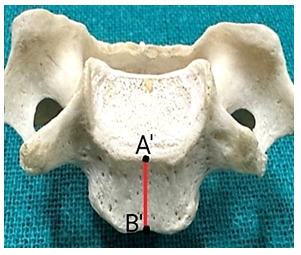
- Length: The length of the vertebral body was measured from the anterior to the posterior aspect, ensuring that the measuring line passed through the midline of the vertebral body.
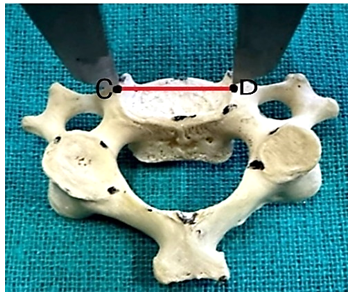
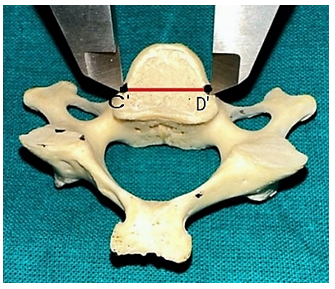
- Width: The superior and inferior aspects of the vertebral body were used to measure the width of the body.
- Height: The vertebral body height was measured at both the anterior and posterior aspects of the body from the inferior edge to the superior edge.
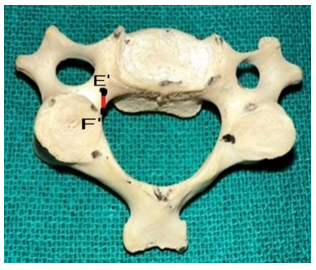
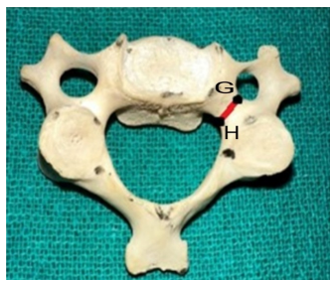
- 2. Pedicle Measurements:
- Length: The pedicle length was measured from the outer edge of the vertebral body to the point where the pedicle meets the lamina, both on the right and left sides.
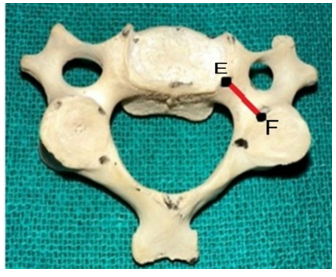
- Height: The height of the pedicle was measured from the superior to the inferior margin.
- Width: The width of the Right and Left pedicles was measured at the level of the vertebral body.
Radiological Imaging: Radiological images (X-rays) were taken of a subset of 20 vertebrae to support the morphometric data and to ensure the accuracy of the physical measurements. These radiological images were also used to examine the presence and size of osteophytes in the cervical vertebrae, providing insight into degenerative changes that may be associated with these morphological features.
Statistical Analysis: Data analysis was performed using SPSS version 23.0. Descriptive statistics, including means and standard deviations (mean ± SD), were calculated for all morphometric parameters. One-sample t-tests were used to compare the current study’s measurements with those reported in previous literature. Paired-samples t-tests were conducted to assess differences between the right and left sides of the pedicle measurements. A p-value of less than 0.05 was considered statistically significant.
Inclusion and Exclusion Criteria Inclusion Criteria:
- Well-preserved, dry, typical cervical vertebrae (C3 to C6) with no severe deformities, fractures, or pathological conditions.
- Specimens with no visible osteophyte formation or only minimal, non-disruptive osteophyte growth.
Exclusion Criteria:
- Vertebrae with significant osteophyte formation affecting the pedicles or vertebral body.
- Specimens showing obvious deformities or fractures that could affect the accuracy of the measurements (Figures 1-8).

- Results
- Vertebral Body
- Descriptive statistics were calculated for the length, width, and height of the vertebral body. The mean vertebral body length was 14.55 ± 2.14 mm (range: 10.24–21.67 mm).
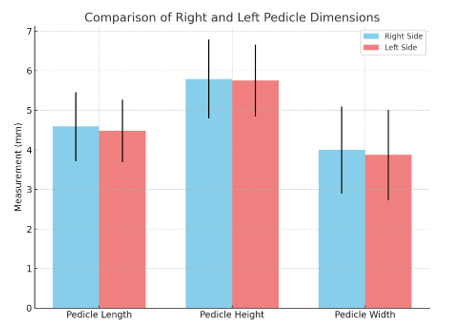
- Pedicle dimensions were recorded bilaterally. The right and left pedicle lengths were 4.59 ± 0.87 mm and 4.48 ± 0.79 mm, respectively.
- Pedicle height measured 5.79 ± 1.00 mm on the right and
- 5.75 ± 0.91 mm on the left. The width of the pedicle was 4.00
- Pedicle
- Mean±SD
- Range p-value
- Right
- 4.59±0.87
- 2.1-6.57
- Length
- 0.159
- Left
- 4.48±0.79
- 1.76-6.35
- Right
- 5.79±1
- 2.93-8.7
- Height
- 0.603
- Left
- 5.75±0.91
- 3.54-7.48
- Right
- 4±1.1
- 1.9-7.79
- Width
- 0.044
- Left
- 3.87±1.14
- 1.87-9.45
Table 1: Measurements of the Pedicle of the Typical Cervical Vertebrae.
| Vertebral Body | Mean±SD | Range |
|---|---|---|
| Vertebral Body Length | 14.55±2.14 | 10.24-21.67 |
| Vertebral Body Superior Width | 21.61±2.81 | 17.46-30.24 |
| Vertebral Body Inferior Width | 19.58±3.2 | 14.27-29.97 |
| Vertebral Body Anterior Height | 9.99±1.35 | 7.1-13.75 |
| Vertebral Body Posterior Height | 11.1±1.4 | 8.02-14.26 |
Table 2: Measurements of the Pedicle of the Typical Cervical Vertebrae.
± 1.10 mm on the right and 3.87 ± 1.14 mm on the left. A significant difference was found in width between the right and left pedicles (p = 0.044), while no statistically significant difference was noted in length or height (p > 0.05) (Tables 2 & 3) (Figures 9 & 10).
| Para-meter | Right (Mean ± SD) | Left (Mean ± SD) | t-value | df | p-value | Interp- retation |
|---|---|---|---|---|---|---|
| Pedicle Length (PL) | 4.59 ± 0.87 | 4.48 ± 0.79 | 2.34 | 99 | 0.021* | Significant difference |
| Pedicle Height (PH) | 5.79 ± 1.00 | 5.75 ± 0.91 | 0.49 | 99 | 0.624 | Not significant |
| Pedicle Width (PW) | 4.00 ± 1.10 | 3.87 ± 1.14 | 2.05 | 99 | 0.043* | Significant difference |
Table 3: Paired-Samples t-Test Results (Right vs. Left Pedicle Measurements). *Statistically significant at p < 0.05
Discussion
Vertebral Body Length
The present study found the mean vertebral body length to be 14.55 ± 2.14 mm, which is slightly lower than values reported in previous studies. Anderson, et al. [13] reported a mean of 15.2 mm from 53 cervical vertebrae, while Rao, et al. [1] found a mean length of 15.69 ± 1.42 mm based on 50 vertebrae. Bazaldúa, et al. [14, 15] observed a mean length of 14.68 ± 17.47 mm in 150 cervical vertebrae, and Polat, et al. [16] reported 14.79 ± 1.96 mm in 96 vertebrae. Similarly, Pramella, et al. [11] reported 14.79 ± 1.96 mm in their study of 100 vertebrae. The minor difference observed in the present study could be attributed to variations in ethnic backgrounds, environmental factors, and anatomical differences inherent to the sample population.
Vertebral Body Superior and Inferior Width
The present study found the mean superior vertebral body width (VBSW) to be 21.60 ± 2.81 mm, which was slightly lower than the findings of Cyriax [14] (20.94 mm in 42 vertebrae) and higher than the 21.49 ± 2.13 mm reported by Rao, et al. [1] for 50 vertebrae. On the other hand, Polat, et al. [16] reported a mean of 24.45 mm, and Pramella, et al. [11] noted 23.22 ± 2.16 mm in 100 cervical vertebrae. These differences could be explained by variations in the environments and ethnic backgrounds of the studied populations.
The mean inferior width (VBIW) in this study was 19.57 ± 3.19 mm, slightly lower than Pramella, et al. [11] findings of 19.88 ± 2.38 mm. These discrepancies might reflect differences in geographical regions and demographic factors among the studied populations (Table 4).
| Author | N | VBL | VBSW | VBIW | |||
|---|---|---|---|---|---|---|---|
| Mean & S.D | Range | Mean & S.D | Range | Mean & | Range | ||
| S.D | |||||||
| Anderson [12] | 53 | 15.2 | 14-16 | 19.9 | - | - | - |
| Cyriax [13] | 42 | - | 20.94 | - | - | - | |
| Rao et al. [1] | 50 | 15.69 ±1.42 | - | 21.49±2.13 | - | - | - |
| Bazaldúa, et al. [14] | 150 | 14.68-17.47 | - | 19.17-23.44 | - | - | - |
| Polat, et al. [15] | 96 | 14.03 | 10.50-20.00 | 24.45 | 17.30-32.00 | - | - |
| Pramella, et al. [10] | 100 | 14.79±1.96 | - | 23.22±2.16 | - | 19.88±2.38 | - |
| Present Study | 100 | 14.55±2.14 | 10.24-21.67 | 21.60±2.81 | 17.46-30.24 | 19.57±3.19 | 14.27-29.97 |
Table 4: Comparison of Vertebral Body Length (VBL), Vertebral Body Superior Width (VBSW), and Vertebral Body Inferior Width (VBIW
Vertebral Body Anterior and Posterior Height
The anterior vertebral body height (VBAH) in this study was 9.99 ± 1.35 mm, which is lower than the findings of Anderson [13] (12.4 mm), Cyriax [14] (12.85 mm), and Rao, et al. [1] (12.31 ± 1.58 mm). The smaller mean observed in our study could be attributed to anatomical or environmental differences in the populations studied. In addition, our study’s (VBPH) was higher than the VBAH, measuring 11.10±1.39mm. This shows that there may be the same inherent variance in the vertebrae’s size and form (Table 5).
| Various Authors conducted the study | N | VBAH (mm) | VBPH (mm) | ||
|---|---|---|---|---|---|
| Mean & S.D | Range | Mean & S.D | Range | ||
| Anderson [12] | 28 | 12.4 | Dec-13 | - | - |
| Cyriax [13] | 42 | 12.85 | Oct-16 | - | - |
| Rao, et al. [1] | 50 | 12.31±1.58 | - | - | - |
| Polat, et al. [15] | 96 | 10.64 | 3.50-20.00 | - | - |
| Pramella, et al. [10] | 100 | 10.92±1.35 | - | - | - |
| Present study | 100 | 9.99±1.35 | 7.10-13.75 | 11.10±1.39 | 8.02-14.26 |
Table 5: Comparison of Vertebral Body Anterior Height (VBAH), and Posterior Height (VBPH) of Typical Cervical Vertebrae. N= Numbe
Pedicle Dimensions
The mean pedicle length (PL) in this study was slightly lower than that reported by Pramella, et al. [11], though the difference was statistically insignificant (p-value > 0.05). This could be due to variations in ethnicity and lifestyle factors that influence skeletal morphology. Similarly, the mean pedicle height (PH) in this study was statistically significant (p-value > 0.05) when compared to the study by Pramella, et al., and was lower than the values they reported. For pedicle width (PW), the mean observed in our study was slightly higher than that of Polat, et al. [16], but lower than Bazaldúa, et al. [15] findings. These differences were statistically insignificant (p-value < 0.05), and could reflect the influence of local living conditions and environmental factors on vertebral morphology (Table 6).
| A study conducted by various Authors over and years | N | PL | PH | PW | ||||
|---|---|---|---|---|---|---|---|---|
| Mean (mm) & S.D | Range (mm) | Mean (mm) & S.D | Range (mm) | Mean (mm) & S.D | Range (mm) | |||
| Bazaldúa, et al. [14] | 150 | Rt/Lt | 4.75±1.11 | - | 6.95±1.25 | - | 4.75±1.33 | - |
| Polat, et al. [15] | 96 | Rt | 5.65±1.91 | 1.50- 11.00 | - | - | 3.72 | 1.50- 8.50 |
| Lt | 5.65±1.76 | 2.00- 10.50 | - | - | 3.61 | 1.00- 9.50 | ||
| Pramella, et al. [10] | 100 | Rt/Lt | 5.41±1.08 | - | 5.98±0.93 | - | 4.52 ± 0.84 | - |
| Present study | 100 | Rt | 4.58± .86 | 2.10-6.57 | 5.79± .99 | 2.93-8.70 | 3.99±1.09 | 1.90-7.79 |
| Lt | 4.47± .79 | 1.76-6.35 | 5.74± .90 | 3.54-7.48 | 3.86±1.13 | 1.87-9.45 |
Table 6: Comparison of Pedicle Length (PL), Pedicle Height (PH) & Pedicle Width (PW) of Typical Cervical Vertebrae. N= Number
Osteophytes and Clinical Implications
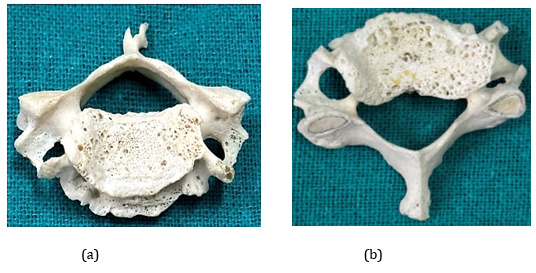
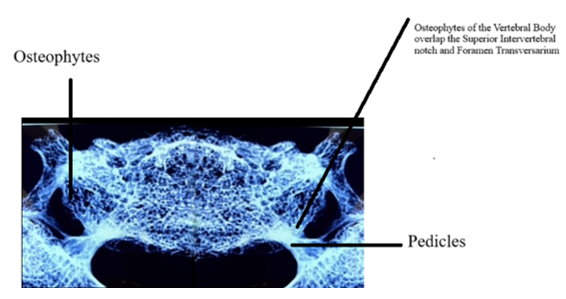
Osteophytes observed in this study were indicative of degenerative changes such as osteoarthritis, leading to stiffness and limited mobility in the neck [17]. These osteophytes also contribute to nerve entrapment syndromes due to narrowing of the superior intervertebral notch on the superior aspect of the pedicle [3]. Larger osteophytes can cause mechanical obstruction of the esophagus, resulting in dysphagia [5, 18], and may even contribute to conditions like sleep apnea [19]. Smaller osteophytes, particularly at the C5/C6 level, may compress the esophageal segment at the cricoid cartilage, causing difficulty in swallowing [5]. Furthermore, prolonged osteophyte growth can encroach on adjacent structures, contributing to clinical symptoms such as brachialgia, dysphagia, and vertebrobasilar insufficiency [20]. These findings underscore the importance of considering osteophyte formation in clinical evaluations of the cervical spine (Figure 11).
Conclusion
A comprehensive understanding of the morphometric features of the cervical vertebrae—including the pedicle, vertebral body, and associated neurovascular structures— can enhance the safety and accuracy of transpedicular screw placement. These measurements are also valuable for surgeons performing anterior cervical reconstruction, where the anteroposterior length of the vertebral body is a critical parameter for bicortical screw fixation [21]. From an anthropological perspective, the development of the vertebral body appears to be influenced by genetic, racial, postural, and occupational factors [21, 22]. While osteophyte formation is generally regarded as a pathological process, their presence on vertebral joint surfaces may serve a compensatory or adaptive function, contributing to spinal stability. Similar adaptive roles of osteophytes have been reported in other skeletal regions [23, 24].
In summary, the distribution of vertebral osteophytes in the cervical spine appears to be more closely associated with segmental mobility rather than axial loading. These
findings are not only clinically relevant but also contribute to our understanding of anatomical adaptation and spinal biomechanics.
Acknowledgments
The authors express their sincere gratitude to the individuals who donated their bodies for the advancement of anatomical science. The insights gained from such generous contributions deepen our understanding of human morphology and directly enhance clinical and surgical practice. We also extend our respect and appreciation to the donors’ families for supporting this invaluable contribution to medical education and research.
References
-
Rao KEV, Rao BS, Vinila BHS (2016) Morphometric analysis of typical cervical vertebrae and their clinical implications: A cross-sectional study. Int J Anat Res 4(4): 2988-2992.
-
Ezra D, Hershkovitz I, Salame K, Alperovitch-Najenson D, Slon V (2019) Osteophytes in the cervical vertebral bodies (C3–C7): Demographical perspectives. Anat Rec 302(2): 226-231.
-
Nathan H (1962) Osteophytes of the vertebral column: an anatomical study of their development according to age, race, and sex with consideration of their etiology and significance. J Bone Joint Surg Am 44(2): 243-268.
-
O’Neill TW, McCloskey EV, Kanis JA, Bhalla AK, Reeve J, et al. (1999) The distribution, determinants, and clinical correlates of vertebral osteophytosis: a population- based survey. J Rheumatol 26: 842-848.
-
Strasser G, Schima W, Schober E, Pokieser P, Kaider A, et al. (2000) Cervical osteophytes impinging on the pharynx: importance of size and concurrent disorders for development of aspiration. Am J Roentgenol 174(2): 449-453.
-
Hughes TA, Wiles CM, Lawrie BW, Smith AP (1994) Dysphagia and sleep apnoea associated with cervical osteophytes due to diffuse idiopathic skeletal hyperostosis (DISH). J Neurol Neurosurg Psychiatry 57(3): 384.
-
Nallan M, Thangavel M (2017) Morphometric analysis of typical cervical vertebral pedicle: an osteological study. Int J Orthop Sci 3(4): 704-708.
-
Kaur S, Lalit M, Mahajan A (2024) Study of morphometric analysis of foramen transversarium and uncinate process and clinical relevance in typical cervical vertebrae. J Hum Anat 8(1): 198.
-
Durga P, Dakshayani KR (2020) Morphometric study of uncinate process of cervical vertebra and its surgical importance. Natl J Clin Anat 9(2): 59-62.
-
Dhatt SS, Kumar V, Rijal S, Prakash M (2018) Morphometric analysis of cervical spine pedicles in an Indian population. J Spinal Disord Tech 5(1): 39-42.
-
Prameela MD, Prabhu LV, Murlimanju BV, Pai MM, Rai RL, et al. (2020) Anatomical dimensions of the typical cervical vertebrae and their clinical implications. Eur J Anat 24(1): 9-15.
-
Anson BJ, Rea RL (1996) Axial skeleton: cervical vertebrae. In: Anson BJ (Ed.), Morris’ Human Anatomy. 12th(Edn.), McGraw Hill, New York, pp: 142-147.
-
Anderson RE, Shealy CN (1970) Cervical pedicle erosion and rootlet compression caused by tortuous vertebral artery. Radiology 90: 537-538.
-
Cyriax EF (1920) On certain absolute and relative measurements of human vertebrae. J Anat 54(4): 305- 308.
-
Bazaldúa CJJ, González LA, Gómez SA, Villarreal SEE, Velázquez GSE, et al. (2011) Morphometric study of cervical vertebrae C3–C7 in a population from northeastern Mexico. Int J Morphol 29(2): 325-330.
-
Polat S, Göker P, Yücel AH, Bozkır MG (2019) Morphometric study of dry cervical vertebrae. Int J Morphol 37(3): 845-851.
-
Klaassen Z, Tubbs RS, Apaydin N, Hage R, Jordan R, et al. (2011) Vertebral spinal osteophytes. Anat Sci Int 86(1): 1-9.
-
Ozgocmen S, Kiris A, Kocakoc E, Ardicoglu O (2002) Osteophyte-induced dysphagia: report of three cases. Joint Bone Spine 69(2): 226-229.
-
Mahto AK, Omar S (2015) Clinico-anatomical approach for instrumentation of the cervical spine: a morphometric study on typical cervical vertebrae. Int J Sci Study 3(4): 143-145.
-
Chanapa P, Mahakkanukrauh P (2011) Locations and lengths of osteophytes in the cervical vertebrae. L Locations and length of osteophytes in the vertebra. Rev Arg Anat Clin 3(1): 15-21.
-
Matsukawa K, Yato Y, Imabayashi H (2020) Impact of screw diameter and length on pedicle screw fixation strength in osteoporotic vertebrae: a finite element analysis. Asian Spine J 15(5): 566-574.
-
Karami KJ, Buckenmeyer LE, Kiapour AM, Kelkar PS, Goel VK, et al. (2015) Biomechanical evaluation of the pedicle screw insertion depth effect on screw stability under cyclic loading and subsequent pullout. Clinical Spine Surgery 28: E133-E139.
-
Prabavathy G, Philip XC, Arthi G, Sadeesh T (2017) Morphometric study of cervical vertebrae C3–C7 in South Indian population: a clinico-anatomical approach. Ital J Anat Embryol 122(1): 49-57.
-
Perry GH, Smith MJ, Whiteside CG (1972) Spontaneous recovery of the joint space in degenerative hip disease. Ann Rheum Dis 31(6): 440-444.
- Pattern of Breast Lesions in Ovu Inland, Delta State, South Southern Nigeria
- Morphometric Analysis of the Human Femur: Exploring Platymetric and Robusticity Indices Among the Nigerian Population
- Anatomical Variation of Arteria Lusoria: Clinical Implications for Dysphagia Lusoria and Surgical Risk
- Epigenetic Mechanisms Driving Human Evolutionary Changes
- Neuroprotective Effects of Ginkgo Biloba Extract on Bilateral Common Carotid Artery Ischaemic Stroke Induced in Wistar Rat
- Communicating Neuroanatomical Fibers in Health and Diseases